

Managing Fetal Ovarian Cysts: Clinical Experience with a Rare Disorder
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
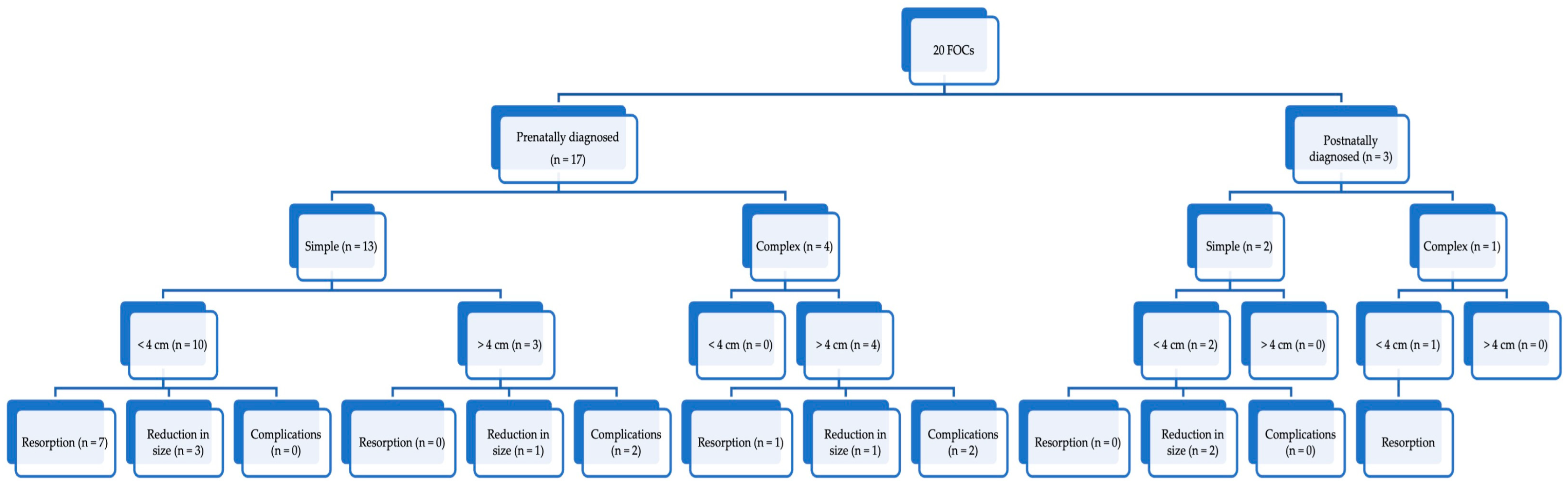
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bryant, A.E.; Laufer, M.R. Fetal ovarian cysts: Incidence, diagnosis and management. J. Reprod. Med. 2004, 49, 329–337. [Google Scholar]
- Brandt, M.L.; Helmrath, M.A. Ovarian cysts in infants and children. Semin. Pediatr. Surg. 2005, 14, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Amies Oelschlager, A.M.; Sawin, R. Teratomas and ovarian lesions in children. Surg. Clin. N. Am. 2012, 92, 599–613. [Google Scholar] [CrossRef]
- Nussbaum, A.R.; Sanders, R.C.; Hartman, D.S.; Dudgeon, D.L.; Parmley, T.H. Neonatal ovarian cysts: Sonographic-pathologic correlation. Radiology 1988, 168, 817–821. [Google Scholar] [CrossRef]
- Trinh, T.W.; Kennedy, A.M. Fetal ovarian cysts: Review of imaging spectrum, differential diagnosis, management, and outcome. Radiographics 2015, 35, 621–635. [Google Scholar] [CrossRef] [PubMed]
- Quarello, E.; Gorincour, G.; Merrot, T.; Boubli, L.; D’Ercole, C. The ‘daughter cyst sign’: A sonographic clue to the diagnosis of fetal ovarian cyst. Ultrasound Obstet. Gynecol. 2003, 22, 433–434. [Google Scholar] [CrossRef] [PubMed]
- Bascietto, F.; Liberati, M.; Marrone, L.; Khalil, A.; Pagani, G.; Gustapane, S.; Leombroni, M.; Buca, D.; Flacco, M.E.; Rizzo, G.; et al. Outcome of fetal ovarian cysts diagnosed on prenatal ultrasound examination: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2017, 50, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Toker Kurtmen, B.; Divarci, E.; Ergun, O.; Ozok, G.; Celik, A. The Role of Surgery in Antenatal Ovarian Torsion: Retrospective Evaluation of 28 Cases and Review of the Literature. J. Pediatr. Adolesc. Gynecol. 2022, 35, 18–22. [Google Scholar] [CrossRef]
- Chen, L.; Hu, Y.; Hu, C.; Wen, H. Prenatal evaluation and postnatal outcomes of fetal ovarian cysts. Prenat. Diagn. 2020, 40, 1258–1264. [Google Scholar] [CrossRef] [PubMed]
- Akın, M.A.; Akın, L.; Özbek, S.; Tireli, G.; Kavuncuoğlu, S.; Sander, S.; Akçakuş, M.; Güneş, T.; Öztürk, M.A.; Kurtoğlu, S. Fetal-neonatal ovarian cysts--their monitoring and management: Retrospective evaluation of 20 cases and review of the literature. J. Clin. Res. Pediatr. Endocrinol. 2010, 2, 28–33. [Google Scholar] [CrossRef]
- Jeanty, C.; Frayer, E.A.; Page, R.; Langenburg, S. Neonatal ovarian torsion complicated by intestinal obstruction and perforation, and review of the literature. J. Pediatr. Surg. 2010, 45, e5–e9. [Google Scholar] [CrossRef] [PubMed]
- Cass, D.L. Fetal abdominal tumors and cysts. Transl. Pediatr. 2021, 10, 1530–1541. [Google Scholar] [CrossRef] [PubMed]
- Bucuri, C.; Mihu, D.; Malutan, A.; Oprea, V.; Berceanu, C.; Nati, I.; Rada, M.; Ormindean, C.; Blaga, L.; Ciortea, R. Fetal Ovarian Cyst-A Scoping Review of the Data from the Last 10 Years. Medicina 2023, 59, 186. [Google Scholar] [CrossRef]
- Bagolan, P.; Giorlandino, C.; Nahom, A.; Bilancioni, E.; Trucchi, A.; Gatti, C.; Aleandri, V.; Spina, V. The management of fetal ovarian cysts. J. Pediatr. Surg. 2002, 37, 25–30. [Google Scholar] [CrossRef]
- Akalin, M.; Demirci, O.; Dayan, E.; Odacilar, A.S.; Ocal, A.; Celayir, A. Natural history of fetal ovarian cysts in the prenatal and postnatal periods. J. Clin. Ultrasound. 2021, 49, 822–827. [Google Scholar] [CrossRef]
- Lewis, S.; Walker, J.; McHoney, M. Antenatally detected abdominal cyst: Does cyst size and nature determine postnatal symptoms and outcome? Early Hum. Dev. 2020, 147, 105102. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, H.N.; Balci, S.; Ekinci, S.; Gunes, A.; Oguz, B.; Ciftci, A.O.; Haliloglu, M. Imaging Findings of Fetal-Neonatal Ovarian Cysts Complicated with Ovarian Torsion and Autoamputation. AJR Am. J. Roentgenol. 2015, 205, 185–189. [Google Scholar] [CrossRef]
- Zampieri, N.; Borruto, F.; Zamboni, C.; Camoglio, F.S. Foetal and neonatal ovarian cysts: A 5-year experience. Arch. Gynecol. Obstet. 2008, 277, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Souganidis, E.; Chen, A.; Friedlaender, E. Symptomatic Persistent Fetal Ovarian Cysts. Pediatr. Emerg. Care. 2021, 37, e672–e674. [Google Scholar] [CrossRef]
- Cheng, Y. Ovarian cysts. Am. J. Obstet. Gynecol. 2021, 225, B23–B25. [Google Scholar] [CrossRef]
- Filip, C.; Socolov, D.G.; Albu, E.; Filip, C.; Serban, R.; Popa, R.F. Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review. Medicina 2021, 57, 160. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, A.E.; Fallat, M.E.; Hewitt, G.; Hertweck, P.; Onwuka, A.; Afrazi, A.; Bence, C.; Burns, R.C.; Corkum, K.S.; Dillon, P.A.; et al. Understanding the Value of Tumor Markers in Pediatric Ovarian Neoplasms. J. Pediatr. Surg. 2020, 55, 122–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotar, I.C.; Tudorache, S.; Staicu, A.; Popa-Stanila, R.; Constantin, R.; Surcel, M.; Zaharie, G.C.; Mureşan, D. Fetal Ovarian Cysts: Prenatal Diagnosis Using Ultrasound and MRI, Management and Postnatal Outcome-Our Centers Experience. Diagnostics 2021, 12, 89. [Google Scholar] [CrossRef]
- Nemec, U.; Nemec, S.F.; Bettelheim, D.; Brugger, P.C.; Horcher, E.; Schöpf, V.; Graham, J.M., Jr.; Rimoin, D.L.; Weber, M.; Prayer, D. Ovarian cysts on prenatal MRI. Eur. J. Radiol. 2012, 81, 1937–1944. [Google Scholar] [CrossRef]
- Norton, M.E.; Cheng, Y.; Chetty, S.; Chyu, J.K.; Connolly, K.; Ghaffari, N.; Hopkins, L.M.; Jelin, A.; Mardy, A.; Osmundson, S.S.; et al. SMFM Fetal Anomalies Consult Series #4: Genitourinary anomalies. Am. J. Obstet. Gynecol. 2021, 225, B2–B35. [Google Scholar] [PubMed]
- Hara, T.; Mimura, K.; Endo, M.; Fujii, M.; Matsuyama, T.; Yagi, K.; Kawanishi, Y.; Tomimatsu, T.; Kimura, T. Diagnosis, Management, and Therapy of Fetal Ovarian Cysts Detected by Prenatal Ultrasonography: A Report of 36 Cases and Literature Review. Diagnostics 2021, 11, 2224. [Google Scholar] [CrossRef] [PubMed]
- Słodki, M.; Respondek-Liberska, M. Fetal ovarian cysts—420 cases from literature—Metaanalysis 1984–2005. Ginekol. Pol. 2007, 78, 324–328. [Google Scholar] [PubMed]
- Senarath, S.; Ades, A.; Nanayakkara, P. Ovarian cysts in pregnancy: A narrative review. J. Obstet. Gynaecol. 2021, 41, 169–175. [Google Scholar] [CrossRef]
- Papic, J.C.; Billmire, D.F.; Rescorla, F.J.; Finnell, S.M.; Leys, C.M. Management of neonatal ovarian cysts and its effect on ovarian preservation. J. Pediatr. Surg. 2014, 49, 990–993; discussion 993–994. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.A.; Zahra, F.; Razianti Zb, C.; Kharismawati, N.; Sutjighassani, T.; Almira, N.L.; Tjandraprawira, K.D. Challenges in prenatal diagnosis of foetal anorectal malformation and hydrocolpos—Case report. Ann. Med. Surg. 2022, 84, 104949. [Google Scholar] [CrossRef]
- Dolgin, S.E. Ovarian masses in the newborn. Semin. Pediatr. Surg. 2000, 9, 121–127. [Google Scholar] [CrossRef]
- Croitoru, D.P.; Aaron, L.E.; Laberge, J.M.; Neilson, I.R.; Guttman, F.M. Management of complex ovarian cysts presenting in the first year of life. J. Pediatr. Surg. 1991, 26, 1366–1368. [Google Scholar] [CrossRef]
- Strickland, J.L. Ovarian cysts in neonates, children and adolescents. Curr. Opin. Obstet. Gynecol. 2002, 14, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Luzzatto, C.; Midrio, P.; Toffolutti, T.; Suma, V. Neonatal ovarian cysts: Management and follow-up. Pediatr. Surg. Int. 2000, 16, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Enríquez, G.; Durán, C.; Torán, N.; Piqueras, J.; Gratacós, E.; Aso, C.; Lloret, J.; Castellote, A.; Lucaya, J. Conservative versus surgical treatment for complex neonatal ovarian cysts: Outcomes study. AJR Am. J. Roentgenol. 2005, 185, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Diguisto, C.; Winer, N.; Benoist, G.; Laurichesse-Delmas, H.; Potin, J.; Binet, A.; Lardy, H.; Morel, B.; Perrotin, F. In-utero aspiration vs expectant management of anechoic fetal ovarian cysts: Open randomized controlled trial. Ultrasound Obstet. Gynecol. 2018, 52, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyraskis, A.; Bakalis, S.; David, A.L.; Eaton, S.; De Coppi, P. A systematic review and meta-analysis on fetal ovarian cysts: Impact of size, appearance and prenatal aspiration. Prenat. Diagn. 2017, 37, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Heling, K.S.; Chaoui, R.; Kirchmair, F.; Stadie, S.; Bollmann, R. Fetal ovarian cysts: Prenatal diagnosis, management and postnatal outcome. Ultrasound Obstet. Gynecol. 2002, 20, 47–50. [Google Scholar] [CrossRef]
- Dimitraki, M.; Koutlaki, N.; Nikas, I.; Mandratzi, T.; Gourovanidis, V.; Kontomanolis, E.; Zervoudis, S.; Galazios, G.; Liberis, V. Fetal ovarian cysts. Our clinical experience over 16 cases and review of the literature. J. Matern Fetal Neonatal. Med. 2012, 25, 222–225. [Google Scholar] [CrossRef]
- Tyraskis, A.; Bakalis, S.; Scala, C.; Syngelaki, A.; Giuliani, S.; Davenport, M.; David, A.L.; Nicolaides, K.; Eaton, S.; De Coppi, P. A retrospective multicenter study of the natural history of fetal ovarian cysts. J. Pediatr. Surg. 2018, 53, 2019–2022. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parameter | Simple Cyst n = 15 | Complex Cyst n = 5 | p Value |
|---|---|---|---|
| Mother’s age (years) | 26.1 ± 2.7 | 34 ± 2.1 | <0.001 |
| Gestation | 1.9 ± 0.5 | 1.6 ± 1.1 | 0.40 |
| Nulliparity (%) | Yes = 6 (40%) | Yes = 3 (60%) | 0.43 |
| GA at birth (weeks) | 39 ± 0.36 | 37.2 ± 4.33 | 0.10 |
| Type of birth (n/%) | Cesarean: 11 (73.3%) Vaginal: 4 (26.7%) | Cesarean: 3 (60%) Vaginal: 2 (40%) | 0.57 |
| Birthweight (g) | 3374.54 ± 212.99 | 3080 ± 141.76 | 0.01 |
| Apgar score at 1 min (mean ± SD) | 8.64 ± 1.68 | 8.19 ± 1.93 | 0.14 |
| Preterm birth (n/%) | Yes = 0% | Yes = 1 (20%) | 0.07 |
| Cyst location | Right: n = 10 (66.7%) Left: n = 4 (26.7%) Bilateral: n = 1 (6.7%) | Right: n = 4 (80%) Left: n = 1 (20%) Bilateral: n = 0 (0%) | 0.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melinte-Popescu, A.-S.; Popa, R.-F.; Harabor, V.; Nechita, A.; Harabor, A.; Adam, A.-M.; Vasilache, I.-A.; Melinte-Popescu, M.; Vaduva, C.; Socolov, D. Managing Fetal Ovarian Cysts: Clinical Experience with a Rare Disorder. Medicina 2023, 59, 715. https://doi.org/10.3390/medicina59040715
Melinte-Popescu A-S, Popa R-F, Harabor V, Nechita A, Harabor A, Adam A-M, Vasilache I-A, Melinte-Popescu M, Vaduva C, Socolov D. Managing Fetal Ovarian Cysts: Clinical Experience with a Rare Disorder. Medicina. 2023; 59(4):715. https://doi.org/10.3390/medicina59040715
Chicago/Turabian StyleMelinte-Popescu, Alina-Sinziana, Radu-Florin Popa, Valeriu Harabor, Aurel Nechita, AnaMaria Harabor, Ana-Maria Adam, Ingrid-Andrada Vasilache, Marian Melinte-Popescu, Cristian Vaduva, and Demetra Socolov. 2023. "Managing Fetal Ovarian Cysts: Clinical Experience with a Rare Disorder" Medicina 59, no. 4: 715. https://doi.org/10.3390/medicina59040715