
Tinnitus Prevalence in the Adult Population—Results from the Gutenberg Health Study

Abstract
:1. Introduction
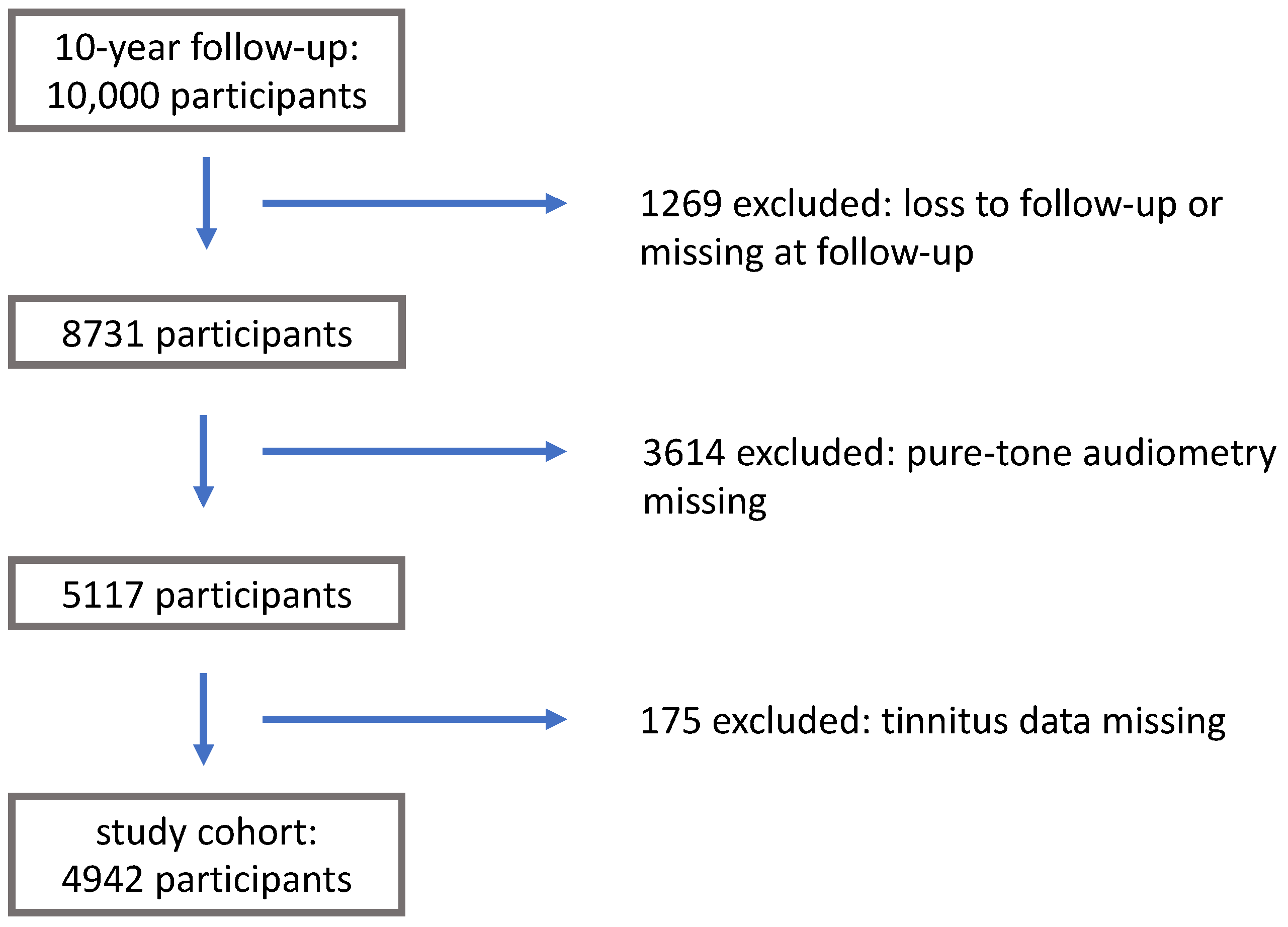
2. Materials and Methods
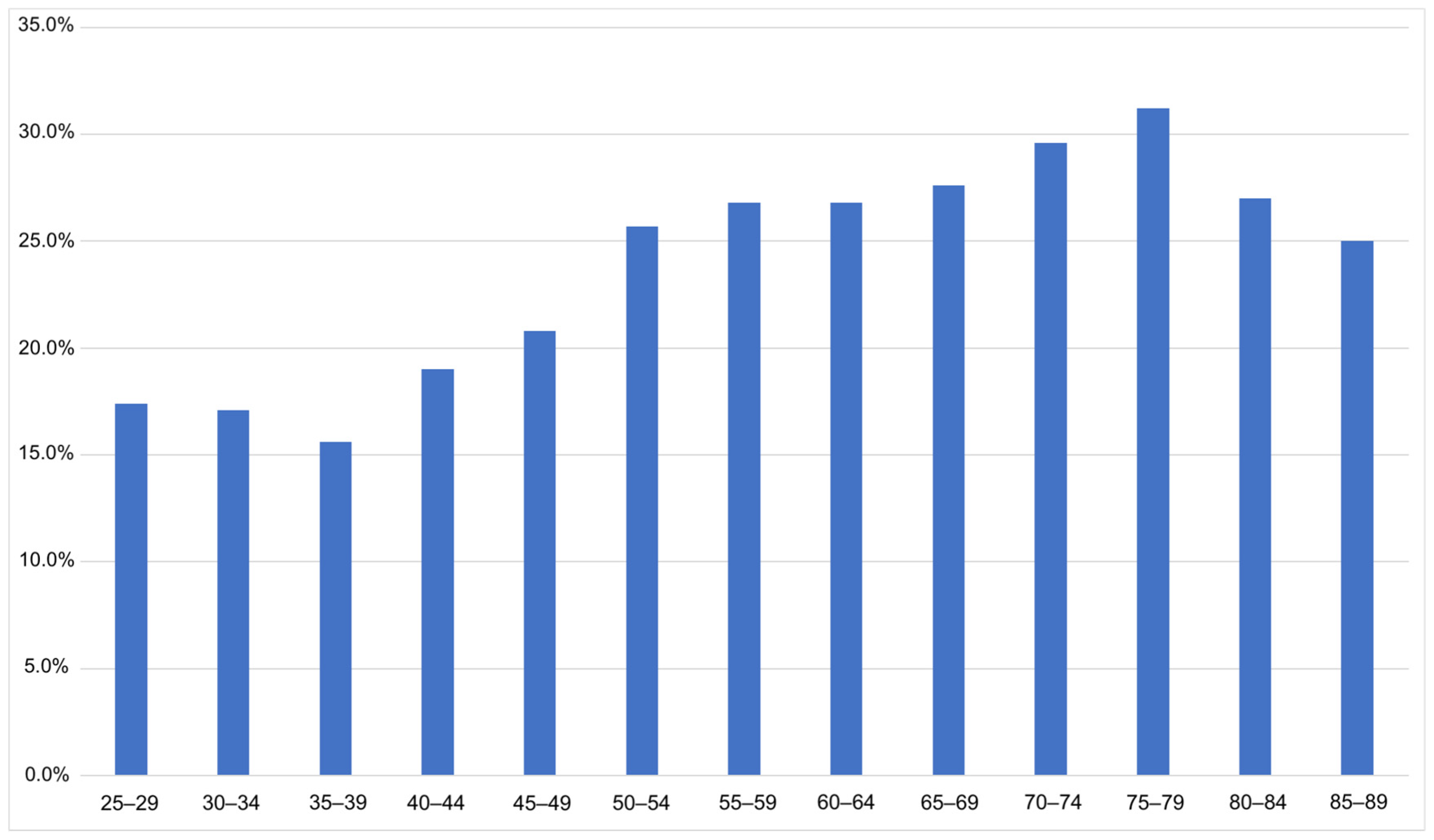
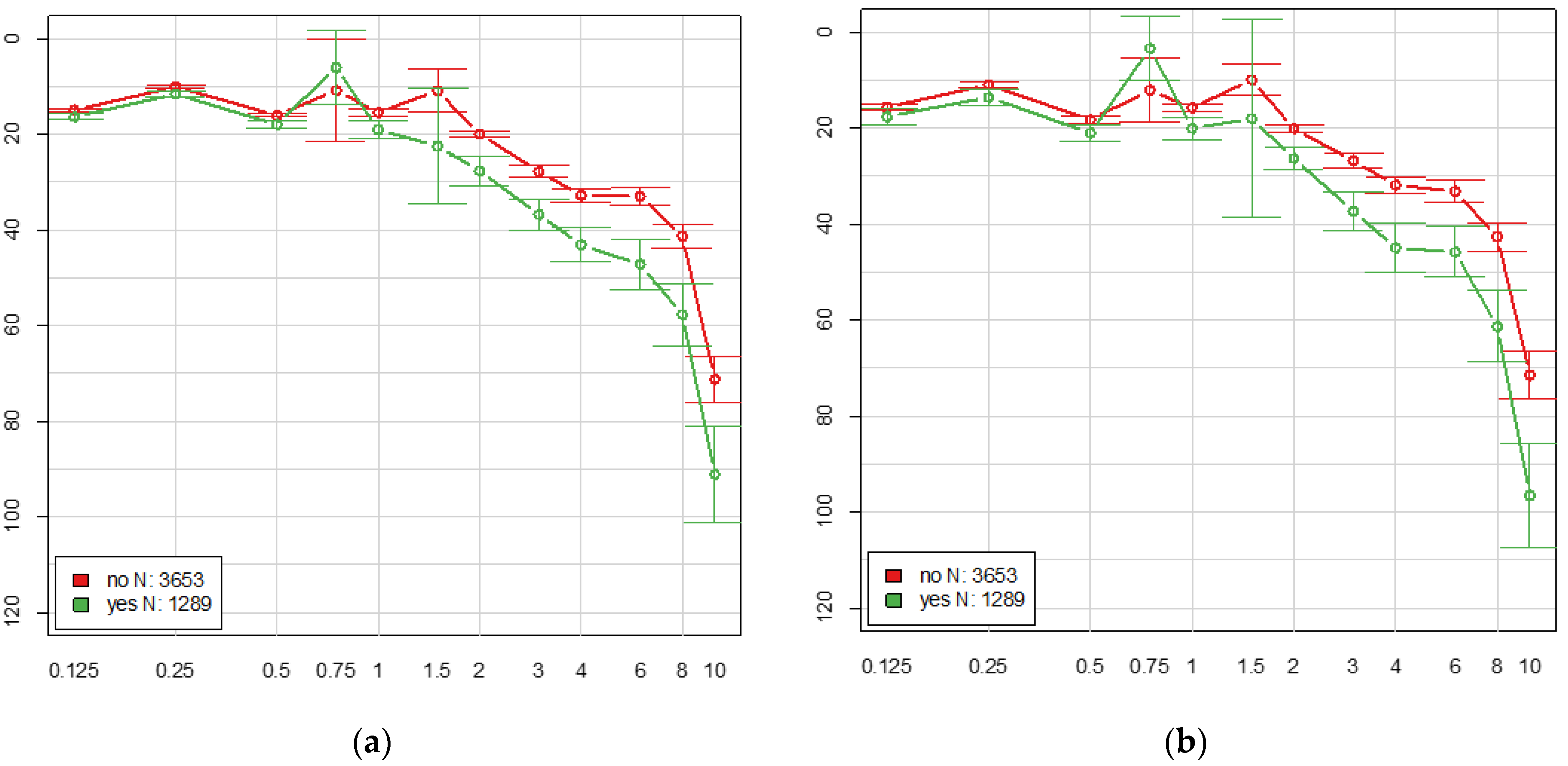
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heller, A.J. Classification and epidemiology of tinnitus. Otolaryngol. Clin. N. Am. 2003, 36, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Widén, S.E.; Erlandsson, S.I. Self-reported tinnitus and noise sensitivity among adolescents in Sweden. Noise Health 2004, 7, 29–40. [Google Scholar] [PubMed]
- Hannula, S.; Bloigu, R.; Majamaa, K.; Sorri, M.; Mäki-Torkko, E. Self-reported hearing problems among older adults: Prevalence and comparison to measured hearing impairment. J. Am. Acad. Audiol. 2011, 22, 550–559. [Google Scholar] [CrossRef]
- Biswas, R.; Lugo, A.; Akeroyd, M.A.; Schlee, W.; Gallus, S.; Hall, D.A. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg. Health Eur. 2022, 12, 100250. [Google Scholar] [CrossRef]
- Jarach, C.M.; Lugo, A.; Scala, M.; van den Brandt, P.A.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef]
- Axelsson, A.; Ringdahl, A. Tinnitus—A study of its prevalence and characteristics. Br. J. Audiol. 1989, 23, 53–62. [Google Scholar] [CrossRef]
- Davis, A.C. The prevalence of hearing impairment and reported hearing disability among adults in Great Britain. Int. J. Epidemiol. 1989, 18, 911–917. [Google Scholar] [CrossRef]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef]
- Park, R.J.; Moon, J.D. Prevalence and risk factors of tinnitus: The Korean National Health and Nutrition Examination Survey 2010-2011, a cross-sectional study. Clin. Otolaryngol. 2014, 39, 89–94. [Google Scholar] [CrossRef]
- Noreña, A.J.; Eggermont, J.J. Changes in spontaneous neural activity immediately after an acoustic trauma: Implications for neural correlates of tinnitus. Hear. Res. 2003, 183, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, P.J.; Hazell, J.W.; Graham, R.L. Neurophysiological model of tinnitus: Dependence of the minimal masking level on treatment outcome. Hear. Res. 1994, 80, 216–232. [Google Scholar] [CrossRef] [PubMed]
- Jastreboff, P.J.; Gray, W.C.; Gold, S.L. Neurophysiological approach to tinnitus patients. Am. J. Otol. 1996, 17, 236–240. [Google Scholar] [PubMed]
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus. Trends Neurosci. 2004, 27, 676–682. [Google Scholar] [CrossRef]
- Noreña, A.J. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci. Biobehav. Rev. 2011, 35, 1089–1109. [Google Scholar] [CrossRef]
- De Ridder, D.; Elgoyhen, A.B.; Romo, R.; Langguth, B. Phantom percepts: Tinnitus and pain as persisting aversive memory networks. Proc. Natl. Acad. Sci. USA 2011, 108, 8075–8080. [Google Scholar] [CrossRef] [Green Version]
- Jastreboff, P.J. Phantom auditory perception (tinnitus): Mechanisms of generation and perception. Neurosci. Res. 1990, 8, 221–254. [Google Scholar] [CrossRef] [PubMed]
- Czornik, M.; Malekshahi, A.; Mahmoud, W.; Wolpert, S.; Birbaumer, N. Psychophysiological treatment of chronic tinnitus: A review. Clin. Psychol. Psychother. 2022, 29, 1236–1253. [Google Scholar] [CrossRef]
- Van de Heyning, P.; Vermeire, K.; Diebl, M.; Nopp, P.; Anderson, I.; De Ridder, D. Incapacitating unilateral tinnitus in single-sided deafness treated by cochlear implantation. Ann. Otol. Rhinol. Laryngol. 2008, 117, 645–652. [Google Scholar] [CrossRef]
- Baguley, D.M.; Atlas, M.D. Cochlear implants and tinnitus. Prog. Brain Res. 2007, 166, 347–355. [Google Scholar] [CrossRef]
- Schaette, R.; König, O.; Hornig, D.; Gross, M.; Kempter, R. Acoustic stimulation treatments against tinnitus could be most effective when tinnitus pitch is within the stimulated frequency range. Hear. Res. 2010, 269, 95–101. [Google Scholar] [CrossRef] [PubMed]
- McNeill, C.; Távora-Vieira, D.; Alnafjan, F.; Searchfield, G.D.; Welch, D. Tinnitus pitch, masking, and the effectiveness of hearing aids for tinnitus therapy. Int. J. Audiol. 2012, 51, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Engdahl, B.; Krog, N.H.; Kvestad, E.; Hoffman, H.J.; Tambs, K. Occupation and the risk of bothersome tinnitus: Results from a prospective cohort study (HUNT). BMJ Open 2012, 2, e000512. [Google Scholar] [CrossRef]
- Johansson, M.S.; Arlinger, S.D. Prevalence of hearing impairment in a population in Sweden. Int. J. Audiol. 2003, 42, 18–28. [Google Scholar] [CrossRef]
- Hannaford, P.C.; Simpson, J.A.; Bisset, A.F.; Davis, A.; McKerrow, W.; Mills, R. The prevalence of ear, nose and throat problems in the community: Results from a national cross-sectional postal survey in Scotland. Fam. Pract. 2005, 22, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Louw, C.; Swanepoel, W.; Eikelboom, R.H. Self-Reported Hearing Loss and Pure Tone Audiometry for Screening in Primary Health Care Clinics. J. Prim. Care Community Health 2018, 9, 2150132718803156. [Google Scholar] [CrossRef] [PubMed]
- Hackenberg, B.; Döge, J.; Lackner, K.J.; Beutel, M.E.; Münzel, T.; Pfeiffer, N.; Nagler, M.; Schmidtmann, I.; Wild, P.S.; Matthias, C.; et al. Hearing Loss and Its Burden of Disease in a Large German Cohort-Hearing Loss in Germany. Laryngoscope 2021, 132, 1843–1849. [Google Scholar] [CrossRef]
- Wild, P.S.; Zeller, T.; Beutel, M.; Blettner, M.; Dugi, K.A.; Lackner, K.J.; Pfeiffer, N.; Münzel, T.; Blankenberg, S. The Gutenberg Health Study. Bundesgesundheitsblatt Gesundh. Gesundh. 2012, 55, 824–829. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Hearing. Available online: https://www.who.int/publications/i/item/world-report-on-hearing (accessed on 7 August 2021).
- European Commission. Eurostat Revision of the European Standard Population. Available online: https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF/e713fa79-1add-44e8-b23d-5e8fa09b3f8f (accessed on 21 April 2021).
- Khedr, E.M.; Ahmed, M.A.; Shawky, O.A.; Mohamed, E.S.; El Attar, G.S.; Mohammad, K.A. Epidemiological study of chronic tinnitus in Assiut, Egypt. Neuroepidemiology 2010, 35, 45–52. [Google Scholar] [CrossRef]
- Welch, D.; Dawes, P.J. Personality and perception of tinnitus. Ear Hear. 2008, 29, 684–692. [Google Scholar] [CrossRef]
- Baigi, A.; Oden, A.; Almlid-Larsen, V.; Barrenäs, M.L.; Holgers, K.M. Tinnitus in the general population with a focus on noise and stress: A public health study. Ear Hear. 2011, 32, 787–789. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.S.; Choi, S.H.; Park, K.H.; Park, H.J.; Kim, J.W.; Moon, I.J.; Rhee, C.S.; Kim, K.S.; Sun, D.I.; Lee, S.H.; et al. Prevalence of otolaryngologic diseases in South Korea: Data from the Korea national health and nutrition examination survey 2008. Clin. Exp. Otorhinolaryngol. 2010, 3, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Dawes, P.; Fortnum, H.; Moore, D.R.; Emsley, R.; Norman, P.; Cruickshanks, K.; Davis, A.; Edmondson-Jones, M.; McCormack, A.; Lutman, M.; et al. Hearing in middle age: A population snapshot of 40- to 69-year olds in the United Kingdom. Ear Hear. 2014, 35, e44–e51. [Google Scholar] [CrossRef] [Green Version]
- Demeester, K.; van Wieringen, A.; Hendrickx, J.J.; Topsakal, V.; Fransen, E.; Van Laer, L.; De Ridder, D.; Van Camp, G.; Van de Heyning, P. Prevalence of tinnitus and audiometric shape. B-ENT 2007, 3 (Suppl. 7), 37–49. [Google Scholar] [PubMed]
- Gibrin, P.C.; Melo, J.J.; Marchiori, L.L. Prevalence of tinnitus complaints and probable association with hearing loss, diabetes mellitus and hypertension in elderly. Codas 2013, 25, 176–180. [Google Scholar] [CrossRef] [Green Version]
- Kuttila, S.; Kuttila, M.; Le Bell, Y.; Alanen, P.; Suonpää, J. Recurrent tinnitus and associated ear symptoms in adults. Int. J. Audiol. 2005, 44, 164–170. [Google Scholar] [CrossRef]
- Michikawa, T.; Nishiwaki, Y.; Kikuchi, Y.; Saito, H.; Mizutari, K.; Okamoto, M.; Takebayashi, T. Prevalence and factors associated with tinnitus: A community-based study of Japanese elders. J. Epidemiol. 2010, 20, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Oiticica, J.; Bittar, R.S. Tinnitus prevalence in the city of São Paulo. Braz. J. Otorhinolaryngol. 2015, 81, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Park, K.H.; Lee, S.H.; Koo, J.W.; Park, H.Y.; Lee, K.Y.; Choi, Y.S.; Oh, K.W.; Lee, A.; Yang, J.E.; Woo, S.Y.; et al. Prevalence and associated factors of tinnitus: Data from the Korean National Health and Nutrition Examination Survey 2009–2011. J. Epidemiol. 2014, 24, 417–426. [Google Scholar] [CrossRef] [Green Version]
- Sindhusake, D.; Mitchell, P.; Newall, P.; Golding, M.; Rochtchina, E.; Rubin, G. Prevalence and characteristics of tinnitus in older adults: The Blue Mountains Hearing Study. Int. J. Audiol. 2003, 42, 289–294. [Google Scholar] [CrossRef]
- Parving, A.; Hein, H.O.; Suadicani, P.; Ostri, B.; Gyntelberg, F. Epidemiology of hearing disorders. Some factors affecting hearing. The Copenhagen Male Study. Scand. Audiol. 1993, 22, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Oosterloo, B.C.; Croll, P.H.; Baatenburg de Jong, R.J.; Ikram, M.K.; Goedegebure, A. Prevalence of Tinnitus in an Aging Population and Its Relation to Age and Hearing Loss. Otolaryngol. Head Neck Surg. 2021, 164, 859–868. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Pilgram, M.; Rychlik, R.; Lebisch, H.; Goebel, G.; Kirchhof, D. Tinnitus in der Bundesrepublik Deutschland - eine repräsentative epidemiologische Studie. HNO Aktuell 1999, 7, 261–265. [Google Scholar]
- Hesse, G.; Kastellis, G.; Mazurek, B. S3-Leitlinie zu chronischem Tinnitus überarbeitet. Was derzeit zu Diagnostik und Therapie empfohlen wird und was nicht. HNO Nachr. 2022, 52, 32–37. [Google Scholar] [CrossRef]
- Hackenberg, B.; Döge, J.; O’Brien, K.; Bohnert, A.; Lackner, K.J.; Beutel, M.E.; Michal, M.; Münzel, T.; Wild, P.S.; Pfeiffer, N.; et al. Tinnitus and Its Relation to Depression, Anxiety, and Stress-A Population-Based Cohort Study. J. Clin. Med. 2023, 12, 1169. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Men | Women | p-Value | |
|---|---|---|---|---|
| n | 4942 | 2550 | 2392 | |
| age, mean (SD) | 61.0 (13.3) | 61.8 (13.4) | 60.2 (13.2) | <0.0001 * |
| tinnitus (yes) | 26.1% | 30.2% | 21.7% | <0.0001 * |
| burden due to tinnitus, mean (SD) | 2.39 (1.26) | 2.30 (1.22) | 2.51 (1.31) | 0.0039 * |
| annoying tinnitus (burden of 3–6) | 9.8% | 10.8% | 8.8% | 0.0233 * |
| WHO Hearing Impairment | Audiometric Value (Average across 0.5/1/2/4 kHz, Better Ear) | Tinnitus Prevalence [95% CI] |
|---|---|---|
| No impairment | <20 dB | 21.6% [20.1%;23.1%] |
| Mild impairment | 20–34.9 dB | 31.2% [28.8%;33.8%] |
| Moderate impairment | 35–49.9 dB | 34.2% [30.0%;38.7%] |
| Moderately severe impairment | 50–64.9 dB | 38.5% [29.2%;48.5%] |
| Severe impairment | 65–79.9 dB | 78.6% [48.8%;94.3%] |
| Profound impairment | 80–94.9 dB | 0% |
| Complete impairment | ≥95 dB | 42.9% [11.8%;79.8%] |
| Variable | OR | 2.5% | 97.5% | p | Events | n | z-Score | Nagelkerke R2 |
|---|---|---|---|---|---|---|---|---|
| 1289 | 4941 | 0.036 | ||||||
| Sex (female) | 0.67 | 0.59 | 0.77 | <0.001 | 519 | 2392 | −5.986 | |
| Age (per year) | 1.00 | 1.00 | 1.01 | 0.55 | 0.545 | |||
| Mild to moderately severe hearing impairment * | 1.63 | 1.39 | 1.39 | <0.001 | 641 | 1981 | 5.963 | |
| Severe to complete hearing impairment * | 6.09 | 2.52 | 14.72 | <0.001 | 14 | 22 | 4.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hackenberg, B.; O’Brien, K.; Döge, J.; Lackner, K.J.; Beutel, M.E.; Münzel, T.; Pfeiffer, N.; Schulz, A.; Schmidtmann, I.; Wild, P.S.; et al. Tinnitus Prevalence in the Adult Population—Results from the Gutenberg Health Study. Medicina 2023, 59, 620. https://doi.org/10.3390/medicina59030620
Hackenberg B, O’Brien K, Döge J, Lackner KJ, Beutel ME, Münzel T, Pfeiffer N, Schulz A, Schmidtmann I, Wild PS, et al. Tinnitus Prevalence in the Adult Population—Results from the Gutenberg Health Study. Medicina. 2023; 59(3):620. https://doi.org/10.3390/medicina59030620
Chicago/Turabian StyleHackenberg, Berit, Karoline O’Brien, Julia Döge, Karl J. Lackner, Manfred E. Beutel, Thomas Münzel, Norbert Pfeiffer, Andreas Schulz, Irene Schmidtmann, Philipp S. Wild, and et al. 2023. "Tinnitus Prevalence in the Adult Population—Results from the Gutenberg Health Study" Medicina 59, no. 3: 620. https://doi.org/10.3390/medicina59030620