
Pre-Test Probability Assessment and d-Dimer Based Evaluation in Patients with Previous Acute Aortic Syndrome
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Patient Selection
2.3. Advanced Imaging
2.4. d-Dimer Assay
2.5. Pretest Probability Assessment
2.6. Final Adjudication
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Pretest Probability Assessment
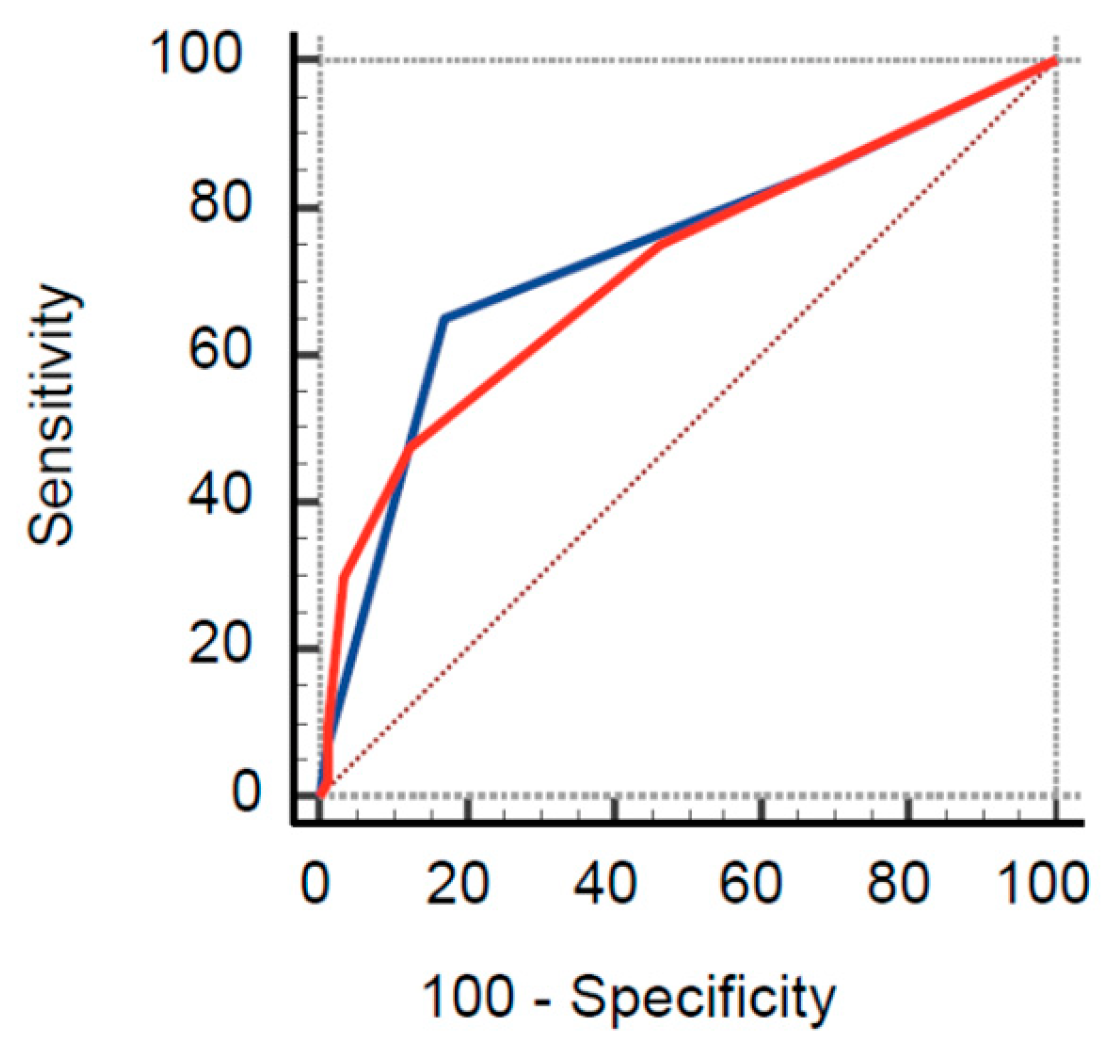
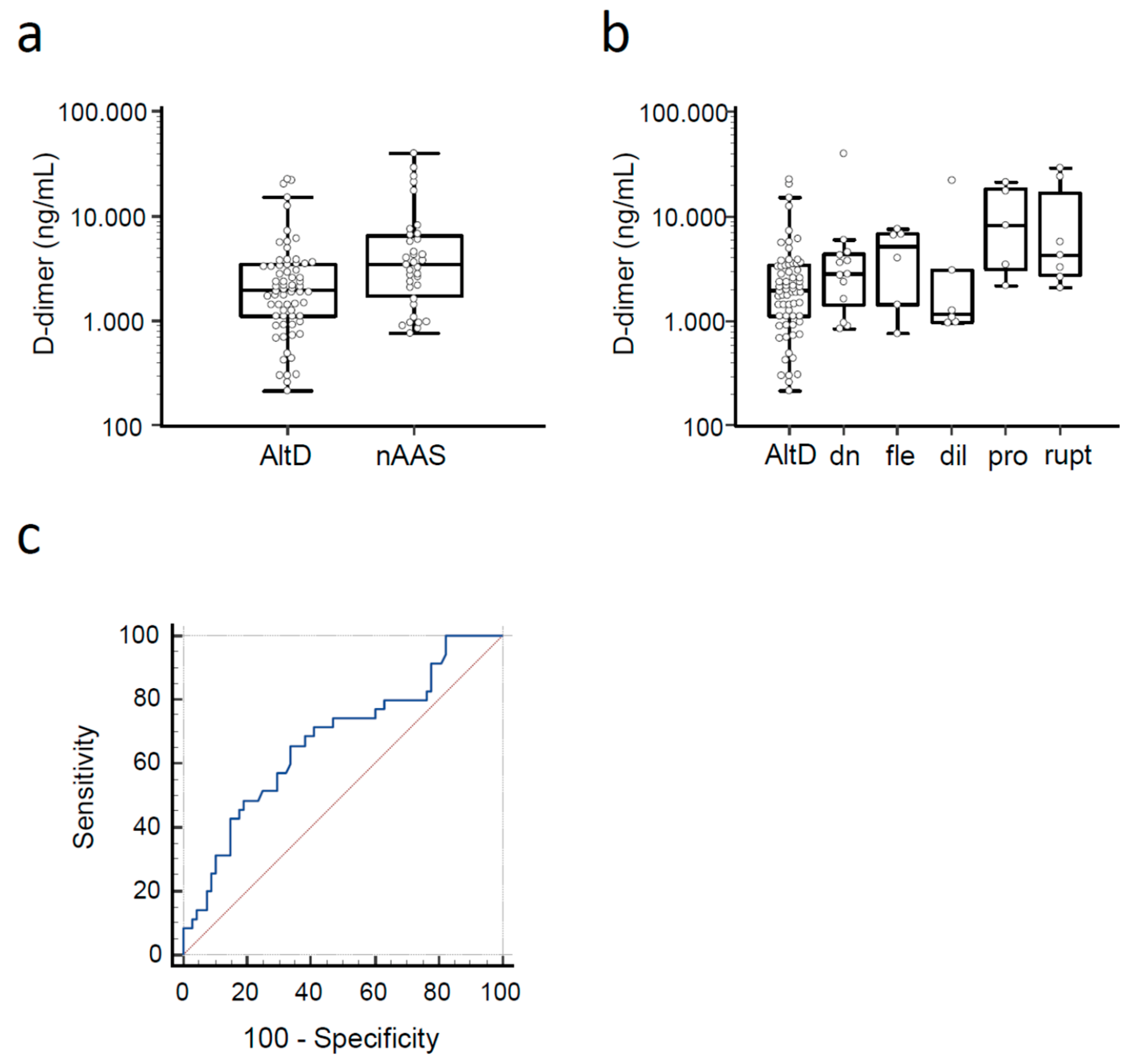
3.3. d-Dimer
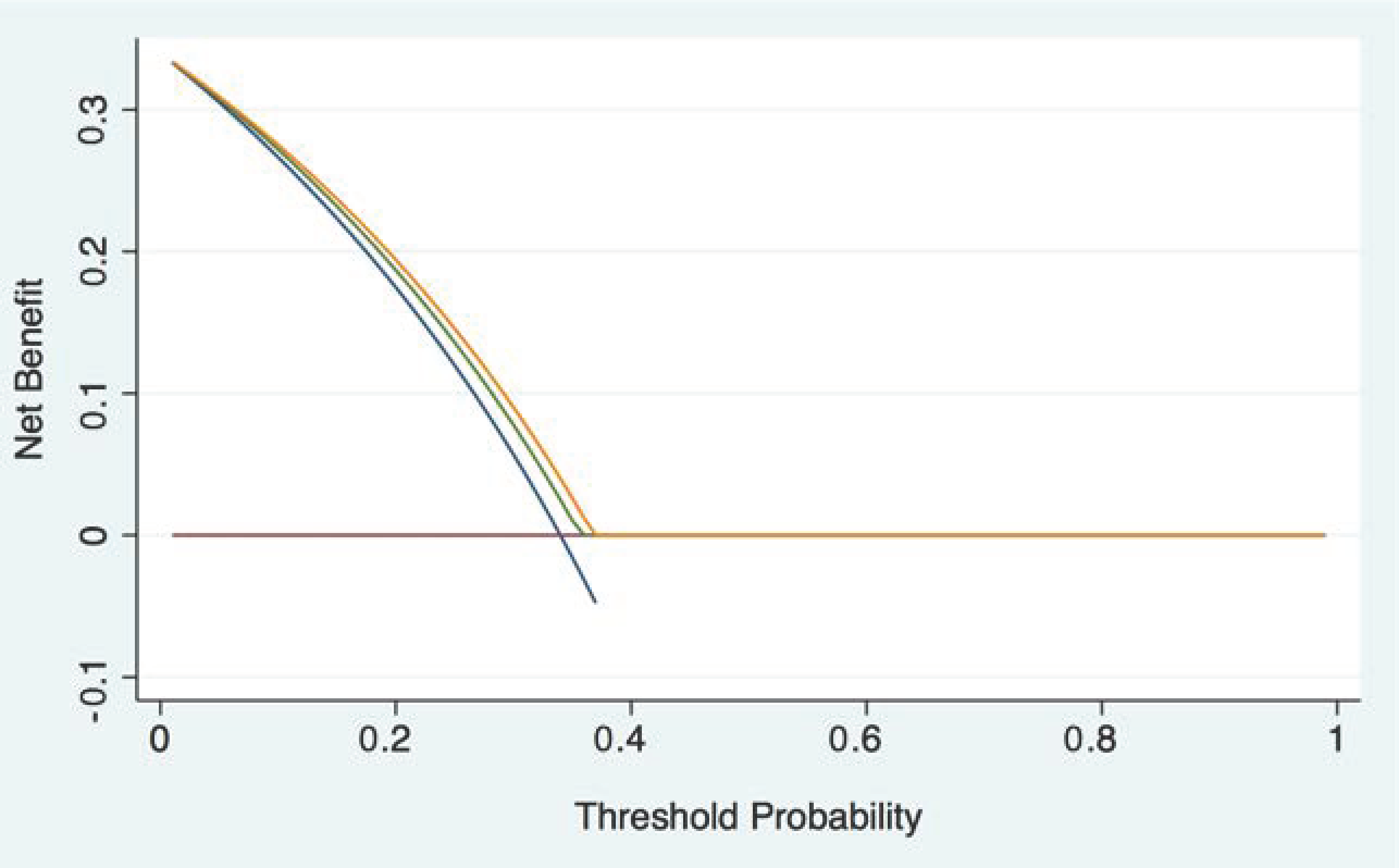
3.4. Integrated Pathway
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vilacosta, I.; San Roman, J.A.; di Bartolomeo, R.; Eagle, K.; Estrera, A.L.; Ferrera, C.; Kaji, S.; Nienaber, C.A.; Riambau, V.; Schafers, H.J.; et al. Acute Aortic Syndrome Revisited: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 2106–2125. [Google Scholar] [CrossRef] [PubMed]
- Morello, F.; Santoro, M.; Fargion, A.T.; Grifoni, S.; Nazerian, P. Diagnosis and management of acute aortic syndromes in the emergency department. Intern. Emerg. Med. 2021, 16, 171–181. [Google Scholar] [CrossRef]
- Hansen, M.S.; Nogareda, G.J.; Hutchison, S.J. Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. Am. J. Cardiol. 2007, 99, 852–856. [Google Scholar] [CrossRef]
- Waxman, D.A.; Kanzaria, H.K.; Schriger, D.L. Unrecognized cardiovascular emergencies among medicare patients. JAMA Intern. Med. 2018, 178, 477–484. [Google Scholar] [CrossRef]
- Holmes, H.R.; Neal, D.; Freeman, K.; Jeng, E.; Back, M.; Huber, T.; Arnaoutakis, K.D.; Shah, S.; Upchurch, G.R., Jr.; Cooper, M.; et al. Misdiagnosis of Thoracic Aortic Disease Occurs Commonly in Emergency Transfers. Ann. Thorac. Surg. 2022, 114, 2202–2208. [Google Scholar] [CrossRef] [PubMed]
- Fattori, R.; Montgomery, D.; Lovato, L.; Kische, S.; Di Eusanio, M.; Ince, H.; Eagle, K.A.; Isselbacher, E.M.; Nienaber, C.A. Survival After Endovascular Therapy in Patients With Type B Aortic Dissection: A Report From the International Registry of Acute Aortic Dissection (IRAD). JACC Cardiovasc. Interv. 2013, 6, 876–882. [Google Scholar] [CrossRef] [Green Version]
- Corsini, A.; Pacini, D.; Lovato, L.; Russo, V.; Lorenzini, M.; Foa, A.; Leone, O.; Nanni, S.; Mingardi, F.; Reggiani, L.B.; et al. Long-term Follow up of Patients with Acute Aortic Syndromes: Relevance of both Aortic and Non-aortic Events. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 200–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, J.M.; Kim, H.; Kwon, O.; Om, S.Y.; Heo, R.; Lee, S.; Kim, D.H.; Kim, H.J.; Kim, J.B.; Jung, S.H.; et al. Differential clinical features and long-term prognosis of acute aortic syndrome according to disease entity. Eur. Heart J. 2019, 40, 2727–2736. [Google Scholar] [CrossRef]
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [Green Version]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, J., 3rd; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146, e334–e482. [Google Scholar] [CrossRef]
- Rogers, A.M.; Hermann, L.K.; Booher, A.M.; Nienaber, C.A.; Williams, D.M.; Kazerooni, E.A.; Froehlich, J.B.; O'Gara, P.T.; Montgomery, D.G.; Cooper, J.V.; et al. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: Results from the international registry of acute aortic dissection. Circulation 2011, 123, 2213–2218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazerian, P.; Giachino, F.; Vanni, S.; Veglio, M.G.; Castelli, M.; Lison, D.; Bitossi, L.; Moiraghi, C.; Grifoni, S.; Morello, F. Diagnostic performance of the aortic dissection detection risk score in patients with suspected acute aortic dissection. Eur. Heart J. Acute Cardiovasc. Care 2014, 3, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Morello, F.; Bima, P.; Pivetta, E.; Santoro, M.; Catini, E.; Casanova, B.; Leidel, B.A.; de Matos Soeiro, A.; Nestelberger, T.; Mueller, C.; et al. Development and Validation of a Simplified Probability Assessment Score Integrated With Age-Adjusted d-Dimer for Diagnosis of Acute Aortic Syndromes. J. Am. Heart Assoc. 2021, 10, e018425. [Google Scholar] [CrossRef]
- Tsutsumi, Y.; Tsujimoto, Y.; Takahashi, S.; Tsuchiya, A.; Fukuma, S.; Yamamoto, Y.; Fukuhara, S. Accuracy of aortic dissection detection risk score alone or with D-dimer: A systematic review and meta-analysis. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, S32–S39. [Google Scholar] [CrossRef] [PubMed]
- Bima, P.; Pivetta, E.; Nazerian, P.; Toyofuku, M.; Gorla, R.; Bossone, E.; Erbel, R.; Lupia, E.; Morello, F. Systematic Review of Aortic Dissection Detection Risk Score Plus D-dimer for Diagnostic Rule-out Of Suspected Acute Aortic Syndromes. Acad Emerg. Med. 2020, 27, 1013–1027. [Google Scholar] [CrossRef]
- Olsson, C.; Thelin, S.; Stahle, E.; Ekbom, A.; Granath, F. Thoracic aortic aneurysm and dissection: Increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation 2006, 114, 2611–2618. [Google Scholar] [CrossRef] [Green Version]
- Booher, A.M.; Isselbacher, E.M.; Nienaber, C.A.; Trimarchi, S.; Evangelista, A.; Montgomery, D.G.; Froehlich, J.B.; Ehrlich, M.P.; Oh, J.K.; Januzzi, J.L.; et al. The IRAD Classification System for Characterizing Survival after Aortic Dissection. Am. J. Med. 2013, 126, 730.e19–730.e24. [Google Scholar] [CrossRef]
- Conway, B.D.; Stamou, S.C.; Kouchoukos, N.T.; Lobdell, K.W.; Khabbaz, K.R.; Murphy, E.; Hagberg, R.C. Improved clinical outcomes and survival following repair of acute type A aortic dissection in the current era. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 971–976. [Google Scholar] [CrossRef]
- Eggebrecht, H.; Naber, C.K.; Bruch, C.; Kroger, K.; von Birgelen, C.; Schmermund, A.; Wichert, M.; Bartel, T.; Mann, K.; Erbel, R. Value of plasma fibrin D-dimers for detection of acute aortic dissection. J. Am. Coll. Cardiol. 2004, 44, 804–809. [Google Scholar] [CrossRef] [Green Version]
- Iyano, K.; Kawada, T.; Aiba, M.; Takaba, T. Correlation of hemostatic molecular markers and morphology of the residual false lumen in chronic aortic dissection. Ann. Thorac. Cardiovasc. Surg. 2004, 10, 106–112. [Google Scholar]
- Fan, Q.K.; Wang, W.W.; Zhang, Z.L.; Liu, Z.J.; Yang, J.; Zhao, G.S.; Cao, S.Z. Evaluation of D-dimer in the diagnosis of suspected aortic dissection. Clin. Chem. Lab. Med. 2010, 48, 1733–1737. [Google Scholar] [CrossRef] [PubMed]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E., Jr.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Nazerian, P.; Morello, F.; Vanni, S.; Bono, A.; Castelli, M.; Forno, D.; Gigli, C.; Soardo, F.; Carbone, F.; Lupia, E.; et al. Combined use of aortic dissection detection risk score and D-dimer in the diagnostic workup of suspected acute aortic dissection. Int. J. Cardiol. 2014, 175, 78–82. [Google Scholar] [CrossRef]
- Nazerian, P.; Mueller, C.; Soeiro, A.M.; Leidel, B.A.; Salvadeo, S.A.T.; Giachino, F.; Vanni, S.; Grimm, K.; Oliveira, M.T., Jr.; Pivetta, E.; et al. Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes: The ADvISED Prospective Multicenter Study. Circulation 2018, 137, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Asha, S.E.; Miers, J.W. A Systematic Review and Meta-analysis of D-dimer as a Rule-out Test for Suspected Acute Aortic Dissection. Ann. Emerg. Med. 2015, 66, 368–378. [Google Scholar] [CrossRef]
- Morello, F.; Piler, P.; Novak, M.; Kruzliak, P. Biomarkers for diagnosis and prognostic stratification of aortic dissection: Challenges and perspectives. Biomark. Med. 2014, 8, 931–941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 128) | nAAS (n = 40) | AltD (n = 88) | p-Value | |
|---|---|---|---|---|
| Age (years), median (IQR) | 66 (57–75) | 63 (55–75) | 68 (57–74) | 0.58 |
| Gender (female), n (%) | 33 (25.8) | 11 (27.5) | 22 (25) | 0.77 |
| Anterior chest pain, n (%) | 66 (51.6) | 22 (55) | 44 (50) | 0.60 |
| Posterior chest pain or lumbar pain, n (%) | 48 (37.5) | 18 (45) | 30 (34.1) | 0.24 |
| Abdominal pain, n (%) | 31 (24.2) | 10 (25) | 21 (23.9) | 0.89 |
| Syncope, n (%) | 11 (8.6) | 6 (15) | 5 (5.7) | 0.082 |
| Perfusion deficit, n (%) | 17 (13.3) | 7 (17.5) | 10 (11.4) | 0.34 |
| Time from symptom onset (hours), median (IQR) [n = 99] | 10 (2–48) | 3 (1–13) | 12 (2–72) | 0.085 |
| Systolic blood pressure (mmHg), median (IQR) | 135 (120–150) | 135 (120–150) | 138 (125–150) | 0.19 |
| Diastolic blood pressure (mmHg), median (IQR) | 80 (70–80) | 70 (60–80) | 80 (70–83.5) | 0.005 |
| Heart rate (bpm), median (IQR) | 74 (65–85) | 80 (67–90) | 74 (64–80) | 0.12 |
| Hypertension, n (%) | 99 (77.3) | 30 (75) | 69 (78.4) | 0.67 |
| Diabetes, n (%) | 10 (7.8) | 2 (5) | 8 (9.1) | 0.43 |
| Smoke, n (%) | 18 (14.1) | 6 (15) | 12 (13.6) | 0.84 |
| Drugs, n (%) [n = 111] | 2 (1.6) | 0 (0) | 2 (2.3) | 0.37 |
| CAD, n (%) [n = 111] | 14 (10.9) | 3 (9.7) | 11 (12.5) | 0.56 |
| Previous surgery for AAS, n (%) [n = 93] | 67 (72) | 19 (79.2) | 48 (69.6) | 0.37 |
| Previous TEVAR for AAS, n (%) [n = 50] | 22 (44) | 9 (47.4) | 13 (41.9) | 0.71 |
| White blood cell count, ×103/µL [n = 94] | 7.71 (6.64–9.71) | 8.8 (7.62–10.38) | 7.33 (6.38–9.44) | 0.027 |
| Creatinine, mg/dL [n = 106] | 0.99 (0.86–1.25) | 1.01 (0.86–1.21) | 0.99 (0.86–1.27) | 0.98 |
| C-reactive protein, mg/L [n = 60] | 12.5 (1.8–40.7) | 25.1 (11.7–59.2) | 7.1 (0.9–32.2) | 0.033 |
| All Patients (n = 128) | nAAS (n = 40) | AltD (n = 88) | Odds Ratio | p-Value | |
|---|---|---|---|---|---|
| Marfan/other connective tissue disease, n (%) | 11 (8.6) | 3 (7.5) | 8 (9.1) | 0.81 (0.2–3.23) | 0.77 |
| Family history of acute aortic syndrome, n (%) | 3 (2.3) | 1 (2.5) | 2 (2.3) | 1.1 (0.1–12.53) | 0.94 |
| Known aortic valve disease, n (%) | 25 (19.5) | 12 (30) | 13 (14.8) | 2.47 (1.01–6.06) | 0.045 |
| Recent aortic manipulation, n (%) | 24 (18.9) | 9 (22.5) | 15 (17) | 1.41 (0.56–3.57) | 0.47 |
| Known thoracic aortic aneurism, n (%) | 16 (12.5) | 9 (22.5) | 7 (8) | 3.36 (1.15–9.8) | 0.022 |
| Severe pain, n (%) | 32 (25) | 16 (40) | 16 (18.2) | 3 (1.3–6.9) | 0.009 |
| Sudden pain, n (%) | 28 (21.9) | 17 (42.5) | 11 (12.5) | 5.17 (2.12–12.6) | <0.001 |
| Ripping pain, n (%) | 3 (2.4) | 3 (7.5) | 0 (0) | 16.52 (0.83–327.77) | 0.010 |
| Pulse asymmetry or systolic blood pressure differential > 20 mmHg, n (%) | 19 (14.8) | 6 (15) | 13 (14.8) | 1.02 (0.36–2.91) | 0.97 |
| Focal neurological deficit, n (%) | 12 (9.4) | 5 (12.5) | 7 (8) | 1.65 (0.49–5.57) | 0.42 |
| New or unknown diastolic aortic murmur, n (%) | 3 (2.3) | 2 (5) | 1 (1.1) | 4.58 (0.4–52.04) | 0.18 |
| Hypotension or shock state, n (%) | 9 (7) | 7 (17.5) | 2 (2.3) | 9.12 (1.8–46.18) | 0.002 |
| ADD score = 0 | 34 (26.6) | 6 (15) | 28 (31.8) | ||
| ADD score = 1, n (%) | 53 (41.4) | 8 (20) | 45 (51.1) | ||
| ADD score ≥ 2, n (%) | 41 (32) | 26 (65) | 15 (17) | ||
| AORTAs score = 0 | 57 (44.5) | 10 (25) | 47 (53.4) | ||
| AORTAs score = 1, n (%) | 41 (32) | 11 (27.5) | 30 (34.1) | ||
| AORTAs score ≥ 2, n (%) | 30 (33.4) | 19 (47.5) | 11 (12.5) |
| TP | FP | TN | FN | Sensitivity (%) | Specificity (%) | LR+ | LR− | |
|---|---|---|---|---|---|---|---|---|
| ADD ≥ 1 | 34 | 60 | 28 | 6 | 85 (70.2–94.3) | 31.8 (22.3–42.6) | 1.25 (1.03–1.51) | 0.47 (0.21–1.05) |
| ADD ≥ 2 | 26 | 15 | 73 | 14 | 65 (48.3–79.4) | 83 (73.4–90.1) | 3.81 (2.28–6.38) | 0.42 (0.27–0.65) |
| AORTAs ≥ 1 | 30 | 41 | 47 | 10 | 75 (58.8–87.3) | 53.4 (42.5–64.1) | 1.61 (1.21–2.14) | 0.47 (0.26–0.83) |
| AORTAs ≥ 2 | 19 | 11 | 77 | 21 | 47.5 (31.5–63.9) | 87.5 (78.7–93.6) | 3.8 (2–7.22) | 0.6 (0.44–0.81) |
| TP | FP | TN | FN | Sensitivity (%) | Specificity (%) | LR+ | LR− | |
|---|---|---|---|---|---|---|---|---|
| ≥500 ng/mL | 35 | 60 | 8 | 0 | 100 (90–100) | 11.8 (5.2–21.9) | 1.13 (1.04–1.24) | 0 |
| ≥750 ng/mL | 35 | 57 | 11 | 0 | 100 (90–100) | 16.2 (8.4–27.1) | 1.19 (1.07–1.32) | 0 |
| ≥1000 ng/mL | 29 | 57 | 11 | 6 | 82.9 (66.4–93.4) | 23.5 (14.1–35.4) | 1.08 (0.89–1.32) | 0.73 (0.31–1.7) |
| ≥age-adjusted cutoff * | 35 | 59 | 9 | 0 | 100 (90–100) | 13.2 (6.2–23.6) | 1.15 (1.05–1.26) | 0 |
| N | FN | Sensitivity (%) | Specificity (%) | LR− | Efficiency * | |
|---|---|---|---|---|---|---|
| ADD = 0 or DD < 500 ng/mL | 2 | 0 | 100 (90–100) | 2.9 (0.4–10.2) | 0 | 1 in 52 |
| ADD = 0 or DD < 1000 ng/mL | 5 | 0 | 100 (90–100) | 7.4 (2.4–16.3) | 0 | 1 in 21 |
| ADD ≤1 or DD < 500 ng/mL | 5 | 0 | 100 (90–100) | 7.4 (2.4–16.3) | 0 | 1 in 21 |
| ADD ≤1 or DD < 1000 ng/mL | 13 | 2 | 94.3 (80.8–99.3) | 16.2 (8.4–27.1) | 0.35 (0.08–1.51) | 1 in 8 |
| AORTAs = 0 or DD < age-adj. cutoff * | 4 | 0 | 100 (90–100) | 5.9 (1.6–14.4) | 0 | 1 in 26 |
| AORTAs = 0 or DD < 1000 ng/mL | 8 | 1 | 97.1 (85.1–99.9) | 10.3 (4.2–20.1) | 0.28 (0.04–2.17) | 1 in 13 |
| AORTAs ≤ 1 or DD < age-adj. cutoff * | 8 | 0 | 100 (90–100) | 11.8 (5.2–21.9) | 0 | 1 in 13 |
| AORTAs ≤ 1 or DD < 1000 ng/mL | 17 | 5 | 85.7 (69.7–95.2) | 17.7 (9.5–28.8) | 0.81 (0.31–2.11) | 1 in 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morello, F.; Santoro, M.; Giachino, F.; Caciolli, F.; Capretti, E.; Castelli, M.; Pivetta, E.; Nazerian, P.; Lupia, E. Pre-Test Probability Assessment and d-Dimer Based Evaluation in Patients with Previous Acute Aortic Syndrome. Medicina 2023, 59, 548. https://doi.org/10.3390/medicina59030548
Morello F, Santoro M, Giachino F, Caciolli F, Capretti E, Castelli M, Pivetta E, Nazerian P, Lupia E. Pre-Test Probability Assessment and d-Dimer Based Evaluation in Patients with Previous Acute Aortic Syndrome. Medicina. 2023; 59(3):548. https://doi.org/10.3390/medicina59030548
Chicago/Turabian StyleMorello, Fulvio, Marco Santoro, Francesca Giachino, Francesca Caciolli, Elisa Capretti, Matteo Castelli, Emanuele Pivetta, Peiman Nazerian, and Enrico Lupia. 2023. "Pre-Test Probability Assessment and d-Dimer Based Evaluation in Patients with Previous Acute Aortic Syndrome" Medicina 59, no. 3: 548. https://doi.org/10.3390/medicina59030548