
Effective Dose Range of Intrathecal Isobaric Bupivacaine to Achieve T5–T10 Sensory Block Heights for Elderly and Overweight Patients: An Observational Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Spinal Block Technique
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gropper, M.A. Miller’s Anesthesia, 9th ed.; Elsevier: Philadelphia, PA, USA, 2019; pp. 1423–1425. [Google Scholar]
- Barash, P.G. Clinical Anesthesia, 8th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2017; p. 916. [Google Scholar]
- Hocking, G.; Wildsmith, J.A. Intrathecal drug spread. Br. J. Anaesth. 2004, 93, 568–578. [Google Scholar] [CrossRef] [Green Version]
- Shen, L.; Liu, P.; Feng, F.; Chen, L.; Wang, S.; Wang, R.; Liu, W.; Zhao, B.; Guan, L. A prospective study on the association between spinal anesthesia and obesity. Trop. J. Pharm. Res. 2018, 17, 695–700. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Chen, C.; Ke, Q. The effect of age on the median effective dose (ED50) of intrathecally administered plain bupivacaine for motor block. Anesth. Analg. 2014, 118, 863–868. [Google Scholar] [CrossRef]
- Ingrande, J.; Brodsky, J.B.; Lemmens, H.J. Regional anesthesia and obesity. Curr. Opin. Anaesthesiol. 2009, 22, 683–686. [Google Scholar] [CrossRef]
- Gragasin, F.S.; Tsui, B.C.H. Local and regional anesthesia in the elderly. In Complications of Regional Anesthesia: Principles of Safe Practice in Local and Regional Anesthesia; Finucane, B.T., Tsui, B.C.H., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 287–301. [Google Scholar]
- Sullivan, J.T.; Grouper, S.; Walker, M.T.; Parrish, T.B.; McCarthy, R.J.; Wong, C.A. Lumbosacral cerebrospinal fluid volume in humans using three-dimensional magnetic resonance imaging. Anesth. Analg. 2006, 103, 1306–1310. [Google Scholar] [CrossRef] [PubMed]
- Hogan, Q.H.; Prost, R.; Kulier, A.; Taylor, M.L.; Liu, S.; Mark, L. Magnetic resonance imaging of cerebrospinal fluid volume and the influence of body habitus and abdominal pressure. Anesthesiology 1996, 84, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, W.H.; Lim, H.W.; Kim, J.A.; Kim, D.K.; Shin, B.S.; Hahm, T.S.; Kim, C.S.; Lee, S.M. Obesity is independently associated with spinal anesthesia outcomes: A prospective observational study. PLoS ONE 2015, 10, e0124264. [Google Scholar] [CrossRef] [Green Version]
- Leino, K.A.; Kuusniemi, K.S.; Palve, H.K.; Tiusanen, H.T.; Tuppurainen, T.T. The effect of body mass index on the spread of spinal block in patients with rheumatoid arthritis. J. Anesth. 2011, 25, 213–218. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, W.J.; Littlewood, D.G. Influence of obesity on spinal analgesia with isobaric 0.5% bupivacaine. Br. J. Anaesth. 1986, 58, 610–614. [Google Scholar] [CrossRef]
- Fettes, P.D.; Jansson, J.R.; Wildsmith, J.A. Failed spinal anaesthesia: Mechanisms, management, and prevention. Br. J. Anaesth. 2009, 102, 739–748. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.Y.; Chang, K.Y. Sensory block level prediction of spinal anaesthesia with 0.5% hyperbaric bupivacaine: A retrospective study. Sci. Rep. 2021, 11, 9105. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, B.; Junger, A.; Klasen, J.; Benson, M.; Jost, A.; Banzhaf, A.; Hempelmann, G. The incidence and risk factors for hypotension after spinal anesthesia induction: An analysis with automated data collection. Anesth. Analg. 2002, 94, 1521–1529. [Google Scholar] [CrossRef]
- Abouleish, E.; Giezentanner, A. Heart rate changes with high spinal anesthesia. Anesth. Analg. 1992, 74, 774–775. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, K.; Hagiwara, R.; Nakamura, K.; Ishizeki, J.; Kubo, K.; Saito, S.; Goto, F. The effects of the extent of spinal block on the BIS score and regional cerebral oxygen saturation in elderly patients: A prospective, randomized, and double-blinded study. J. Clin. Monit. Comput. 2007, 21, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Günkaya, M.; Arar, C.; Mordeniz, C.; Baran, O.; Topçu, B. Effect of waist circumference and body mass index on the level of spinal anesthesia. Ain-Shams J. Anesthesiol. 2022, 14, 19. [Google Scholar] [CrossRef]
- Kalichman, L.; Cole, R.; Kim, D.H.; Li, L.; Suri, P.; Guermazi, A.; Hunter, D.J. Spinal stenosis prevalence and association with symptoms: The Framingham study. Spine J. 2009, 9, 545–550. [Google Scholar] [CrossRef] [Green Version]
- Van Calster, B.; Vergouwe, Y.; Looman, C.W.; Van Belle, V.; Timmerman, D.; Steyerberg, E.W. Assessing the discriminative ability of risk models for more than two outcome categories. Eur. J. Epidemiol. 2012, 27, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Van Egmond, J.C.; Verburg, H.; Derks, E.A.; Langendijk, P.N.J.; Icli, C.; Van Dasselaar, N.T.; Mathijssen, N.M.C. Optimal dose of intrathecal isobaric bupivacaine in total knee arthroplasty. Can. J. Anaesth. 2018, 65, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Michalek-Sauberer, A.; Kozek-Langenecker, S.A.; Heinzl, H.; Deusch, E.; Chiari, A. Median effective local anesthetic doses of plain bupivacaine and ropivacaine for spinal anesthesia administered via a spinal catheter for brachytherapy of the lower abdomen. Reg. Anesth. Pain Med. 2008, 33, 4–9. [Google Scholar] [CrossRef]
- Yu, S.; Saleh, H.; Bolz, N.; Buza, J.; Iorio, R.; Rathod, P.A.; Schwarzkopf, R.; Deshmukh, A. Re-revision total hip arthroplasty: Epidemiology and factors associated with outcomes. J. Clin. Orthop. Trauma. 2020, 11, 43–46. [Google Scholar] [CrossRef]
- Logan, M.R.; McClure, J.H.; Wildsmith, J.A. Plain bupivacaine: An unpredictable spinal anaesthetic agent. Br. J. Anaesth. 1986, 58, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Taivainen, T.; Tuominen, M.; Rosenberg, P.H. Influence of obesity on the spread of spinal analgesia after injection of plain 0.5% bupivacaine at the L3-4 or L4-5 interspace. Br. J. Anaesth. 1990, 64, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Parate, L.H.; Manjunath, B.; Tejesh, C.A.; Pujari, V. Inaccurate level of intervertebral space estimated by palpation: The ultrasonic revelation. Saudi J. Anaesth. 2016, 10, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.H.; Lee, J.H.; Ko, J.S.; Ahn, H.J.; Park, S.K.; Gwak, M.S.; Kim, G.S. The effect of body mass index on spinal anaesthesia for total knee replacement arthroplasty: A dose-response study. Anaesth. Intensive Care. 2012, 40, 410–416. [Google Scholar] [CrossRef] [Green Version]
- Veering, B.T.; Burm, A.G.; van Kleef, J.W.; Hennis, P.J.; Spierdijk, J. Spinal anesthesia with glucose-free bupivacaine: Effects of age on neural blockade and pharmacokinetics. Anesth. Analg. 1987, 66, 965–970. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characters | Low Sensory Block Level (≤T11) | Favorable Sensory Block Level (T5–T10) | High Sensory Block Level (≥T4) | p Value | |||
|---|---|---|---|---|---|---|---|
| (n = 146) | (n = 762) | (n = 171) | |||||
| Male | 89 | (61.0) | 366 | (48.0) | 62 | (36.3) | <0.001 |
| Age (year) | 45.8 | ±19.9 | 55.1 | ±20.7 | 58.5 | ±18.5 | <0.001 |
| Weight (kg) | 61.2 | ±10.4 | 60.1 | ±12.4 | 63.0 | ±12.5 | 0.016 |
| Height (cm) | 163.6 | ±8.2 | 160.1 | ±9.3 | 158.7 | ±9.1 | <0.001 |
| BMI (kg/m2) | 22.9 | ±3.4 | 23.4 | ±4.1 | 25.0 | ±4.5 | <0.001 |
| Location of operation | |||||||
| Upper abdomen | 0 | (0) | 1 | (0.1) | 0 | (0) | 0.025 |
| Lower abdomen | 0 | (0) | 4 | (0.5) | 2 | (1.2) | |
| Groin/inguinal | 1 | (0.7) | 24 | (3.2) | 1 | (0.6) | |
| Hip | 11 | (7.5) | 85 | (11.2) | 10 | (5.9) | |
| Lower extremity | 127 | (87.0) | 586 | (76.9) | 152 | (88.9) | |
| Perineum/anus | 1 | (0.7) | 24 | (3.2) | 2 | (1.2) | |
| Others | 6 | (4.1) | 38 | (5.0) | 4 | (2.3) | |
| Injection level | |||||||
| L2–L3 | 8 | (5.5) | 31 | (4.1) | 7 | (4.1) | 0.253 |
| L3–L4 | 98 | (67.1) | 531 | (69.7) | 118 | (69.0) | |
| L4–L5 | 36 | (24.7) | 194 | (25.5) | 46 | (26.9) | |
| L5–S1 | 4 | (2.7) | 6 | (0.8) | 0 | (0) | |
| Bupivacaine dose (mg) | 16.1 | ±2.5 | 16.4 | ±2.3 | 17.2 | ±2.3 | <0.001 |
| Peak level of sensory nerve block | |||||||
| T1–T2 | - | - | - | - | 9 | (5.3) | <0.001 |
| T3–T4 | - | - | - | - | 162 | (94.7) | |
| T5–T6 | - | - | 215 | (28.2) | - | - | |
| T7–T8 | - | - | 183 | (24.0) | - | - | |
| T9–T10 | - | - | 364 | (47.8) | - | - | |
| T11–T12 | 113 | (77.4) | - | - | - | - | |
| L1–L2 | 33 | (22.6) | - | - | - | - | |
| Characters | Low Sensory Block Level (≤T11) | Favorable Sensory Block Level (T5–T10) | High Sensory Block Level (≥T4) | p Value | |||
|---|---|---|---|---|---|---|---|
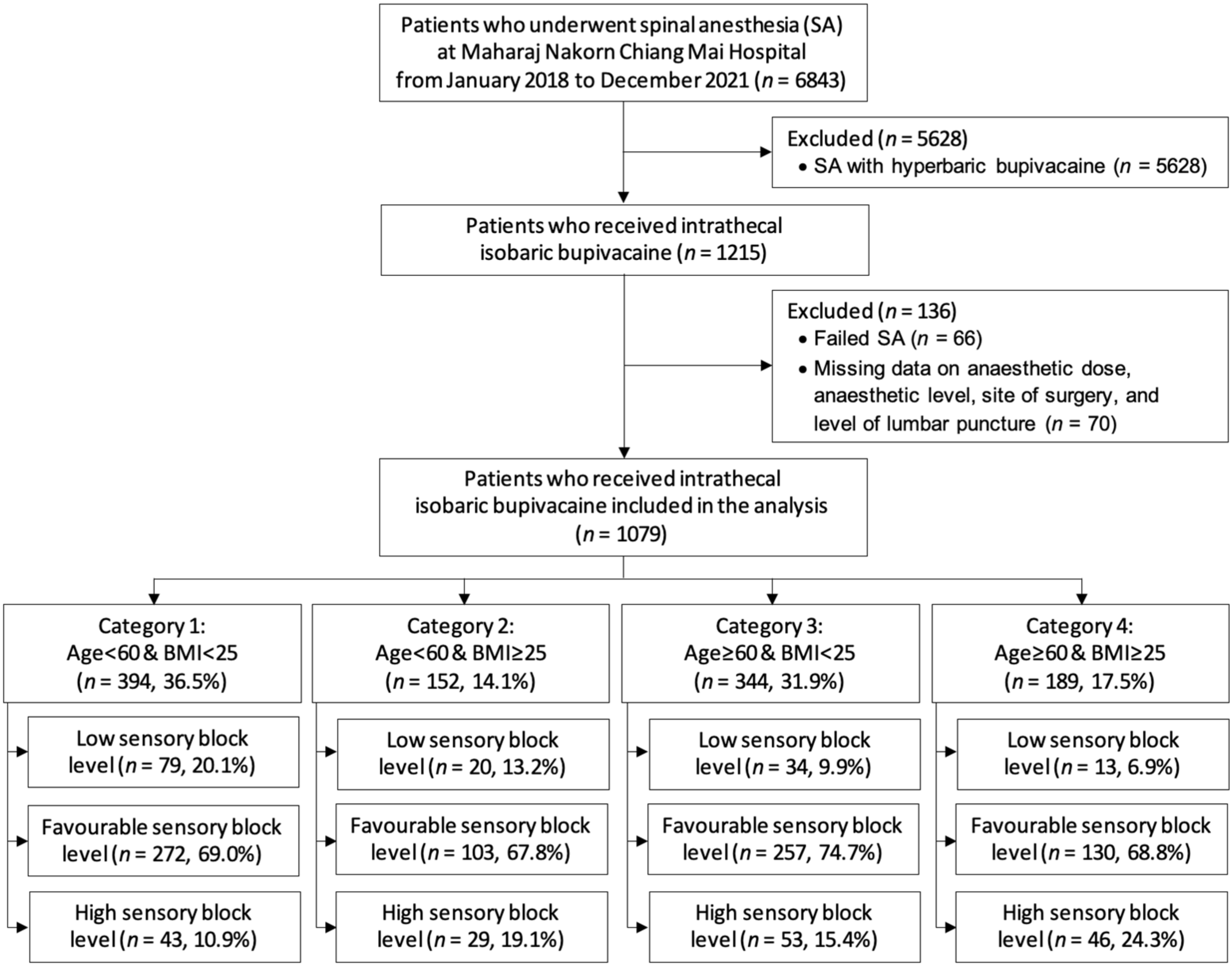
| Category 1 (n = 394) | 79 | (20.1) | 272 | (69.0) | 43 | (10.9) | |
| Male | 54 | (68.4) | 168 | (61.8) | 24 | (55.8) | 0.357 |
| Age (year) | 34.4 | ±14.1 | 37.0 | ±15.2 | 39.6 | ±14.2 | 0.163 |
| Weight (kg) | 59.1 | ±9.5 | 57.0 | ±8.4 | 57.4 | ±8.6 | 0.163 |
| Height (cm) | 165.2 | ±8.6 | 163.3 | ±8.8 | 162.9 | ±8.1 | 0.194 |
| BMI (kg/m2) | 21.6 | ±2.4 | 21.3 | ±2.2 | 21.6 | ±2.2 | 0.559 |
| Injection level | |||||||
| L2–L3 | 5 | (6.3) | 9 | (3.3) | 1 | (2.3) | 0.406 |
| L3–L4 | 53 | (67.1) | 192 | (70.6) | 29 | (67.4) | |
| L4–L5 | 20 | (25.3) | 71 | (26.1) | 13 | (30.2) | |
| L5–S1 | 1 | (1.3) | 0 | (0) | 0 | (0) | |
| Bupivacaine dose (mg) | 16.4 | ±2.6 | 16.8 | ±2.1 | 18.0 | ±2.1 | <0.001 |
| Category 2 (n = 152) | 20 | (13.2) | 103 | (67.8) | 29 | (19.1) | |
| Male | 13 | (65.0) | 67 | (65.1) | 16 | (55.2) | 0.622 |
| Age (year) | 37.8 | ±13.4 | 40.9 | ±12.6 | 43.7 | ±14.5 | 0.295 |
| Weight (kg) | 72.6 | ±5.7 | 76.5 | ±10.6 | 77.4 | ±12.1 | 0.244 |
| Height (cm) | 161.8 | ±7.9 | 164.6 | ±9.6 | 162.2 | ±11.5 | 0.317 |
| BMI (kg/m2) | 27.8 | ±1.7 | 28.2 | ±2.7 | 29.5 | ±4.7 | 0.082 |
| Injection level | |||||||
| L2–L3 | 1 | (5.0) | 3 | (2.9) | 0 | (0) | 0.236 |
| L3–L4 | 13 | (65.0) | 75 | (72.8) | 22 | (75.9) | |
| L4–L5 | 5 | (25.0) | 25 | (24.3) | 7 | (24.1) | |
| L5–S1 | 1 | (5.0) | 0 | (0) | 0 | (0) | |
| Bupivacaine dose (mg) | 16.0 | ±2.1 | 17.2 | ±2.2 | 18.2 | ±1.8 | 0.003 |
| Category 3 (n = 344) | 34 | (9.9) | 257 | (74.7) | 53 | (15.4) | |
| Male | 18 | (52.9) | 99 | (38.5) | 12 | (22.6) | 0.013 |
| Age (year) | 68.5 | ±8.6 | 73.0 | ±9.6 | 72.1 | ±8.2 | 0.028 |
| Weight (kg) | 56.8 | ±9.7 | 52.5 | ±9.1 | 53.9 | ±8.5 | 0.031 |
| Height (cm) | 162.7 | ±6.8 | 157.2 | ±8.6 | 155.3 | ±8.8 | <0.001 |
| BMI (kg/m2) | 21.4 | ±3.0 | 21.2 | ±2.5 | 22.3 | ±2.2 | 0.014 |
| Injection level | |||||||
| L2–L3 | 2 | (5.9) | 11 | (4.3) | 2 | (3.8) | 0.947 |
| L3–L4 | 22 | (64.7) | 170 | (66.2) | 35 | (66.0) | |
| L4–L5 | 10 | (29.4) | 72 | (28.0) | 16 | (30.2) | |
| L5–S1 | 0 | (0) | 4 | (1.6) | 0 | (0) | |
| Bupivacaine dose (mg) | 15.7 | ±2.7 | 15.7 | ±2.4 | 16.5 | ±2.7 | 0.094 |
| Category 4 (n = 189) | 13 | (6.9) | 130 | (68.8) | 46 | (24.3) | |
| Male | 4 | (30.8) | 32 | (24.6) | 10 | (21.7) | 0.750 |
| Age (year) | 68.1 | ±6.0 | 69.0 | ±7.3 | 69.6 | ±7.8 | 0.786 |
| Weight (kg) | 68.2 | ±6.3 | 68.4 | ±8.7 | 69.5 | ±6.6 | 0.712 |
| Height (cm) | 158.6 | ±6.6 | 155.8 | ±7.5 | 156.5 | ±5.8 | 0.347 |
| BMI (kg/m2) | 27.1 | ±1.4 | 28.2 | ±3.0 | 28.4 | ±2.6 | 0.309 |
| Injection level | |||||||
| L2–L3 | 0 | (0) | 8 | (6.2) | 4 | (8.7) | 0.026 |
| L3–L4 | 10 | (76.9) | 94 | (72.3) | 32 | (69.6) | |
| L4–L5 | 1 | (7.7) | 26 | (20.0) | 10 | (21.7) | |
| L5–S1 | 2 | (15.4) | 2 | (1.5) | 0 | (0) | |
| Bupivacaine dose (mg) | 15.7 | ±2.1 | 16.1 | ±2.1 | 16.6 | ±2.0 | 0.196 |
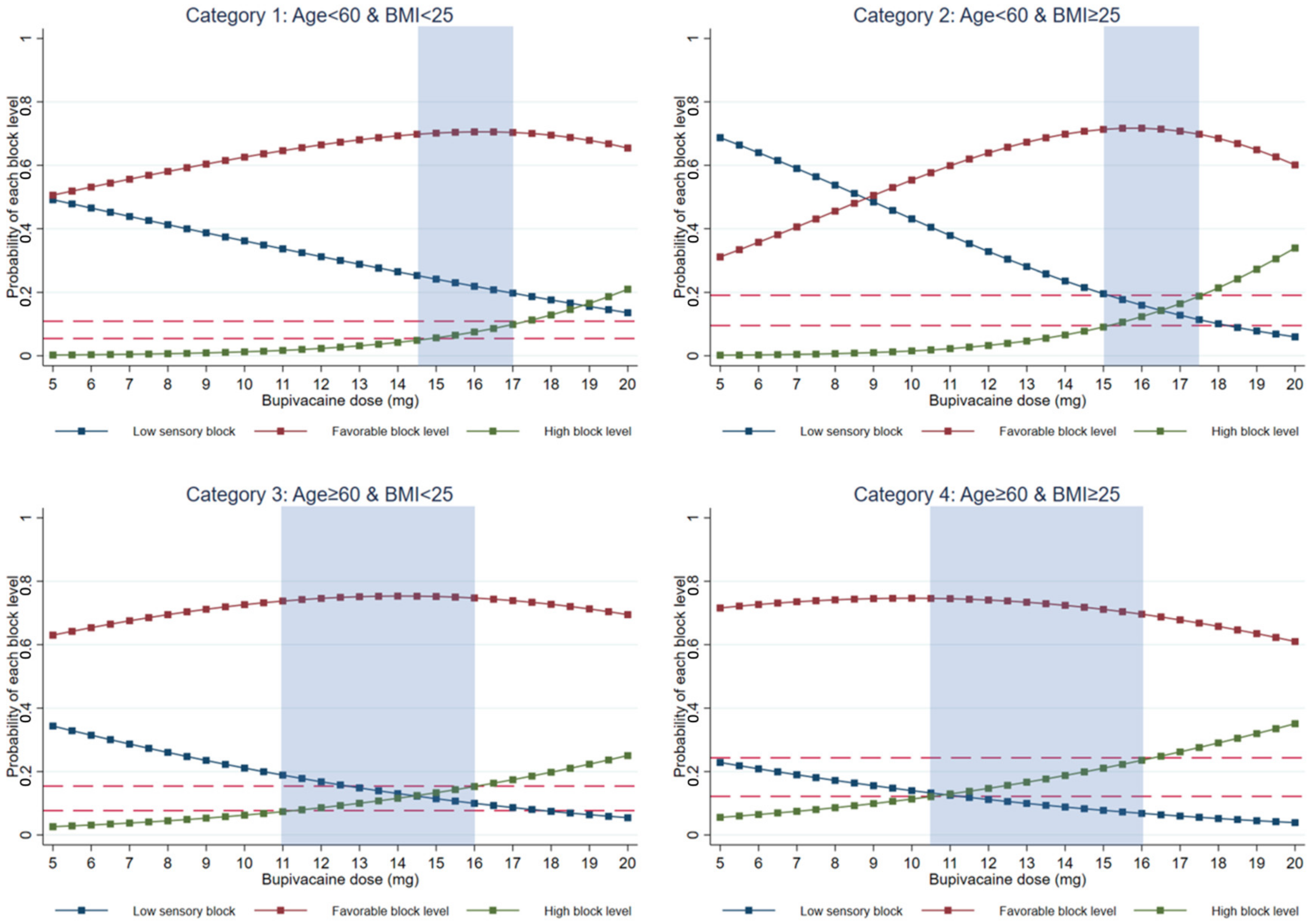
| Category 1: Age < 60 BMI < 25 | Category 2: Age < 60 BMI ≥ 25 | Category 3: Age ≥ 60 BMI < 25 | Category 4: Age ≥ 60 BMI ≥ 25 | |
|---|---|---|---|---|
| Suggested dose range for favorable sensory block level (mg) | 14.5–17.0 | 15.0–17.5 | 11.0–16.0 | 10.5–16.0 |
| Pairwise c-indexes | ||||
| Low vs. Favorable | 0.62 (0.55, 0.69) | 0.73 (0.62, 0.84) | 0.75 (0.66, 0.83) | 0.81 (0.73, 0.90) |
| Low vs. High | 0.74 (0.65, 0.83) | 0.84 (0.74, 0.95) | 0.82 (0.73, 0.90) | 0.86 (0.75, 0.97) |
| Favorable vs. High | 0.67 (0.59, 0.76) | 0.66 (0.53, 0.79) | 0.68 (0.60, 0.77) | 0.62 (0.53, 0.72) |
| Frequency and Percentage of High Sensory Block | Frequency and Percentage of Favorable Sensory Block | |||||
|---|---|---|---|---|---|---|
| Total | Within Suggested Dose Range | Out of Suggested Dose Range | Total | Within Suggested Dose Range | Out of Suggested Dose Range | |
| Overall | 171/1079 (15.9) | 69/571 (12.1) | 102/508 (20.1) | 762/1079 (70.6) | 422/571 (73.9) | 340/508 (66.9) |
| Dose (mg) | 16.5 ± 2.4 | 15.1 ± 1.3 | 18.0 ± 2.3 | 16.5 ± 2.4 | 15.1 ± 1.3 | 18.0 ± 2.3 |
| Category 1 | 43/394 (10.9) | 14/191 (7.3) | 29/203 (14.3) | 272/394 (69.0) | 140/191 (73.3) | 132/203 (65.0) |
| Dose (mg) | 16.9 ± 2.3 | 15.7 ± 0.8 | 18 ± 2.6 | 16.9 ± 2.3 | 15.7 ± 0.8 | 18 ± 2.6 |
| Category 2 | 29/152 (19.1) | 8/75 (10.7) | 21/77 (27.3) | 103/152 (67.8) | 55/75 (73.3) | 48/77 (62.3) |
| Dose (mg) | 17.2 ± 2.2 | 16.0 ± 1.0 | 18.4 ± 2.5 | 17.2 ± 2.2 | 16.0 ± 1.0 | 18.4 ± 2.5 |
| Categories 1 and 2 | 72/546 (13.2) | 22/266 (8.3) | 50/280 (17.9) | 375/546 (68.7) | 195/266 (73.3) | 180/280 (64.3) |
| Dose (mg) | 17.0 ± 2.2 | 15.8 ± 0.9 | 18.1 ± 2.6 | 17.0 ± 2.2 | 15.8 ± 0.9 | 18.1 ± 2.6 |
| Category 3 | 53/344 (15.4) | 24/199 (12.1) | 29/145 (20.0) | 257/344 (74.7) | 153/199 (76.9) | 104/145 (71.7) |
| Dose (mg) | 15.8 ± 2.5 | 14.3 ± 1.3 | 17.9 ± 2.2 | 15.8 ± 2.5 | 14.3 ± 1.3 | 17.9 ± 2.2 |
| Category 4 | 46/189 (24.3) | 23/106 (21.7) | 23/83 (27.7) | 130/189 (68.8) | 74/106 (69.8) | 56/83 (67.5) |
| Dose (mg) | 16.2 ± 2.1 | 14.8 ± 1.0 | 17.9 ± 1.7 | 16.2 ± 2.1 | 14.8 ± 1.0 | 17.9 ± 1.7 |
| Categories 3 and 4 | 99/533 (18.6) | 47/305 (15.4) | 52/228 (22.8) | 387/533 (72.6) | 227/305 (74.4) | 160/228 (70.2) |
| Dose (mg) | 16.0 ± 2.3 | 14.5 ± 1.2 | 17.9 ± 2.1 | 16.0 ± 2.3 | 14.5 ± 1.2 | 17.9 ± 2.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visavakul, O.; Leurcharusmee, P.; Pipanmekaporn, T.; Khorana, J.; Patumanond, J.; Phinyo, P. Effective Dose Range of Intrathecal Isobaric Bupivacaine to Achieve T5–T10 Sensory Block Heights for Elderly and Overweight Patients: An Observational Study. Medicina 2023, 59, 484. https://doi.org/10.3390/medicina59030484
Visavakul O, Leurcharusmee P, Pipanmekaporn T, Khorana J, Patumanond J, Phinyo P. Effective Dose Range of Intrathecal Isobaric Bupivacaine to Achieve T5–T10 Sensory Block Heights for Elderly and Overweight Patients: An Observational Study. Medicina. 2023; 59(3):484. https://doi.org/10.3390/medicina59030484
Chicago/Turabian StyleVisavakul, Ornwara, Prangmalee Leurcharusmee, Tanyong Pipanmekaporn, Jiraporn Khorana, Jayanton Patumanond, and Phichayut Phinyo. 2023. "Effective Dose Range of Intrathecal Isobaric Bupivacaine to Achieve T5–T10 Sensory Block Heights for Elderly and Overweight Patients: An Observational Study" Medicina 59, no. 3: 484. https://doi.org/10.3390/medicina59030484