
Efficacy of Smear Layer Removal at the Apical One-Third of the Root Using Different Protocols of Erbium-Doped Yttrium Aluminium Garnet (Er:YAG) Laser

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Root Canal Preparation and Activation Procedures
2.3. Temperature Measurements
2.4. Sample Fixation and Preparation
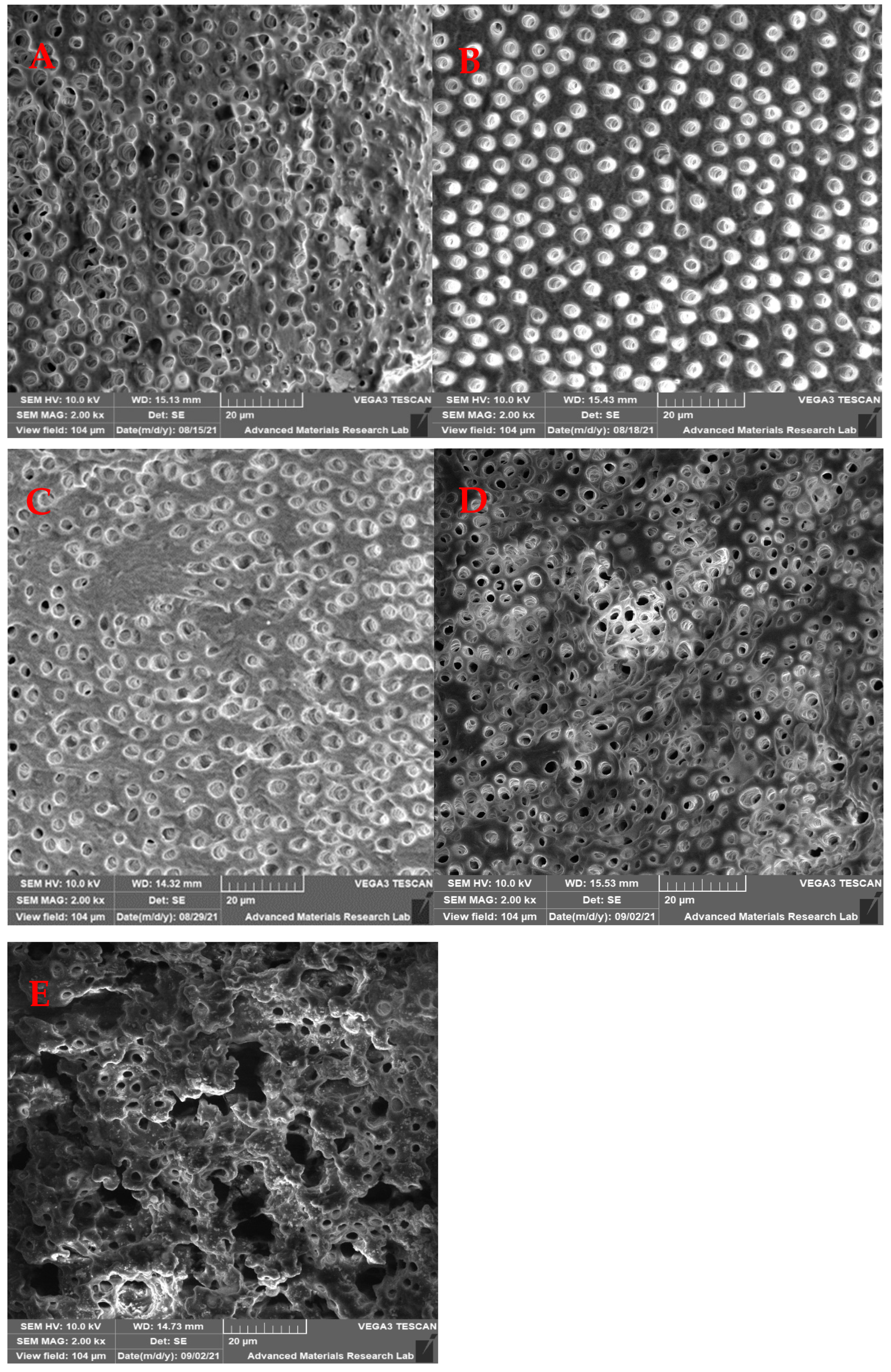
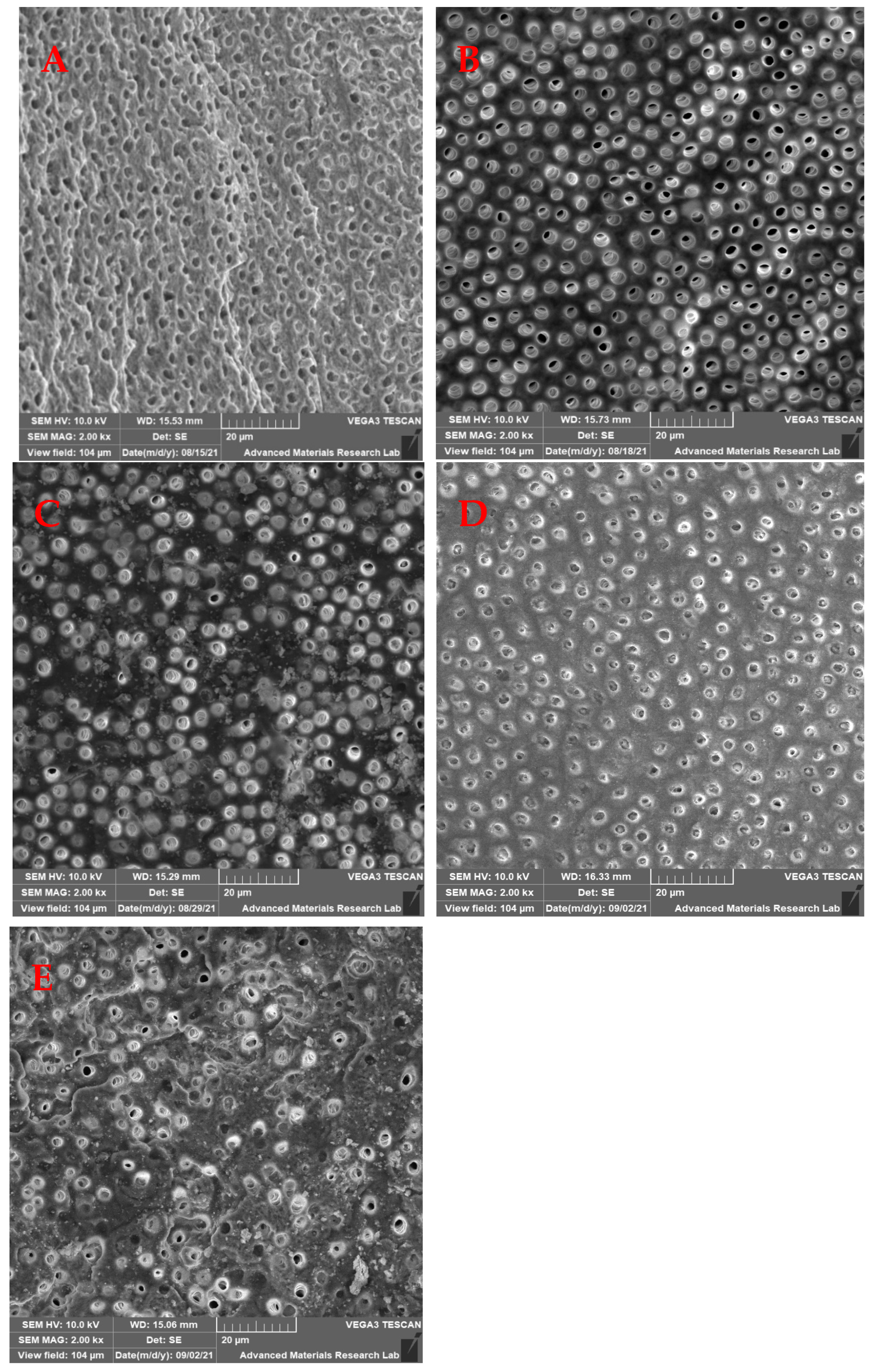
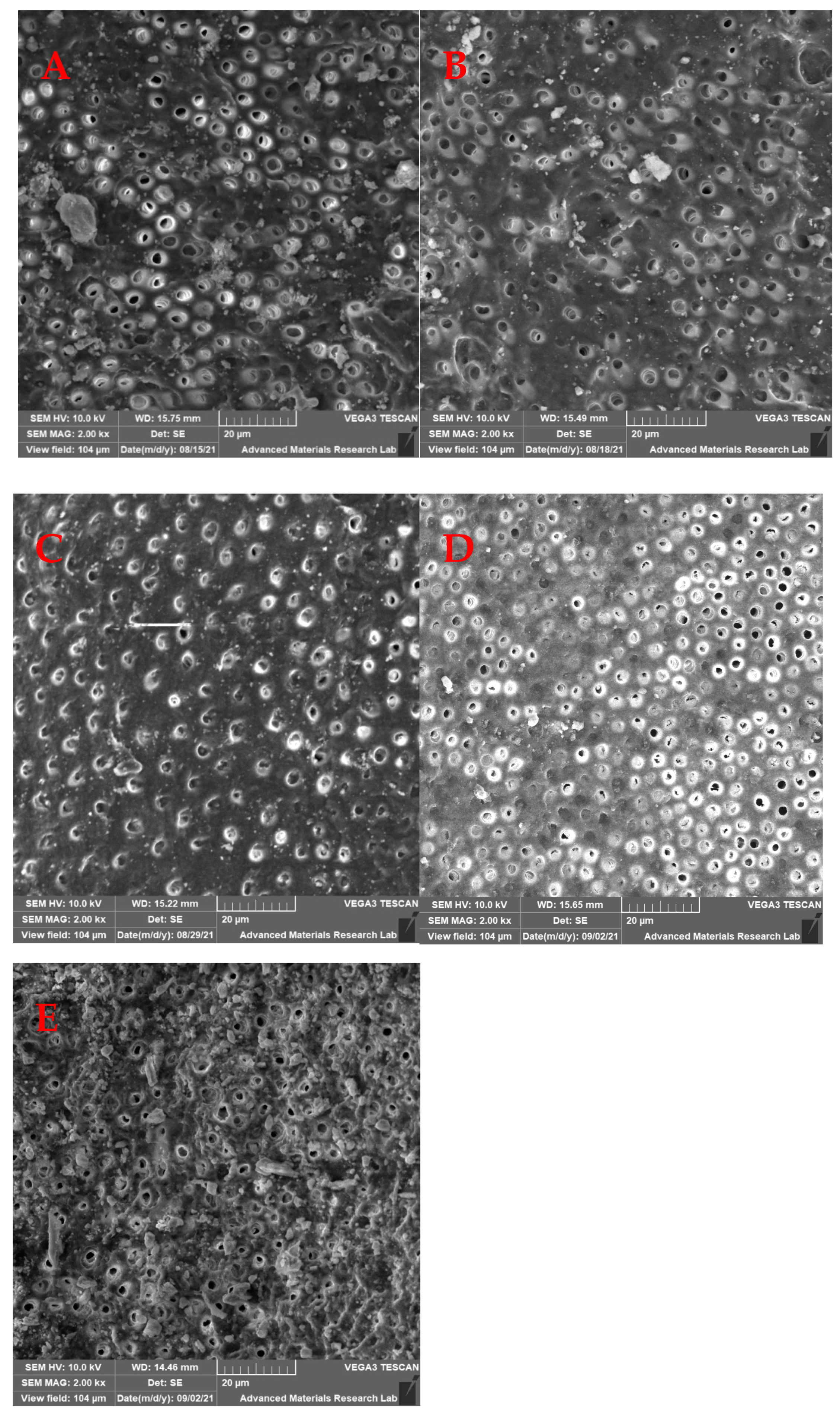
2.5. Scanning Electron Microscopy
2.6. Statistical Analysis
3. Results
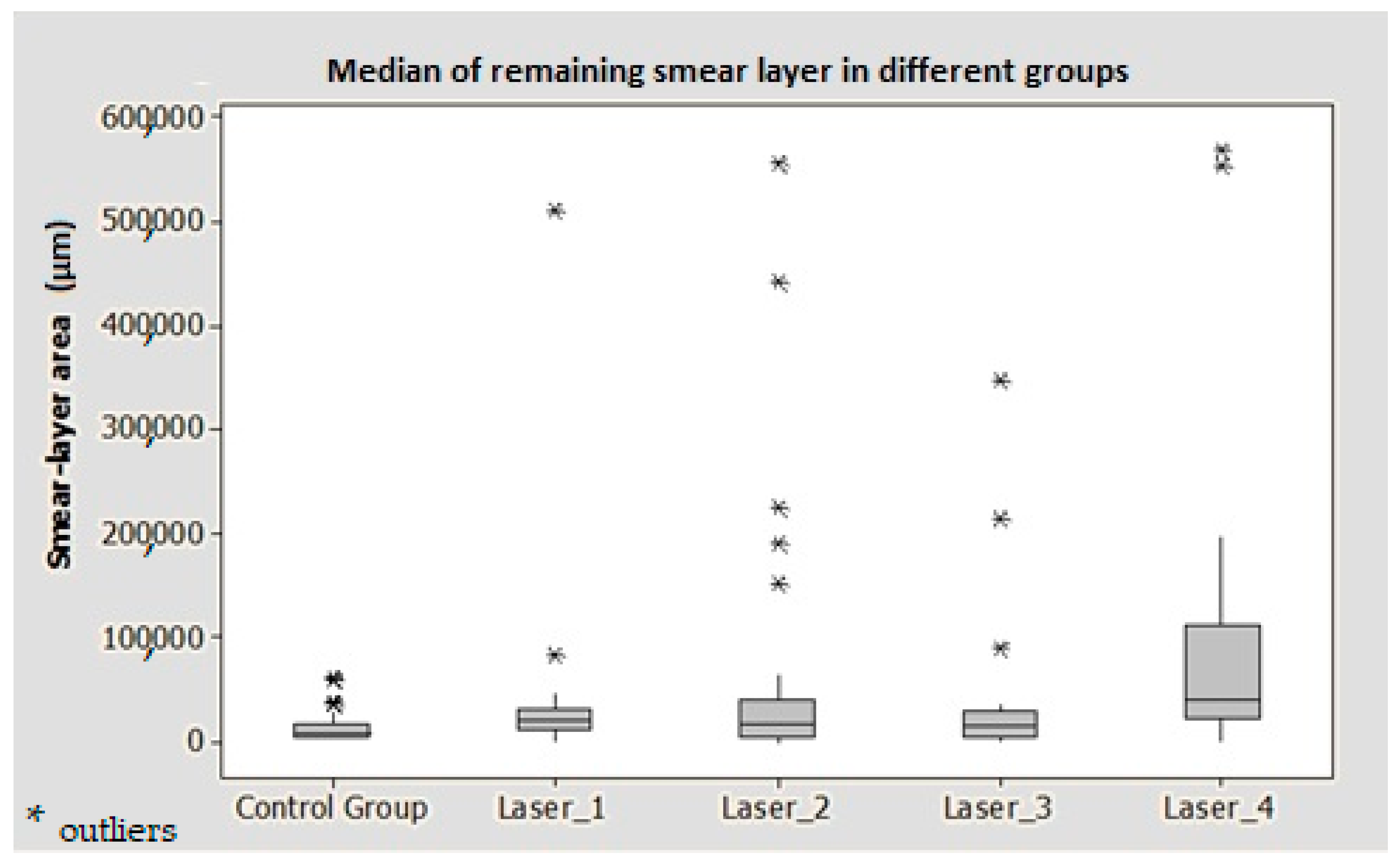
3.1. Remaining Smear Layer Area
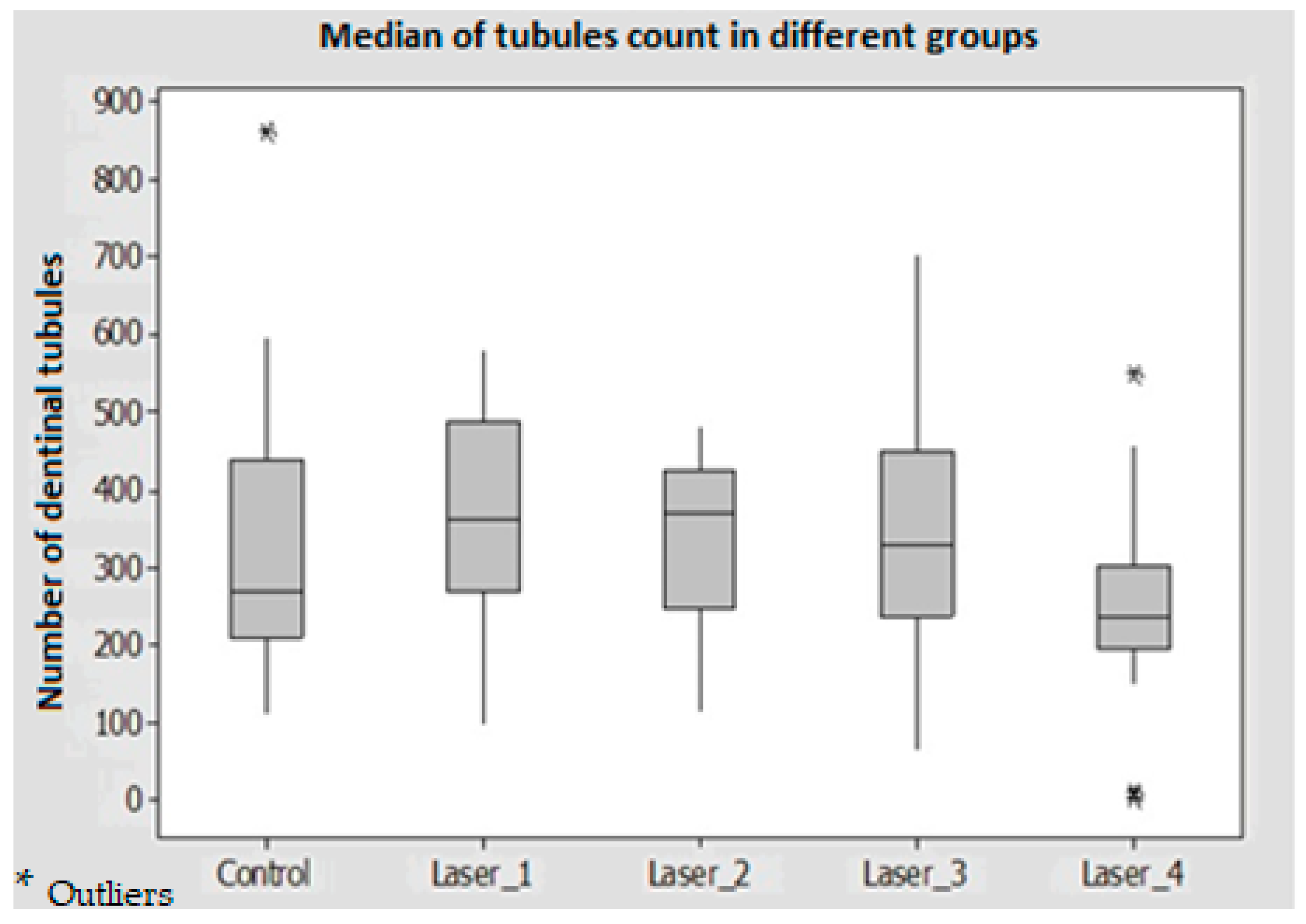
3.2. Count of Exposed Dentinal Tubules
3.3. Count of Debris
3.4. Temperature Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ali, M.; Ahmed, M.A.; Syed, A.U.Y.; Jamil, A.; Khan, S.P.; AlMokhatieb, A.A.; Abdulwahed, A.; Al-Aali, K.A.; Vohra, F.; Abduljabbar, T. Quantitative Evaluation of Apically Extruded Debris of Root Canal Dentin Layer with WaveOne, ProTaper Next, ProTaper Gold Rotary File Systems. Coatings 2022, 12, 451. [Google Scholar] [CrossRef]
- Young, G.R.; Parashos, P.; Messer, H.H. The Principles of Techniques for Cleaning Root Canals. Aust. Dent. J. 2007, 52, S52–S63. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Manoil, D.; Näsman, P.; Belibasakis, G.N.; Neelakantan, P. Microbiological Aspects of Root Canal Infections and Disinfection Strategies: An Update Review on the Current Knowledge and Challenges. Front. Oral Health 2021, 2, 672887. [Google Scholar] [CrossRef]
- Shuping, G.; Sigurdsson, A.; Trope, M. Reduction of Intracanal Bacteria Using NiTi Rotary Instrumentation and Various Medicaments. J. Endod. 1999, 25, 307. [Google Scholar] [CrossRef]
- Almadi, K.H.; Ahmed, M.A.; Ghazal, T.; Jouhar, R.; Alkahtany, M.F.; Abduljabbar, T.; Vohra, F. Antimicrobial Efficacy of Propolis in Comparison to Chlorhexidine against Enterococcus faecalis: A Systematic Review and Meta-Analysis. Appl. Sci. 2021, 11, 3469. [Google Scholar] [CrossRef]
- Al-Nazhan, S.; Al-Sulaiman, A.; Al-Rasheed, F.; Alnajjar, F.; Al-Abdulwahab, B.; Al-Badah, A. Microorganism Penetration in Dentinal Tubules of Instrumented and Retreated Root Canal Walls. In Vitro SEM Study. Restor. Dent. Endod. 2014, 39, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kina, J.R.; Kina, J.; Kina, E.F.U.; Kina, M.; Soubhia, A.M.P. Presence of Bacteria in Dentinal Tubules. J. Appl. Oral Sci. 2008, 16, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, N.; Noiri, Y.; Narimatsu, M.; Ebisu, S. Identification and Localization of Extraradicular Biofilm-Forming Bacteria Associated with Refractory Endodontic Pathogens. Appl. Environ. Microbiol. 2005, 71, 8738–8743. [Google Scholar] [CrossRef] [Green Version]
- Jaju, S.; Jaju, P.P. Newer Root Canal Irrigants in Horizon: A Review. Int. J. Dent. 2011, 2011, 851359. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.; Wang, Z.; Gao, Y. Irrigation in Endodontics. Br. Dent. J. 2014, 216, 299–303. [Google Scholar] [CrossRef]
- Ali, A.; Bhosale, A.; Pawar, S.; Kakti, A.; Bichpuriya, A.; Agwan, M.A. Current Trends in Root Canal Irrigation. Cureus 2022, 14, 1–8. [Google Scholar] [CrossRef]
- Zehnder, M. Root Canal Irrigants. J. Endod. 2006, 32, 389–398. [Google Scholar] [CrossRef]
- Meire, M.A.; Poelman, D.; De Moor, R.J. Optical Properties of Root Canal Irrigants in the 300-3,000-Nm Wavelength Region. Lasers Med. Sci. 2014, 29, 1557–1562. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Yoshimine, Y.; Akamine, A. Visualization of Irrigant Flow and Cavitation Induced by Er:YAG Laser within a Root Canal Model. J. Endod. 2011, 37, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Blanken, J.; De Moor, R.J.G.; Meire, M.; Verdaasdonk, R. Laser Induced Explosive Vapor and Cavitation Resulting in Effective Irrigation of the Root Canal. Part 1: A Visualization Study. Lasers Surg. Med. 2009, 41, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Song, W.D.; Hong, M.H.; Lukyanchuk, B.; Chong, T.C. Laser-Induced Cavitation Bubbles for Cleaning of Solid Surfaces. J. Appl. Phys. 2004, 95, 2952–2956. [Google Scholar] [CrossRef]
- Gu, L.S.; Kim, J.R.; Ling, J.; Choi, K.K.; Pashley, D.H.; Tay, F.R. Review of Contemporary Irrigant Agitation Techniques and Devices. J. Endod. 2009, 35, 791–804. [Google Scholar] [CrossRef]
- Jurič, I.B.; Anić, I. The Use of Lasers in Disinfection and Cleanliness of Root Canals: A Review. Acta Stomatol. Croat. 2014, 48, 6–15. [Google Scholar] [CrossRef]
- Salman, M.I.; Baumann, M.A.; Hellmich, M.; Roggendorf, M.J.; Termaat, S. SEM Evaluation of Root Canal Debridement with Sonicare Canal Brush Irrigation. Int. Endod. J. 2010, 43, 363–369. [Google Scholar] [CrossRef]
- Ciocca, L.; Gallina, I.; Navacchia, E.; Baldissara, P.; Scotti, R. A New Method for Quantitative Analysis of Dentinal Tubules. Comput. Biol. Med. 2007, 37, 277–286. [Google Scholar] [CrossRef]
- De Groot, S.D.; Verhaagen, B.; Versluis, M.; Wu, M.K.; Wesselink, P.R.; Van Der Sluis, L.W.M. Laser-Activated Irrigation within Root Canals: Cleaning Efficacy and Flow Visualization. Int. Endod. J. 2009, 42, 1077–1083. [Google Scholar] [CrossRef]
- Gregorčič, P.; Jezeršek, M.; Možina, J. Optodynamic Energy-Conversion Efficiency during an Er:YAG-Laser-Pulse Delivery into a Liquid through Different Fiber-Tip Geometries. J. Biomed. Opt. 2012, 17, 0750061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moor, R.J.G.D.; Meire, M.; Goharkhay, K. Efficacy of Ultrasonic versus Laser-Activated Irrigation To. J. Endod. 2010, 36, 1580–1583. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Al-Haj, H.; D’Hoedt, B. Intrapulpal Temperature Changes during Root Surface Irradiation with an 809-Nm GaAlAs Laser. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 730–735. [Google Scholar] [CrossRef]
- Bahrololoomi, Z.; Birang, R.; Chiniforush, N.; Yousefshahi, H.; Foroughi, E. Thermal Changes of Root Surface of Anterior Primary Teeth in Pulpectomy with Er:YAG Laser. J. Dent. (Tehran, Iran) 2018, 15, 178–186. [Google Scholar]
- Podolak, B.; Nowicka, A.; Woźniak, K.; Szyszka-Sommerfeld, L.; Dura, W.; Borawski, M.; Dembowska, E.; Lipski, M. Root Surface Temperature Increases during Root Canal Filling in Vitro with Nd:YAG Laser-Softened Gutta-Percha. J. Healthc. Eng. 2020, 2020, 8828272. [Google Scholar] [CrossRef]
- Guidotti, R.; Merigo, E.; Fornaini, C.; Rocca, J.P.; Medioni, E.; Vescovi, P. Er:YAG 2,940-Nm Laser Fiber in Endodontic Treatment: A Help in Removing Smear Layer. Lasers Med. Sci. 2014, 29, 69–75. [Google Scholar] [CrossRef]
- Verma, A.; Yadav, R.; Tikku, A.; Chandra, A.; Shakya, V. Evaluation of Temperature Rise on the External Root Surface during the Application of Laser in Root Canals: An in Vitro Study. Saudi Endod. J. 2020, 10, 28–32. [Google Scholar]
- Farmakis, E.T.R.; Beer, F.; Tzoutzas, I.; Kurzmann, C.; Shokoohi-Tabrizi, H.A.; Pantazis, N.; Moritz, A. Influence of Laser Irradiation Settings, during Diode-Assisted Endodontics, on the Intraradicular Adhesion of Self-Etch and Self-Curing Luting Cement during Restoration—An Ex Vivo Study. Materials 2022, 15, 2531. [Google Scholar] [CrossRef]
- Abad-Gallegos, M.; Arnabat-Domínguez, J.; España-Tost, A.; Berini-Aytés, L.; Gay-Escoda, C. In Vitro Evaluation of the Temperature Increment at the External Root Surface after Er, Cr:YSGG Laser Irradiation of the Root Canal. Med. Oral Patol. Oral Cir. Bucal 2009, 14, 658–662. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Classification of Remaining Smear Layer Area |
|---|---|
| Score 1 | The smear layer covers < 25% of the total area |
| Score 2 | The smear layer covers 25–49% of the total area |
| Score 3 | The smear layer covers 50–74% of the total area |
| Score 4 | The smear layer covers > 75% of the total area |
| Groups | Remaining Smear Layer | Exposed Dentinal Tubules | Count of Debris | |
|---|---|---|---|---|
| Laser 1 | 0.040 * | 0.779 | 0.607 | |
| Control Group (Ultrasonic) | Laser 2 | 0.431 | 0.996 | 0.999 |
| Laser 3 | 0.634 | 0.988 | 0.232 | |
| Laser 4 | 0.000 * | 0.067 | 0.001 * |
| Groups | p-Value | |
|---|---|---|
| Laser 1 (Flat × 10 s) | Laser 2 (Taper × 10 s) | 1.000 |
| Laser 1 (Flat × 10 s) | Laser 3 (Flat × 20 s) | 0.041 * |
| Laser 1 (Flat × 10 s) | Laser 4 (Taper × 20 s) | 0.000 * |
| Laser 2 (Taper × 10 s) | Laser 3 (Flat × 20 s) | 0.967 |
| Laser 2 (Taper × 10 s) | Laser 4 (Taper × 20 s) | 0.005 * |
| Laser 3 (Flat × 20 s) | Laser 4 (Taper × 20 s) | 0.627 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habshi, A.Y.; Aga, N.; Habshi, K.Y.; Hassan, M.E.M.; Choudhry, Z.; Ahmed, M.A.; Syed, A.U.Y.; Jouhar, R. Efficacy of Smear Layer Removal at the Apical One-Third of the Root Using Different Protocols of Erbium-Doped Yttrium Aluminium Garnet (Er:YAG) Laser. Medicina 2023, 59, 433. https://doi.org/10.3390/medicina59030433
Habshi AY, Aga N, Habshi KY, Hassan MEM, Choudhry Z, Ahmed MA, Syed AUY, Jouhar R. Efficacy of Smear Layer Removal at the Apical One-Third of the Root Using Different Protocols of Erbium-Doped Yttrium Aluminium Garnet (Er:YAG) Laser. Medicina. 2023; 59(3):433. https://doi.org/10.3390/medicina59030433
Chicago/Turabian StyleHabshi, Amel Yousif, Nausheen Aga, Khadija Yousif Habshi, Muna Eisa Mohamed Hassan, Ziaullah Choudhry, Muhammad Adeel Ahmed, Azeem Ul Yaqin Syed, and Rizwan Jouhar. 2023. "Efficacy of Smear Layer Removal at the Apical One-Third of the Root Using Different Protocols of Erbium-Doped Yttrium Aluminium Garnet (Er:YAG) Laser" Medicina 59, no. 3: 433. https://doi.org/10.3390/medicina59030433