
Mixed Primary Hepatocellular Carcinoma and Hepatic Neuroendocrine Carcinoma: Case Report and Literature Review

Abstract
:1. Introduction
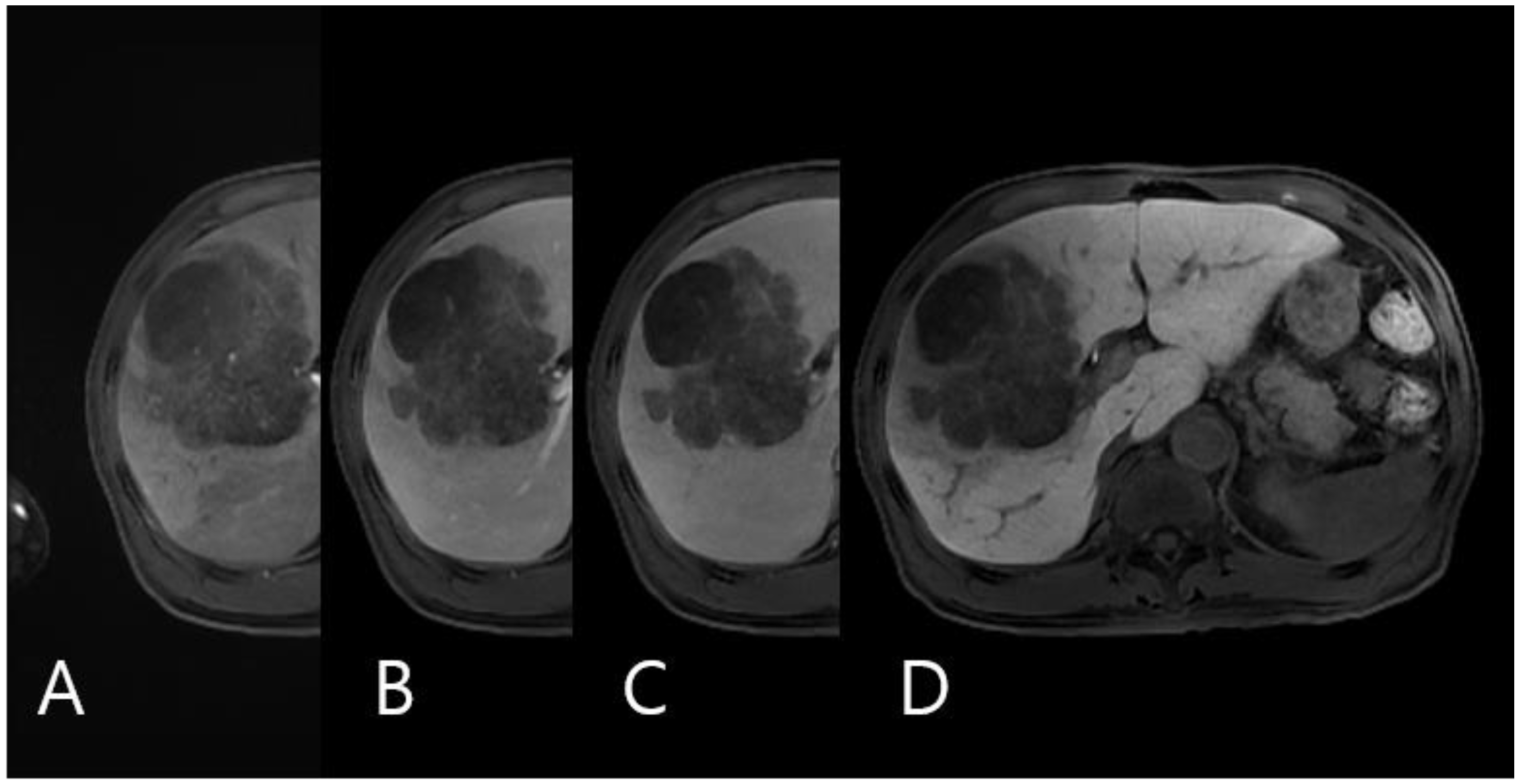
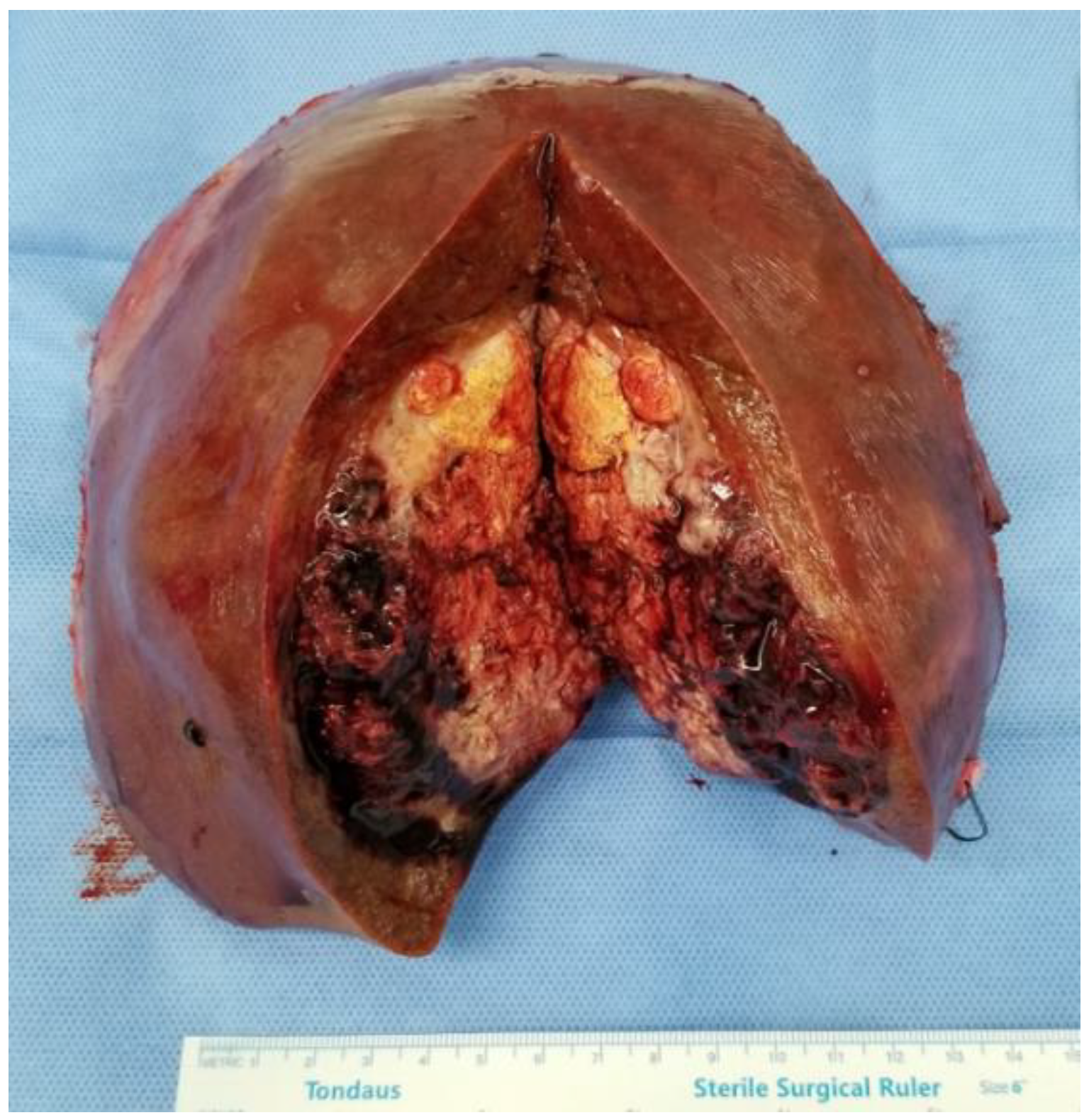
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nomura, Y.; Nakashima, O.; Akiba, J.; Ogasawara, S.; Fukutomi, S.; Yamaguchi, R.; Kusano, H.; Kage, M.; Okuda, K.; Yano, H. Clinicopathological features of neoplasms with neuroendocrine differentiation occurring in the liver. J. Clin. Pathol. 2017, 70, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Jarnagin, W.R.; Weber, S.; Tickoo, S.K.; Koea, J.B.; Obiekwe, S.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; Klimstra, D. Combined hepatocellular and cholangiocarcinoma: Demographic, clinical, and prognostic factors. Cancer 2002, 94, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Nakano, A.; Hirabayashi, K.; Yamamuro, H.; Mashiko, T.; Masuoka, Y.; Yamamoto, S.; Ozawa, S.; Nakagohri, T. Combined primary hepatic neuroendocrine carcinoma and hepatocellular carcinoma: Case report and literature review. World J. Surg. Oncol. 2021, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Barsky, S.H.; Linnoila, I.; Triche, T.J.; Costa, J. Hepatocellular carcinoma with carcinoid features. Hum. Pathol. 1984, 15, 892–894. [Google Scholar] [CrossRef]
- Artopoulos, J.G.; Destuni, C. Primary mixed hepatocellular carcinoma with carcinoid characteristics. A case report. Hepatogastroenterology 1994, 41, 442–444. [Google Scholar]
- Vora, I.M.; Amarapurkar, A.D.; Rege, J.D.; Mathur, S.K. Neuroendocrine differentiation in hepatocellular carcinoma. Indian J. Gastroenterol. Off. J. Indian Soc. Gastroenterol. 2000, 19, 37–38. [Google Scholar]
- Ishida, M.; Seki, K.; Tatsuzawa, A.; Katayama, K.; Hirose, K.; Azuma, T.; Imamura, Y.; Abraham, A.; Yamaguchi, A. Primary hepatic neuroendocrine carcinoma coexisting with hepatocellular carcinoma in hepatitis C liver cirrhosis: Report of a case. Surg. Today 2003, 33, 214–218. [Google Scholar] [CrossRef]
- Yamaguchi, R.; Nakashima, O.; Ogata, T.; Hanada, K.; Kumabe, T.; Kojiro, M. Hepatocellular carcinoma with an unusual neuroendocrine component. Pathol. Int. 2004, 54, 861–865. [Google Scholar] [CrossRef]
- Garcia, M.T.; Bejarano, P.A.; Yssa, M.; Buitrago, E.; Livingstone, A. Tumor of the liver (hepatocellular and high grade neuroendocrine carcinoma): A case report and review of the literature. Virchows Arch. 2006, 449, 376–381. [Google Scholar] [CrossRef]
- Yang, C.S.; Wen, M.C.; Jan, Y.J.; Wang, J.; Wu, C.C. Combined primary neuroendocrine carcinoma and hepatocellular carcinoma of the liver. J. Chin. Med. Assoc. 2009, 72, 430–433. [Google Scholar] [CrossRef] [Green Version]
- Tazi, E.M.; Essadi, I.; M’Rabti, H.; Errihani, H. Hepatocellular Carcinoma and High Grade Neuroendocrine Carcinoma: A Case Report and Review of the Literature. World J. Oncol. 2011, 2, 37–40. [Google Scholar] [PubMed] [Green Version]
- Nakanishi, C.; Sato, K.; Ito, Y.; Abe, T.; Akada, T.; Muto, R.; Sakashita, K.; Konno, T.; Kato, H.; Satomi, S. Combined hepatocellular carcinoma and neuroendocrine carcinoma with sarcomatous change of the liver after transarterial chemoembolization. Hepatol. Res. 2012, 42, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Hammedi, F.; Rammah, S.; Trabelsi, A.; Bdioui, A.; Jomaa, W.; Anjorin, A.; Bakir, D.; Mokni, M. Carcinome hépatocellulaire avec composante neuroendocrine: À propos d’un cas. Afr. J. Cancer 2012, 4, 120–123. [Google Scholar] [CrossRef]
- Aboelenen, A.; El-Hawary, A.K.; Megahed, N.; refaat Zalata, K.; El-Salk, E.M.; Fattah, M.A.; El Sorogy, M.; Shehta, A. Right hepatectomy for combined primary neuroendocrine and hepatocellular carcinoma. A case report. Int. J. Surg. Case Rep. 2014, 5, 26–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishino, H.; Hatano, E.; Seo, S.; Shibuya, S.; Anazawa, T.; Iida, T.; Masui, T.; Taura, K.; Haga, H.; Uemoto, S. Histological features of mixed neuroendocrine carcinoma and hepatocellular carcinoma in the liver: A case report and literature review. Clin. J. Gastroenterol. 2016, 9, 272–279. [Google Scholar] [CrossRef]
- Yun, E.Y.; Kim, T.H.; Lee, S.S.; Kim, H.J.; Kim, H.J.; Jung, W.T.; Lee, O.J.; Song, D.H. A Case of Composite Hepatocellular Carcinoma and Neuroendocrine Carcinoma in a Patient with Liver Cirrhosis Caused by Chronic Hepatitis B. Korean J. Gastroenterol. 2016, 68, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Choi, G.H.; Ann, S.Y.; Lee, S.I.; Kim, S.B.; Song, I.H. Collision tumor of hepatocellular carcinoma and neuroendocrine carcinoma involving the liver: Case report and review of the literature. World J. Gastroenterol. 2016, 22, 9229–9234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beard, R.E.; Finkelstein, S.D.; Borhani, A.A.; Minervini, M.I.; Marsh, J.W. A massive hepatic tumor demonstrating hepatocellular, cholangiocarcinoma and neuroendocrine lineages: A case report and review of the literature. Int. J. Surg. Case Rep. 2017, 37, 26–32. [Google Scholar] [CrossRef]
- Baker, E.; Jacobs, C.; Martinie, J.; Iannitti, D.A.; Vrochides, D.; Swan, R.Z. Mixed Hepatocellular Carcinoma, Neuroendocrine Carcinoma of the Liver. Am. Surg. 2016, 82, 1121–1125. [Google Scholar] [CrossRef]
- Liu, Y.J.; Ng, K.F.; Huang, S.C.; Wu, R.C.; Chen, T.C. Composite hepatocellular carcinoma and small cell carcinoma with early nodal metastasis: A case report. Medicine 2017, 96, e7868. [Google Scholar] [CrossRef]
- Okumura, Y.; Kohashi, K.; Wang, H.; Kato, M.; Maehara, Y.; Ogawa, Y.; Oda, Y. Combined primary hepatic neuroendocrine carcinoma and hepatocellular carcinoma with aggressive biological behavior (adverse clinical course): A case report. Pathol. Res. Pract. 2017, 213, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.G.; Farukhi, M.A.; Mayeda, D.; French, S.W. Hepatocellular carcinoma with neuroendocrine differentiation: A case report. Exp. Mol. Pathol. 2017, 103, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, D.B.; Bayramoglu, Z.; Unay, G.; Ayik, E.; Bassorgun, C.I.; Elpek, G.O. Incidental Collision Tumor of Hepatocellular Carcinoma and Neuroendocrine Carcinoma. J. Clin. Transl. Hepatol. 2018, 6, 339–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, A.; Aoki, K.; Terashima, T.; Itokawa, Y.; Kokuryu, H. A fat containing combined neuroendocrine carcinoma and hepatocellular carcinoma in the liver: A case report. Ann. Hepatol. 2021, 22, 100183. [Google Scholar] [CrossRef]
- Kwon, H.J.; Kim, J.W.; Kim, H.; Choi, Y.; Ahn, S. Combined Hepatocellular Carcinoma and Neuroendocrine Carcinoma with Ectopic Secretion of Parathyroid Hormone: A Case Report and Review of the Literature. J. Pathol. Transl. Med. 2018, 52, 232–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahan, N.; Warraich, I.; Onkendi, E.; Awasthi, S. Mixed hepatocellular carcinoma-neuroendocrine carcinoma—A diagnostic and therapeutic challenge. Curr. Probl. Cancer Case Rep. 2020, 1, 100020. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age/Sex | Tumor Size (cm) | Type | Initial Treatment | Recurrence | Survival | |
|---|---|---|---|---|---|---|
| Barsky et al. [4] | 43/M | Large | Combined | Palliative CTx d/t omental seeding | Dead (26 mon) | |
| Artopoulos et al. [5] | 69/M | 10 | Combined | Resection | NA | NA |
| Vora et al. [6] | 63/M | 10 | Combined | Resection | NA | Dead (1 mon) |
| Ishida et al. [7] | 72/M | 3 | Collision | Resection | NA | NA |
| Yamaguchi et al. [8] | 71/M | 4.1 | Combined | Resection | Recurrence (bone, 5 mon) | Alive (F/U 5 mon) |
| Garcia et al. [9] | 50/M | 5.3 | Collision | Resection | Recurrence (liver, peritoneum 4 mon) | Alive (F/U 16 mon) |
| Yang et al. [10] | 65/M | 7.5 | Combined | Resection | Recurrence (liver and adrenal, LN 4 mon) | Dead (12 mon) |
| Tazi et al. [11] | 68/M | 4 | Collision | Resection | No recurrence | Alive (F/U 28 mon) |
| Nakanishi et al. [12] | 76/M | 3 | Combined | TACE followed by resection | Recurrence (bone, 7 mon) | Dead (17 mon) |
| Hammedi et al. [13] | 51/M | 20 | Combined | Resection | NA | Dead (1 mon) |
| Aboelenen et al. [14] | 56/F | 7.5 | Combined | Resection | No recurrence | Alive (F/U 6 mon) |
| Nishino et al. [15] | 72/M | 2.5 | Combined | Resection | Recurrence (LN, 0.7 mon) | Dead (2 mon) |
| Yun et al. [16] | 68/F | 2.5 | Combined | Resection | Recurrence (bone, 6 mon) | Dead (13 mon) |
| Choi et al. [17] | 72/M | 2.5 | Collision | Resection | Recurrence (liver, 6 mon) | Alive (F/U 10 mon) |
| Beard et al. [18] | 19/M | 25 | Combined | Resection | Recurrence (LN, 4 mon) | Alive (F/U 8 mon) |
| Nomura et al. [1] | 71/M | 4 | Combined | Resection | Recurrence (Liver, NA) | Dead (10 mon) |
| 71/M | 3 | Collision | RFA followed by resection | Recurrence (Liver, NA) | Dead (8.6 mon) | |
| 58/M | 4.3 | Combined | Resection | No recurrence | Alive (F/U 19.4 mon) | |
| 50/M | 1.8 | Combined | Resection | No recurrence | Alive (F/U 19.3 mon) | |
| 63/M | 3 | Combined | Resection | No recurrence | Alive (F/U 23.7 mon) | |
| Baker et al. [19] | 76/M | 5.5 | Collision | Resection | NA | NA |
| Liu et al. [20] | 65/M | 4.3 | Collision | Resection | Hepatic and renal failure | Dead (1.3 mon) |
| Okumura et al. [21] | 70/M | 11 | Mixed | Resection | Recurrence (bone, 1 mon) | Dead (3 mon) |
| Lu et al. [22] | 65/M | 14 | Combined | Hospice | NA | |
| Yilmaz et al. [23] | 56/M | 2.3 | Collision | Resection | No recurrence | Alive (F/U 10 mon) |
| Ikeda et al. [24] | 79/M | 6 | Combined | Resection | Recurrence (NA, 4 mon) | Dead (4 mon) |
| Kwon et al. [25] | 44/M | 10.5 | Combined | Resection | Recurrence (liver and bone, 1.9 mon) | Dead (4 mon) |
| Jahan et al. [26] | 50/M | 2.7 | Combined | Resection | Recurrence (liver, LN, and bone, 13 mon) | Dead (33 mon) |
| Nakano et al. [3] | 84/F | 5.5 | Combined | Resection | No recurrence | Alive (F/U 9 mon) |
| Present case | 63/M | 9 | Combined | Resection | Recurrence (adrenal, liver, and lung, 5 mon) | Dead (12 mon) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, W.Y.; Lee, K.Y.; Kim, K.D. Mixed Primary Hepatocellular Carcinoma and Hepatic Neuroendocrine Carcinoma: Case Report and Literature Review. Medicina 2023, 59, 418. https://doi.org/10.3390/medicina59020418
Shin WY, Lee KY, Kim KD. Mixed Primary Hepatocellular Carcinoma and Hepatic Neuroendocrine Carcinoma: Case Report and Literature Review. Medicina. 2023; 59(2):418. https://doi.org/10.3390/medicina59020418
Chicago/Turabian StyleShin, Woo Young, Keon Young Lee, and Kyeong Deok Kim. 2023. "Mixed Primary Hepatocellular Carcinoma and Hepatic Neuroendocrine Carcinoma: Case Report and Literature Review" Medicina 59, no. 2: 418. https://doi.org/10.3390/medicina59020418