
Extremely Low Activity of Serum Alanine Aminotransferase Is Associated with Long-Term Overall-Cause Mortality in the Elderly Patients Undergoing Percutaneous Coronary Intervention after Acute Coronary Syndrome


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Size Calculation
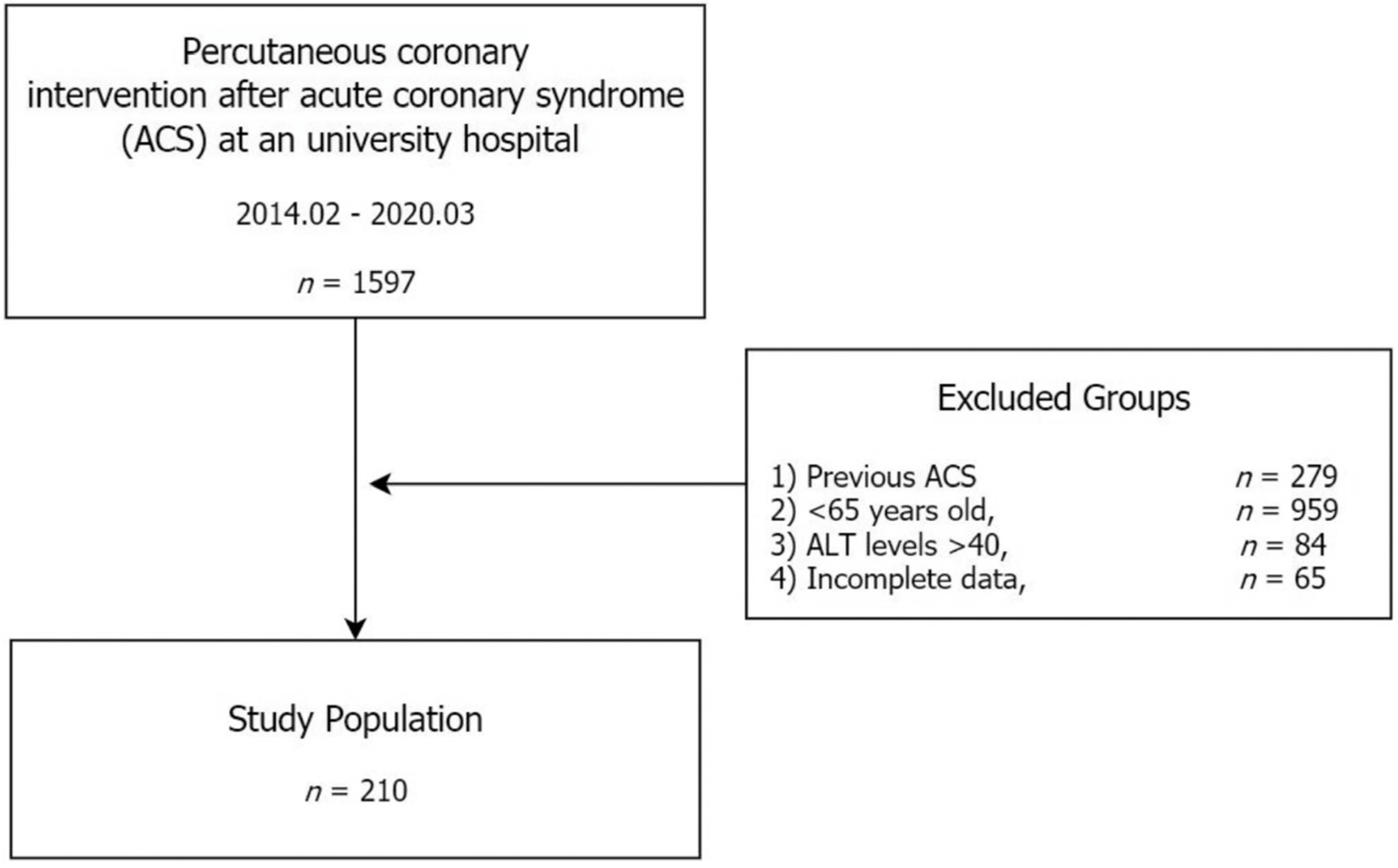
2.2. Participants
2.3. Clinical Data
2.4. Statistical Analyses
3. Results
3.1. Clinical Description
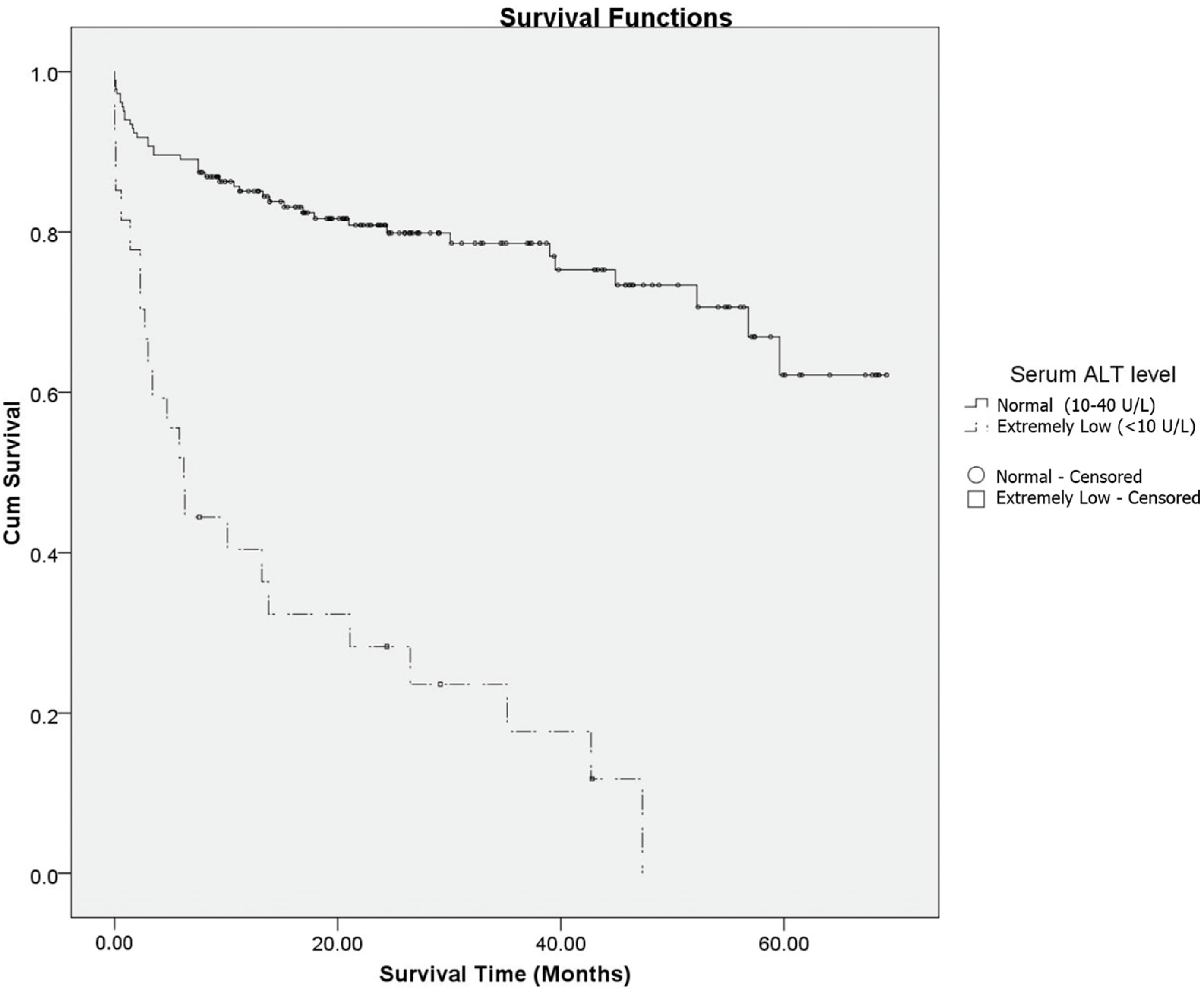
3.2. Survival Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, W.R.; Flamm, S.L.; Di Bisceglie, A.M.; Bodenheimer, H.C. Public Policy Committee of the American Association for the Study of Liver Disease. Serum activity of alanine aminotransferase (ALT) as an indicator of health and disease. Hepatology 2008, 47, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Blyth, F.M.; Creasey, H.M.; Handelsman, D.J.; Naganathan, V.; Sambrook, P.N.; Seibel, M.J.; Waite, L.M.; Cumming, R.G. The association of alanine transaminase with aging, frailty, and mortality. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 712–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, P.E.; Goh, B.G.; Ekstrom, V.; Ong, M.L.; Tan, C.K. Low serum albumin predicts early mortality in patients with severe hypoxic hepatitis. World J. Hepatol. 2017, 9, 959–966. [Google Scholar] [CrossRef]
- Kim, D.Y.; Cho, K.-C. Extremely low serum alanine transaminase level is associated with all-cause mortality in the elderly after intracranial hemorrhage. J. Korean Neurosurg. Soc. 2021, 64, 460–468. [Google Scholar] [CrossRef] [PubMed]
- An, S.J.; Yang, Y.-J.; Jeon, N.-m.; Hong, Y.-P.; Kim, Y.I.; Kim, D.-Y. Significantly reduced alanine aminotransferase level increases all-cause mortality rate in the elderly after ischemic stroke. Int. J. Environ. Res. Public Health 2021, 18, 4915. [Google Scholar] [CrossRef]
- Liu, Z.; Ning, H.; Que, S.; Wang, L.; Qin, X.; Peng, T. Complex association between alanine aminotransferase activity and mortality in general population: A systematic review and meta-analysis of prospective studies. PLoS ONE 2014, 9, e91410. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Baztán, J.J.; Gálvez, C.P.; Socorro, A. Recovery of functional impairment after acute illness and mortality: One-year follow-up study. Gerontology 2009, 55, 269–274. [Google Scholar] [CrossRef]
- Wikman, A.; Bhattacharyya, M.; Perkins-Porras, L.; Steptoe, A. Persistence of posttraumatic stress symptoms 12 and 36 months after acute coronary syndrome. Psychosom. Med. 2008, 70, 764–772. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y. Heart disease and stroke statistics—2022 update: A report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Bawamia, B.; Mehran, R.; Qiu, W.; Kunadian, V. Risk scores in acute coronary syndrome and percutaneous coronary intervention: A review. Am. Heart J. 2013, 165, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Nikolic-Heitzler, V.; Rabuzin, F.; Tatzber, F.; Vrkic, N.; Bulj, N.; Borovic, S.; Wonisch, W.; Sunko, B.M.; Zarkovic, N. Persistent oxidative stress after myocardial infarction treated by percutaneous coronary intervention. Tohoku J. Exp. Med. 2006, 210, 247–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giallauria, F.; Di Lorenzo, A.; Venturini, E.; Pacileo, M.; D’Andrea, A.; Garofalo, U.; De Lucia, F.; Testa, C.; Cuomo, G.; Iannuzzo, G.; et al. Frailty in acute and chronic coronary syndrome patients entering cardiac rehabilitation. J. Clin. Med. 2021, 10, 1696. [Google Scholar] [CrossRef]
- Veronese, N.; Cereda, E.; Stubbs, B.; Solmi, M.; Luchini, C.; Manzato, E.; Sergi, G.; Manu, P.; Harris, T.; Fontana, L.; et al. Risk of cardiovascular disease morbidity and mortality in frail and pre-frail older adults: Results from a meta-analysis and exploratory meta-regression analysis. Ageing Res. Rev. 2017, 35, 63–73. [Google Scholar] [CrossRef] [Green Version]
- Worster, A.; Haines, T. Advanced statistics: Understanding medical record review (MRR) studies. Acad. Emerg. Med. 2004, 11, 187–192. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Pocock, S.J.; McCormack, V.; Gueyffier, F.; Boutitie, F.; Fagard, R.H.; Boissel, J.P. A score for predicting risk of death from cardiovascular disease in adults with raised blood pressure, based on individual patient data from randomised controlled trials. BMJ 2001, 323, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Yashin, A.I.; Manton, K.G.; Vaupel, J.W. Mortality and aging in a heterogeneous population: A stochastic process model with observed and unobserved variables. Theor. Popul. Biol. 1985, 27, 154–175. [Google Scholar] [CrossRef] [Green Version]
- Pyrkov, T.V.; Fedichev, P.O. Biological age is a universal marker of aging, stress, and frailty. In Biomarkers of Human Aging; Moskalev, A., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 23–36. [Google Scholar] [CrossRef]
- Kang, L.; Zhang, S.Y.; Zhu, W.L.; Pang, H.Y.; Zhang, L.; Zhu, M.L.; Liu, X.H.; Liu, Y.T. Is frailty associated with short-term outcomes for elderly patients with acute coronary syndrome? J. Geriatr. Cardiol. 2015, 12, 662–667. [Google Scholar] [CrossRef]
- Rodríguez-Queraltó, O.; Formiga, F.; López-Palop, R.; Marín, F.; Vidán, M.T.; Martínez-Sellés, M.; Díez-Villanueva, P.; Sanchís, J.; Corbí, M.; Aboal, J.; et al. LONGEVO-SCA registry investigators. FRAIL scale also predicts long-term outcomes in older patients with acute coronary syndromes. J. Am. Med. Dir. Assoc. 2020, 21, 683–687.e1. [Google Scholar] [CrossRef]
- Graham, M.M.; Galbraith, P.D.; O’Neill, D.; Rolfson, D.B.; Dando, C.; Norris, C.M. Frailty and outcome in elderly patients with acute coronary syndrome. Can. J. Cardiol. 2013, 29, 1610–1615. [Google Scholar] [CrossRef] [Green Version]
- Kwok, C.S.; Achenbach, S.; Curzen, N.; Fischman, D.L.; Savage, M.; Bagur, R.; Kontopantelis, E.; Martin, G.P.; Steg, P.G.; Mamas, M.A. Relation of frailty to outcomes in percutaneous coronary intervention. Cardiovasc. Revasc. Med. 2020, 21, 811–818. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Dodson, J.A.; Hochman, J.S.; Roe, M.T.; Chen, A.Y.; Chaudhry, S.I.; Katz, S.; Zhong, H.; Radford, M.J.; Udell, J.A.; Bagai, A.; et al. The association of frailty with in-hospital bleeding among older adults with acute myocardial infarction: Insights from the ACTION Registry. JACC Cardiovasc. Interv. 2018, 11, 2287–2296. [Google Scholar] [CrossRef] [PubMed]
- Rauch, B.; Davos, C.H.; Doherty, P.; Saure, D.; Metzendorf, M.I.; Salzwedel, A.; Völler, H.; Jensen, K.; Schmid, J.P.; Cardiac Rehabilitation Section; et al. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies-The Cardiac Rehabilitation Outcome Study (CROS). Eur. J. Prev. Cardiol. 2016, 23, 1914–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.; Choi, Y.; Sajgalik, P.; No, M.H.; Lee, S.H.; Kim, S.; Heo, J.W.; Cho, E.J.; Chang, E.; Kang, J.H.; et al. Exercise as a therapeutic strategy for sarcopenia in heart failure: Insights into underlying mechanisms. Cells 2020, 9, 2284. [Google Scholar] [CrossRef]
- Poh, A.W.Y.; Teo, S.P. Utility of frailty screening tools in older surgical patients. Ann. Geriatr. Med. Res. 2020, 24, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Irina, G.; Refaela, C.; Adi, B.; Avia, D.; Liron, H.; Chen, A.; Gad, S. Low blood ALT activity and high FRAIL questionnaire scores correlate with increased mortality and with each other. A prospective study in the internal medicine department. J. Clin. Med. 2018, 7, 386. [Google Scholar] [CrossRef] [Green Version]
- Segev, A.; Itelman, E.; Beigel, R.; Segal, G.; Chernomordik, F.; Matetzky, S.; Grupper, A. Low ALT levels are associated with poor outcomes in acute coronary syndrome patients in the intensive cardiac care unit. J. Cardiol. 2022, 79, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Eisenberg, M.J.; Morin, J.F.; Bergman, H.; Monette, J.; Noiseux, N.; Perrault, L.P.; Alexander, K.P.; Langlois, Y.; Dendukuri, N.; et al. Gait speed as an incremental predictor of mortality and major morbidity in elderly patients undergoing cardiac surgery. J. Am. Coll. Cardiol. 2010, 56, 1668–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sepehri, A.; Beggs, T.; Hassan, A.; Rigatto, C.; Shaw-Daigle, C.; Tangri, N.; Arora, R.C. The impact of frailty on outcomes after cardiac surgery: A systematic review. J. Thorac. Cardiovasc. Surg. 2014, 148, 3110–3117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arthur, H.M.; Daniels, C.; McKelvie, R.; Hirsh, J.; Rush, B. Effect of a preoperative intervention on preoperative and postoperative outcomes in low-risk patients awaiting elective coronary artery bypass graft surgery. A randomized, controlled trial. Ann. Intern. Med. 2000, 133, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Stammers, A.N.; Kehler, D.S.; Afilalo, J.; Avery, L.J.; Bagshaw, S.M.; Grocott, H.P.; Legare, J.F.; Logsetty, S.; Metge, C.; Nguyen, T.; et al. Protocol for the PREHAB study-Pre-operative Rehabilitation for reduction of Hospitalization After coronary Bypass and valvular surgery: A randomised controlled trial. BMJ Open 2015, 5, e007250. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total (n = 210) | Surviving (n = 146) | Death (n = 64) | p-Value | |
|---|---|---|---|---|
| Age (years) | 76.9 ± 7.6 | 75.2 ± 7.0 | 80.7 ± 7.4 | <0.001 * |
| Survival Time (month) | 25.0 ± 18.9 | 30.6 ± 17.5 | 12.3 ± 15.9 | <0.001 * |
| Sex, n (%) | 0.522 | |||
| -Female | 98 (46.7%) | 66 (45.2%) | 32 (50.0%) | |
| -Male | 112 (53.3%) | 80 (54.8%) | 32 (50.0%) | |
| BMI, n (%) | 0.002 * | |||
| -Reference (18.5–24.9) | 127 (60.5%) | 85 (58.3%) | 42 (65.6%) | |
| -Underweight (<18.5) | 15 (7.1%) | 5 (3.4%) | 10 (15.6%) | |
| -Overweight (25.0–29.9) | 62 (29.4) | 51 (34.9%) | 11 (17.2%) | |
| -Obese (≥30) | 6 (2.9%) | 5 (3.4%) | 1 (1.6%) | |
| Smoking history, n (%) | 0.262 | |||
| -Non-smoker | 144 (68.6%) | 104 (71.2%) | 40 (62.5%) | |
| -Past-smoker | 41 (19.5%) | 28 (19.2%) | 13 (20.3%) | |
| -Current-smoker | 25 (11.9%) | 14 (9.6%) | 11 (17.2%) | |
| Invading vessel, n (%) | 0.639 | |||
| -Single vessel | 165 (78.6%) | 116 (79.5%) | 49 (76.6%) | |
| -Multiple vessels | 45 (21.4% | 30 (20.5%) | 15 (23.4%) | |
| Door-to-PCI time (minutes) | 74.0 ± 20.9 | 72.2 ± 16.6 | 77.9 ± 28.0 | 0.133 |
| ST elevation on ECG, n (%) | 62 (29.5%) | 39 (26.7%) | 23 (35.9%) | 0.177 |
| LVH on echocardiogram, n (%) | 44 (21.0%) | 26 (17.8%) | 18 (28.1%) | 0.091 |
| Initial SBP at diagnosis (mmHg) | 131.2 ± 27.2 | 134.3 ± 25.9 | 124.1 ± 28.7 | 0.012 * |
| Laboratory findings at diagnosis | ||||
| -Extremely low activity of serum ALT (<10 U/L), n (%) | 27 (12.9%) | 4 (2.7%) | 23 (35.9%) | <0.001* |
| -ALT (U/L) | 19.7 ± 8.5 | 20.14 ± 7.8 | 18.8 ± 9.9 | 0.358 |
| -Creatinine (mg/dL) | 1.2 ± 1.0 | 1.1 ± 0.9 | 1.4 ± 1.2 | 0.089 |
| -CRP (mg/L) | 23.2 ± 46.9 | 11.1 ± 27.4 | 50.6 ± 66.9 | <0.001 * |
| -Hb (g/dL) | 12.7 ± 2.1 | 13.1 ± 1.9 | 12.0 ± 2.3 | <0.001 * |
| -Glucose (mg/dL) | 174.9 ± 74.6 | 171.0 ± 73.1 | 183.7 ±77.6 | 0.256 |
| -Total cholesterol (mg/dL) | 161.5 ± 43.7 | 162.7 ± 40.8 | 158.9 ± 49.9 | 0.569 |
| -HDL (mg/dL) | 42.4 ± 9.7 | 43.3 ± 9.4 | 40.19 ± 10.2 | 0.030 * |
| -CK-MB (pg/mL) | 5.7 ± 10.8 | 4.7 ± 10.5 | 8.0 ± 11.2 | 0.043 * |
| -NT-ProBNP (pg/mL) | 886.2 [176.6, 3777] | 444.3 [119.4, 1743] | 3500.5 [983.6, 12766] | <0.001 * |
| -TnI (pg/mL) | 47.9 [9.8, 675.2] | 28.5 [7.9, 213] | 525.4 [25.0, 2219.2] | <0.001 * |
| Underlying diseases | ||||
| -DM, n (%) | 90 (42.9%) | 64 (43.8%) | 26 (40.6%) | 0.665 |
| -Hypertension, n (%) | 145 (69.1%) | 100 (68.5%) | 45 (70.3%) | 0.793 |
| -Chronic kidney disease, n (%) | 15 (7.1%) | 9 (6.2%) | 6 (9.4%) | 0.397 |
| -Cerebrovascular disease, n (%) | 18 (8.6%) | 11 (7.5%) | 7 (10.9%) | 0.417 |
| Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age (years) | 1.062 | 1.016 | 1.110 | 0.008 * |
| Sex (reference; female), n | 1.109 | 0.565 | 2.180 | 0.763 |
| Extremely low activity of serum ALT group (<10 U/L), n | 5.024 | 2.588 | 9.753 | <0.001 * |
| BMI (reference; 18.5–24.9), n | 0.635 | |||
| -Underweight (<18.5) | 1.408 | 0.611 | 3.245 | 0.421 |
| -Overweight (25.0–29.9) | 0.716 | 0.337 | 1.520 | 0.384 |
| -Obese (≥30) | 0.679 | 0.082 | 5.599 | 0.719 |
| Smoking history (reference; non-smoker), n | 0.453 | |||
| -Past-smoker | 1.293 | 0.552 | 3.031 | 0.554 |
| -Current-smoker | 2.432 | 0.594 | 9.964 | 0.217 |
| Invading multiple vessels, n | 0.948 | 0.485 | 1.852 | 0.875 |
| Door-to-PCI time (minutes) | 1.004 | 0.991 | 1.016 | 0.569 |
| ST elevation on ECG, n | 1.163 | 0.603 | 2.243 | 0.652 |
| LVH on echocardiogram, n | 1.287 | 0.678 | 2.445 | 0.441 |
| Initial SBP at diagnosis (mmHg) | 0.991 | 0.979 | 1.003 | 0.158 |
| Laboratory findings at diagnosis | ||||
| -Low level Hb group (<11 g/dL) | 1.093 | 0.570 | 2.098 | 0.789 |
| -Low level HDL group (<40 mg/dL) | 1.111 | 0.584 | 2.114 | 0.749 |
| -Total cholesterol (mg/dL) | 1.007 | 0.999 | 1.014 | 0.078 |
| -Creatinine (mg/dL) | 0.904 | 0.665 | 1.229 | 0.519 |
| -CRP (mg/L) | 1.002 | 0.996 | 1.008 | 0.561 |
| -Glucose (mg/dL) | 0.999 | 0.995 | 1.003 | 0.504 |
| -CK-MB (pg/mL) | 1.010 | 0.984 | 1.036 | 0.454 |
| -NT-ProBNP (pg/mL) | 1.000 | 1.000 | 1.000 | 0.021 * |
| -TnI (pg/mL) | 1.000 | 1.000 | 1.000 | 0.680 |
| Underlying diseases | ||||
| -DM, n | 1.225 | 0.590 | 2.541 | 0.586 |
| -Hypertension, n | 1.457 | 0.735 | 2.890 | 0.281 |
| -Chronic kidney disease, n | 2.864 | 0.848 | 9.674 | 0.090 |
| -Cerebrovascular disease, n | 1.851 | 0.708 | 4.841 | 0.209 |
| Adjusted Hazard Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Extremely low activity of serum ALT group (<10 U/L), n | 5.157 | 3.001 | 8.862 | <0.001 * |
| CRP (mg/L) | 1.006 | 1.001 | 1.011 | 0.010 * |
| NT-ProBNP (pg/mL) | 1.000 | 1.000 | 1.000 | 0.003 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.Y.; Park, S.-W.; Han, H.-W.; Kim, M.-K.; Kim, H.-J. Extremely Low Activity of Serum Alanine Aminotransferase Is Associated with Long-Term Overall-Cause Mortality in the Elderly Patients Undergoing Percutaneous Coronary Intervention after Acute Coronary Syndrome. Medicina 2023, 59, 415. https://doi.org/10.3390/medicina59020415
Kim DY, Park S-W, Han H-W, Kim M-K, Kim H-J. Extremely Low Activity of Serum Alanine Aminotransferase Is Associated with Long-Term Overall-Cause Mortality in the Elderly Patients Undergoing Percutaneous Coronary Intervention after Acute Coronary Syndrome. Medicina. 2023; 59(2):415. https://doi.org/10.3390/medicina59020415
Chicago/Turabian StyleKim, Doo Young, Si-Woon Park, Hyung-Wook Han, Myeong-Kon Kim, and Ha-Jung Kim. 2023. "Extremely Low Activity of Serum Alanine Aminotransferase Is Associated with Long-Term Overall-Cause Mortality in the Elderly Patients Undergoing Percutaneous Coronary Intervention after Acute Coronary Syndrome" Medicina 59, no. 2: 415. https://doi.org/10.3390/medicina59020415