
Emergency Management of Electrical Storm: A Practical Overview
 , ,
, ,
Abstract
:1. Introduction
1.1. Definition
1.2. Incidence, Basic Epidemiological Aspects and Risk Factors
1.3. Prognosis
2. Causes
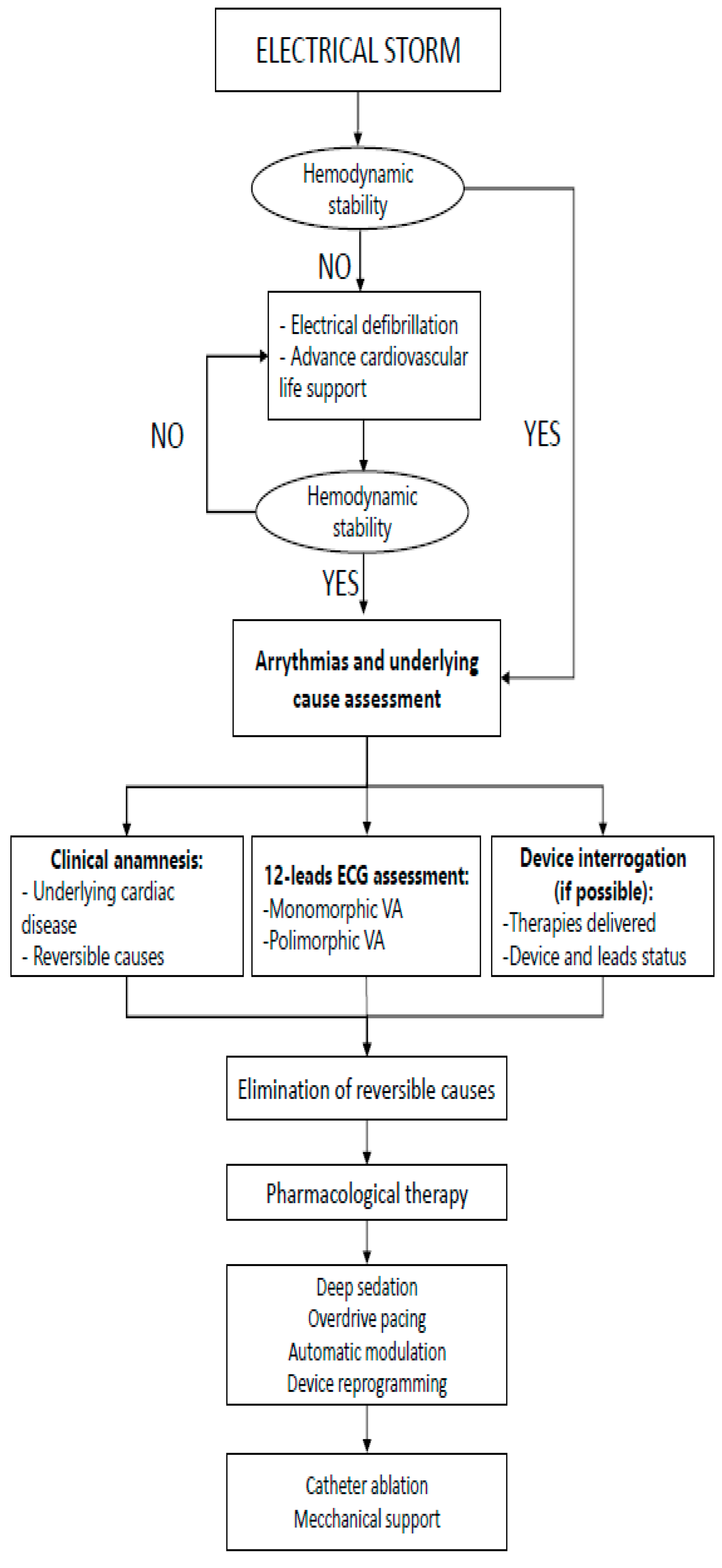
3. Early Evaluation and Acute Management
3.1. ECG 12 Lead Evaluation
3.2. Reversible Causes Treatment
3.3. Device (ICD) Interrogation and Reprogramming
4. Medical Therapy
4.1. Sodium-Channel Blockers (Class I)
- Class Ia (Quinidine)
- Class Ib (Mexiletine and Lidocaine)
- Class Ic (Procainamide, Flecainide and Propafenone)
4.2. Beta Blockers (Class II)
4.3. Amiodarone and Sotalol (Class III)
4.4. Calcium Channel Blockers (Class IV)
4.5. Alternative Drugs
5. Catheter Ablation
6. Neuraxial Modulation
7. Bailout Therapies
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death Developed by the task force for the management of patients with death of the European Society of Cardiology (ESC) Endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [PubMed]
- Gao, D.; Sapp, J.L. Electrical storm: Definitions, clinical importance, and treatment. Curr. Opin. Cardiol. 2013, 28, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hohnloser, S.H.; Al-Khalidi, H.R.; Pratt, C.M.; Brum, J.M.; Tatla, D.S.; Tchou, P.; Dorian, P. Electrical storm in patients with an implantable defibrillator: Incidence, features, and preventive therapy: Insights from a randomized trial. Eur. Heart J. 2006, 27, 3027–3032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.T.; Traub, D. Recurrent Ventricular Arrhythmia Storms in the Age of Implantable Cardioverter Defibrillator Therapy: A Comprehensive Review. Prog. Cardiovasc. Dis. 2008, 51, 229–236. [Google Scholar] [CrossRef]
- Nattel, S.; Maguy, A.; Le Bouter, S.; Yeh, Y.H. Arrhythmogenic ion-channel remodeling in the heart: Heart failure, myocardial infarction, and atrial fibrillation. Physiol. Rev. 2007, 87, 425–456. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Shkoza, M.; Scappini, L.; Flori, M.; Capucci, A. Role of electrical storm as a mortality and morbidity risk factor and its clinical predictors: A meta-analysis. Europace 2014, 16, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Stuber, T.; Eigenmann, C.; Delacrétaz, E. Characteristics and relevance of clustering ventricular arrhythmias in defibrillator recipients. Pacing Clin. Electrophysiol. 2005, 28, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Israel, C.W.; Serge Barold, S. Electrical storm in patients with an implanted defibrillator: A matter of definition. Ann. Noninvasive Electrocardiol. 2007, 12, 375–382. [Google Scholar] [CrossRef]
- Nayyar, S.; Ganesan, A.N.; Brooks, A.G.; Sullivan, T.; Roberts-Thomson, K.C.; Sanders, P. Venturing into ventricular arrhythmia storm: A systematic review and meta-analysis. Eur. Heart J. 2013, 34, 560–571. [Google Scholar] [CrossRef]
- Elsokkari, I.; Sapp, J.L. Electrical storm: Prognosis and management. Prog. Cardiovasc. Dis. 2021, 66, 70–79. [Google Scholar] [CrossRef]
- Friedman, D.J.; Altman, R.K.; Orencole, M.; Picard, M.H.; Ruskin, J.N.; Singh, J.P. Heist EKPredictors of sustained ventricular arrhythmias in cardiac resynchronization therapy. Circ. Arrhythmia Electrophysiol. 2012, 5, 762–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Credner, S.C.; Klingenheben, T.; Mauss, O.; Sticherling, C.; Hohnloser, S.H. Electrical storm in patients with transvenous implantable cardioverter- defibrillators: Incidence, management and prognostic implications. J. Am. Coll. Cardiol. 1998, 32, 1909–1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Exner, D.V.; Pinski, S.L.; Wyse, D.G.; Renfroe, E.G.; Follmann, D.; Gold, M.; Beckman, K.J.; Coromilas, J.; Lancaster, S.; Hallstrom, A.P. Electrical storm presages nonsudden death: The antiarrhythmics versus implantable defibrillators (AVID) trial. Circulation 2001, 103, 2066–2071. [Google Scholar] [CrossRef] [Green Version]
- Brigadeau, F.; Kouakam, C.; Klug, D.; Marquié, C.; Duhamel, A.; Mizon-Gérard, F.; Lacroix, D.; Kacet, S. Clinical predictors and prognostic significance of electrical storm in patients with implantable cardioverter defibrillators. Eur. Heart J. 2006, 27, 700–707. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A.; et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. Eur. J. Heart Fail. 2012, 14, 803–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trappe, H.J.; Brugada, P.; Talajic, M.; Della Bella, P.; Lezaun, R.; Mulleneers, R.; Wellens, H.J. Prognosis of patients with ventricular tachycardia and ventricular fibrillation: Role of the underlying etiology. J. Am. Coll. Cardiol. 1988, 12, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Pires, L.A.; Lehmann, M.H.; Steinman, R.T.; Baga, J.J.; Schuger, C.D. Sudden death in implantable cardioverter-defibrillator recipients: Clinical context, arrhythmic events and device responses. J. Am. Coll. Cardiol. 1999, 33, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Bänsch, D.; Böcker, D.; Brunn, J.; Weber, M.; Breithardt, G.; Block, M. Clusters of ventricular tachycardias signify impaired survival in patients with idiopathic dilated cardiomyopathy and implantable cardioverter defibrillators. J. Am. Coll. Cardiol. 2000, 36, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, M.O.; Sherfesee, L.; DeGroot, P.J.; Wathen, M.S.; Wilkoff, B.L. Differences in effects of electrical therapy type for ventricular arrhythmias on mortality in implantable cardioverter-defibrillator patients. Heart Rhythm 2010, 7, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Runsiö, M.; Bergfeldt, L.; Brodin, L.A.; Ribeiro, A.; Samuelsson, S.; Rosenqvist, M. Left ventricular function after repeated episodes of ventricular fibrillation and defibrillation assessed by transoesophageal echocardiography. Eur. Heart J. 1997, 18, 124–131. [Google Scholar] [CrossRef] [Green Version]
- lsokkari, I.; Parkash, R.; Tang, A.; Wells, G.; Doucette, S.; Yetisir, E.; Gardner, M.; Healey, J.S.; Thibault, B.; Sterns, L.; et al. Mortality Risk Increases With Clustered Ventricular Arrhythmias in Patients With Implantable Cardioverter-Defibrillators. JACC Clin. Electrophysiol. 2020, 6, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Sesselberg, H.W.; Moss, A.J.; McNitt, S.; Zareba, W.; Daubert, J.P.; Andrews, M.L.; Hall, W.J.; McClinitic, B. Huang DTVentricular arrhythmia storms in postinfarction patients with implantable defibrillators for primary prevention indications: A MADIT-II substudy. Heart Rhythm 2007, 4, 1395–1402. [Google Scholar] [CrossRef]
- Carbucicchio, C.; Santamaria, M.; Trevisi, N.; Maccabelli, G.; Giraldi, F.; Fassini, G.; Riva, S.; Moltrasio, M.; Cireddu, M.; Veglia, F.; et al. Catheter ablation for the treatment of electrical storm in patients with implantable cardioverter-defibrillators: Short-and long-term outcomes in a prospective single-center study. Circulation 2008, 117, 462–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deneke, T.; Shin, D.I.; Lawo, T.; Bösche, L.; Balta, O.; Anders, H.; Bünz, K.; Horlitz, M.; Grewe, P.H.; Lemke, B.; et al. Catheter ablation of electrical storm in a collaborative hospital network. Am. J. Cardiol. 2011, 108, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, Y.; Hocini, M.; Nogami, A.; Maury, P.; Peichl, P.; Iwasaki, Y.K.; Masuda, K.; Denis, A.; Voglimacci-Stephanopoli, Q.; Wichterle, D.; et al. Catheter Ablation of Refractory Ventricular Fibrillation Storm after Myocardial Infarction: A Multicenter Study. Circulation 2019, 139, 2315–2325. [Google Scholar] [CrossRef]
- Logantha, S.J.R.J.; Cai, X.J.; Yanni, J.; Jones, C.B.; Stephenson, R.S.; Stuart, L.; Quigley, G.; Monfredi, O.; Nakao, S.; Oh, I.Y.; et al. Remodeling of the Purkinje Network in Congestive Heart Failure in the Rabbit. Circ. Heart Fail. 2021, 14, e007505. [Google Scholar] [CrossRef]
- Yamaguchi, J.; Takigawa, M.; Tao, S.; Takahashi, Y.; Goya, M.; Sasano, T. Successful Substrate Ablation for Ventricular Fibrillation in a Patient With Nonischemic Cardiomyopathy. JACC Case Rep. 2021, 3, 1091–1096. [Google Scholar] [CrossRef]
- Arya, A.; Haghjoo, M.; Dehghani, M.R.; Fazelifar, A.F.; Nikoo, M.H.; Bagherzadeh, A. Sadr-Ameli MAPrevalence and predictors of electrical storm in patients with implantable cardioverter-defibrillator. Am. J. Cardiol. 2006, 97, 389–392. [Google Scholar] [CrossRef]
- Sapp, J.L.; Parkash, R.; Wells, G.A.; Yetisir, E.; Gardner, M.J.; Healey, J.S.; Thibault, B.; Sterns, L.D.; Birnie, D.; Nery, P.B.; et al. Cardiac resynchronization therapy reduces ventricular arrhythmias in primary but not secondary prophylactic implantable cardioverter defibrillator patients: Insight from the resynchronization in ambulatory heart failure trial. Circ. Arrhythmia Electrophysiol. 2017, 10, e004875. [Google Scholar] [CrossRef]
- Deif, B.; Ballantyne, B.; Almehmadi, F.; Mikhail, M.; McIntyre, W.F.; Manlucu, J.; Yee, R.; Sapp, J.L.; Roberts, J.D.; Healey, J.S.; et al. Cardiac resynchronization is pro-arrhythmic in the absence of reverse ventricular remodelling: A systematic review and meta-analysis. Cardiovasc. Res. 2018, 114, 1435–1444. [Google Scholar] [CrossRef] [Green Version]
- Elsokkari, I.; Tsuji, Y.; Sapp, J.L.; Nattel, S. Recent Insights Into Mechanisms and Clinical Approaches to Electrical Storm. Can. J. Cardiol. 2022, 38, 439–453. [Google Scholar] [CrossRef]
- Ninni, S.; Layec, J.; Brigadeau, F.; Behal, H.; Labreuche, J.; Klein, C.; Schurtz, G.; Potelle, C.; Coisne, A.; Lemesle, G.; et al. Incidence and predictors of mortality after an electrical storm in the ICU. Eur. Heart J. Acute Cardiovasc. Care. 2022, 11, 431–439. [Google Scholar] [CrossRef]
- Gadula-Gacek, E.; Tajstra, M.; Niedziela, J.; Pyka, Ł.; Gąsior, M. Characteristics and Outcomes in Patients with Electrical Storm. Am. J. Cardiol. 2019, 123, 1637–1642. [Google Scholar] [CrossRef]
- Koizumi, T.; Kamada, R.; Watanabe, M.; Yokoshiki, H.; Temma, T.; Hagiwara, H.; Koya, T.; Nakao, M.; Kadosaka, T.; Natsui, H.; et al. Predictors of cardiovascular mortality after an electrical storm in patients with structural heart disease. J. Cardiol. 2022, 80, 167–171. [Google Scholar] [CrossRef]
- Geraghty, L.; Santangeli, P.; Tedrow, U.B.; Shivkumar, K.; Kumar, S. Contemporary Management of Electrical Storm. Heart Lung Circ. 2019, 28, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madhavan, M.; Friedman, P.A.; Lennon, R.J.; Prasad, A.; White, R.D.; Sriram, C.S.; Gulati, R.; Gersh, B.J. Implantable cardioverter-defibrillator therapy in patients with ventricular fibrillation out of hospital cardiac arrest secondary to acute coronary syndrome. J. Am. Heart Assoc. 2015, 4, e001255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyse, D.G.; Friedman, P.L.; Brodsky, M.A.; Beckman, K.J.; Carlson, M.D.; Curtis, A.B.; Hallstrom, A.P.; Raitt, M.H.; Wilkoff, B.L.; Greene, H.L. AVID Investigators Life-threatening ventricular arrhythmias due to transient or correctable causes: High risk for death in follow-up. J. Am. Coll. Cardiol. 2001, 38, 1718–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, A.; Spertus, J.A.; Gosch, K.; Venkitachalam, L.; Jones, P.G.; Van den Berghe, G.; Kosiborod, M. Serum potassium levels and mortality in acute myocardial infarction. JAMA 2012, 307, 157–164. [Google Scholar] [CrossRef]
- Hoppe, L.K.; Muhlack, D.C.; Koenig, W.; Carr, P.R.; Brenner, H.; Schöttker, B. Association of Abnormal Serum Potassium Levels with Arrhythmias and Cardiovascular Mortality: A Systematic Review and Meta-Analysis of Observational Studies. Cardiovasc. Drugs Ther. 2018, 32, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Ravn Jacobsen, M.; Jabbari, R.; Glinge, C.; Kjær Stampe, N.; Butt, J.H.; Blanche, P.; Lønborg, J.; Wendelboe Nielsen, O.; Køber, L.; Torp-Pedersen, L.; et al. Potassium Disturbances and Risk of Ventricular Fibrillation Among Patients with ST-Segment–Elevation Myocardial Infarction. J. Am. Heart Assoc. 2020, 9, e014160. [Google Scholar] [CrossRef] [PubMed]
- Shao, H.; Shi, D.; Dai, Y. Linezolid and the risk of QT interval prolongation: A pharmacovigilance study of the Food and Drug Administration Adverse Event Reporting System. Br. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, C.; Thalamus, J.; Heldal, K.; Holla, Ø.L.; Haugaa, K.H. Hysing JPredictors of mortality in high-risk patients with QT prolongation in a community hospital. Europace 2018, 20, f99–f107. [Google Scholar] [CrossRef]
- Simpson, T.F.; Salazar, J.W.; Vittinghoff, E.; Probert, J.; Iwahashi, A.; Olgin, J.E.; Ursell, P.; Hart, A.; Moffatt, E.; Tseng, Z.H. Association of QT-Prolonging Medications with Risk of Autopsy-Defined Causes of Sudden Death. JAMA Intern. Med. 2020, 180, 698–706. [Google Scholar] [CrossRef]
- Tsuji, Y.; Heijman, J.; Nattel, S.; Dobrev, D. Electrical storm: Recent pathophysiological insights and therapeutic consequences. Basic Res. Cardiol. 2013, 108, 336. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.J.; Spazzolini, C.; Priori, S.G.; Crotti, L.; Vicentini, A.; Landolina, M.; Gasparini, M.; Wilde, A.A.; Knops, R.E.; Denjoy, I.; et al. Who are the long-QT syndrome patients who receive an implantable cardioverter-defibrillator and what happens to them?: Data from the European Long-QT syndrome implantable cardioverter-defibrillator (LQTS ICD) registry. Circulation 2010, 122, 1272–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Werf, C.; Zwinderman, A.H.; Wilde, A.A.M. Therapeutic approach for patients with catecholaminergic polymorphic ventricular tachycardia: State of the art and future developments. Europace 2012, 14, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Gauvin, C.A.; Klyachman, L.; Grewal, P.K.; Germana, S.S.; Singh, A.; Rashba, E.J. Electrical storm in a case of bilateral pheochromocytomas. Am. J. Case Rep. 2021, 22, e929507. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.; Bonelli, P.; Flori, M.; Cipolletta, L.; Carbucicchio, C.; Izquierdo, M.; Kozluk, E.; Shivkumar, K.; Vaseghi, M.; Patani, F.; et al. Temporal trends and temperature-related incidence of electrical storm: The TEMPEST Study (Temperature-related incidence of electrical storm). Circ. Arrhythmia Electrophysiol. 2017, 10, e004634. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.; Dyson, K.; Bernard, S.; Smith, K. Seasonal Variation in Out-of-Hospital Cardiac Arrest in Victoria 2008–2017: Winter Peak. Prehospital Emerg. Care 2020, 24, 769–777. [Google Scholar] [CrossRef]
- Steinberg, C.; Davies, B.; Mellor, G.; Tadros, R.; Laksman, Z.W.; Roberts, J.D.; Green, M.; Alqarawi, W.; Angaran, P.; Healey, J.; et al. Short-coupled ventricular fibrillation represents a distinct phenotype among latent causes of unexplained cardiac arrest: A report from the CASPER registry. Eur. Heart J. 2021, 42, 2827–2838. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, Y.; Chinushi, M.; Hasegawa, K.; Naiki, N.; Horie, M.; Kaneko, Y.; Kurabayashi, M.; Ito, S.; Imaizumi, T.; Aizawa, Y.; et al. Electrical storm in idiopathic ventricular fibrillation is associated with early repolarization. J. Am. Coll. Cardiol. 2013, 62, 1015–1019. [Google Scholar] [CrossRef] [Green Version]
- Bun, S.S.; Maury, P.; Giustetto, C.; Deharo, J.C. Electrical storm in short-QT syndrome successfully treated with isoproterenol. J. Cardiovasc. Electrophysiol. 2012, 23, 1028–1030. [Google Scholar] [CrossRef]
- Ahmed, W.; Flynn, M.A.; Alpert, M.A. Cardiovascular complications of weight reduction diets. Am. J. Med. Sci. 2001, 321, 280–284. [Google Scholar] [CrossRef]
- Belhassen, B.; Glick, A.; Viskin, S. Efficacy of Quinidine in High-Risk Patients with Brugada Syndrome. Circulation 2004, 110, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antzelevitch, C.; Yan, G.X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J-Wave Syndromes Expert Consensus Conference Report: Emerging Concepts and Gaps in Knowledge. Eur. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2017, 19, 665–694. [Google Scholar] [CrossRef]
- Guarracini, F.; Casella, M.; Muser, D.; Barbato, G.; Notarstefano, P.; Sgarito, G.; Marini, M.; Grandinetti, G.; Mariani, M.V.; Boriani, G.; et al. Clinical Management of Electrical Storm: A Current Overview. J. Cardiovasc. Med. 2021, 22, 669–679. [Google Scholar] [CrossRef]
- Li, D.L.; Cox, Z.L.; Richardson, T.D.; Kanagasundram, A.N.; Saavedra, P.J.; Shen, S.T.; Montgomery, J.A.; Murray, K.T.; Roden, D.M.; Stevenson, W.G.; et al. Quinidine in the Management of Recurrent Ventricular Arrhythmias: A Reappraisal. JACC Clin. Electrophysiol. 2021, 7, 1254–1263. [Google Scholar] [CrossRef] [PubMed]
- Viskin, S.; Chorin, E.; Viskin, D.; Hochstadt, A.; Halkin, A.; Tovia-Brodie, O.; Lee, J.K.; Asher, E.; Laish-Farkash, A.; Amit, G.; et al. Quinidine-Responsive Polymorphic Ventricular Tachycardia in Patients with Coronary Heart Disease. Circulation 2019, 139, 2304–2314. [Google Scholar] [CrossRef]
- Nasir, N., Jr.; Taylor, A.; Doyle, T.K.; Pacifico, A. Evaluation of Intravenous Lidocaine for the Termination of Sustained Monomorphic Ventricular Tachycardia in Patients with Coronary Artery Disease with or without Healed Myocardial Infarction. Am. J. Cardiol. 1994, 74, 1183–1186. [Google Scholar] [CrossRef]
- Gao, D.; Van Herendael, H.; Alshengeiti, L.; Dorian, P.; Mangat, I.; Korley, V.; Ahmad, K.; Golovchiner, G.; Aves, T.; Pinter, A. Mexiletine as an Adjunctive Therapy to Amiodarone Reduces the Frequency of Ventricular Tachyarrhythmia Events in Patients With an Implantable Defibrillator. J. Cardiovasc. Pharmacol. 2013, 62, 199–204. [Google Scholar] [CrossRef]
- Sobiech, M.; Lewandowski, M.; Zając, D.; Maciąg, A.; Syska, P.; Ateńska-Pawłowska, J.; Kowalik, I.; Sterliński, M.; Szwed, H.; Pytkowski, M. Efficacy and Tolerability of Mexiletine Treatment in Patients with Recurrent Ventricular Tachyarrhythmias and Implantable Cardioverter-Defibrillator Shocks. Kardiol. Pol. 2017, 75, 1027–1032. [Google Scholar] [CrossRef]
- Li, G.; Zhang, L. The Role of Mexiletine in the Management of Long QT Syndrome. J. Electrocardiol. 2018, 51, 1061–1065. [Google Scholar] [CrossRef]
- Callans, D.J.; Marchlinski, F.E. Dissociation of Termination and Prevention of Inducibility of Sustained Ventricular Tachycardia with Infusion of Procainamide: Evidence for Distinct Mechanisms. J. Am. Coll. Cardiol. 1992, 19, 111–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorgels, A.P.; van den Dool, A.; Hofs, A.; Mulleneers, R.; Smeets, J.L.; Vos, M.A.; Wellens, H.J. Comparison of Procainamide and Lidocaine in Terminating Sustained Monomorphic Ventricular Tachycardia. Am. J. Cardiol. 1996, 78, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.; Martín, A.; Arribas, F.; Coll-Vinent, B.; Del Arco, C.; Peinado, R.; Almendral, J.; PROCAMIO Study Investigators. Randomized Comparison of Intravenous Procainamide vs. Intravenous Amiodarone for the Acute Treatment of Tolerated Wide QRS Tachycardia: The PROCAMIO Study. Eur. Heart J. 2017, 38, 1329–1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Peng, X.; Lin, R.; Wang, X.; Liu, X.; Bai, R.; Ma, C.; Tang, R.; Ruan, Y.; Liu, N. The Antiarrhythmic Mechanisms of Flecainide in Catecholaminergic Polymorphic Ventricular Tachycardia. Front. Physiol. 2022, 13, 419. [Google Scholar] [CrossRef] [PubMed]
- Vaseghi, M.; Shivkumar, K. The Role of the Autonomic Nervous System in Sudden Cardiac Death. Prog. Cardiovasc. Dis. 2008, 50, 404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowe, M.D.; Rowland, E.; Brown, M.J. Grace AABeta(2) Adrenergic Receptors Mediate Important Electrophysiological Effects in Human Ventricular Myocardium. Heart (Br. Card. Soc.) 2001, 86, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Tsagalou, E.P.; Kanakakis, J.; Rokas, S.; Anastasiou-Nana, M.I. Suppression by Propranolol and Amiodarone of an Electrical Storm Refractory to Metoprolol and Amiodarone. Int. J. Cardiol. 2005, 99, 341–342. [Google Scholar] [CrossRef]
- Chatzidou, S.; Kontogiannis, C.; Tsilimigras, D.I.; Georgiopoulos, G.; Kosmopoulos, M.; Papadopoulou, E.; Vasilopoulos, G.; Rokas, S. Propranolol Versus Metoprolol for Treatment of Electrical Storm in Patients with Implantable Cardioverter-Defibrillator. J. Am. Coll. Cardiol. 2018, 71, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Li, L.I.; Zhou, Y.L.; Zhang, X.J.; Wang, H.T. Successful Treatment of Cardiac Electrical Storm in Dilated Cardiomyopathy Using Esmolol: A Case Report. Exp. Ther. Med. 2016, 12, 107–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, Y.Y. Landiolol: A Review in Tachyarrhythmias. Drugs 2018, 78, 377–388. [Google Scholar] [CrossRef]
- Shiga, T.; Ikeda, T.; Shimizu, W.; Kinugawa, K.; Sakamoto, A.; Nagai, R.; Daimon, T.; Oki, K.; Okamoto, H.; Yamashita, T. Efficacy and Safety of Landiolol in Patients with Ventricular Tachyarrhythmias with or Without Renal Impairment- Subanalysis of the J-Land II Study. Circ. Rep. 2020, 2, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Kaski, J.C.; Girotti, L.A.; Messuti, H.; Rutitzky, B.; Rosenbaum, M.B. Long-Term Management of Sustained, Recurrent, Symptomatic Ventricular Tachycardia with Amiodarone. Circulation 1981, 64, 273–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowey, P.R.; Levine, J.H.; Herre, J.M.; Pacifico, A.; Lindsay, B.D.; Plumb, V.J.; Janosik, D.L.; Kopelman, H.A.; Scheinman, M.M. Randomized, Double-Blind Comparison of Intravenous Amiodarone and Bretylium in the Treatment of Patients with Recurrent, Hemodynamically Destabilizing Ventricular Tachycardia or Fibrillation. Circulation 1995, 92, 3255–3263. [Google Scholar] [CrossRef]
- Jung, W.; Manz, M.; Pizzulli, L.; Pfeiffer, D.; Lüderitz, B. Effects of Chronic Amiodarone Therapy on Defibrillation Threshold. Am. J. Cardiol. 1992, 70, 1023–1027. [Google Scholar] [CrossRef] [PubMed]
- Vrobel, T.R.; Miller, P.E.; Mostow, N.D.; Rakita, L. A General Overview of Amiodarone Toxicity: Its Prevention, Detection, and Management. Prog. Cardiovasc. Dis. 1989, 31, 393–426. [Google Scholar] [CrossRef] [PubMed]
- Furushima, H.; Chinushi, M.; Okamura, K.; Komura, S.; Tanabe, Y.; Sato, A.; Izumi, D.; Aizawa, Y. Effect of Dl-Sotalol on Mortality and Recurrence of Ventricular, Tachyarrhythmias:Ischemic Compared to Nonischemic Cardiomyopathy. Pacing Clin. Electrophysiol. 2007, 30, 1136–1141. [Google Scholar] [CrossRef]
- Pacifico, A.; Hohnloser, S.H.; Williams, J.H.; Tao, B.; Saksena, S.; Henry, P.D.; Prystowsky, E.N. Prevention of Implantable-Defibrillator Shocks by Treatment with Sotalol. d,l-Sotalol Implantable Cardioverter-Defibrillator Study Group. N. Engl. J. Med. 1999, 340, 1855–1862. [Google Scholar] [CrossRef]
- Verduyn, S.C.; Vos, M.A.; van der Zande, J.; van der Hulst, F.F.; Wellens, H.J. Role of Interventricular Dispersion of Repolarization in Acquired Torsade-de-Pointes Arrhythmias: Reversal by Magnesium. Cardiovasc. Res. 1997, 34, 453–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.; Dorian, P.; Roberts, R.; Gent, M.; Bailin, S.; Fain, E.; Thorpe, K.; Champagne, J.; Talajic, M.; Coutu, B.; et al. Optimal Pharmacological Therapy in Cardioverter Defibrillator Patients (OPTIC) Investigators. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: The OPTIC study: A randomized trial. JAMA 2006, 295, 165–171. [Google Scholar]
- Kataoka, N.; Nagase, S.; Okawa, K.; Aiba, T.; Kinugawa, K.; Kusano, K. Multifocal Purkinje-related premature contractions and electrical storm suppressed by quinidine and verapamil in a case with short-coupled ventricular fibrillation. J. Cardiol. Cases 2021, 25, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Vega, J.; Enríquez, A.; Vergara, I.; Frangini, P.; Baeza, M.; Millapán, I.; González, R. Electrical storm in Brugada syndrome successfully treated with isoproterenol. Report of a case. Rev. Med. De Chile 2013, 141, 1340–1343. [Google Scholar] [CrossRef] [Green Version]
- Chinushi, M.; Hasegawa, K.; Iijima, K.; Furushima, H.; Izumi, D.; Sato, A.; Aizawa, Y. Characteristics of J Wave-Associated Idiopathic Ventricular Fibrillation: Role of Drugs. Pacing Clin. Electrophysiol. 2012, 35, e226–e230. [Google Scholar] [CrossRef] [PubMed]
- Bernard, A.; Genée, O.; Grimard, C.; Sacher, F.; Fauchier, L.; Babuty, D. Electrical storm reversible by isoproterenol infusion in a striking case of early repolarization. J. Interv. Card. Electrophysiol. 2009, 25, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Tzivoni, D.; Banai, S.; Schuger, C.; Benhorin, J.; Keren, A.; Gottlieb, S.; Stern, S. Treatment of torsade de pointes with magnesium sulfate. Circulation 1988, 77, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lüderitz, B.; Manz, M. The value of magnesium in intensive care medicine. Z. Fur Kardiol. 1994, 83 (Suppl. S6), 121–126. [Google Scholar]
- Manz, M.; Jung, W.; Lüderitz, B. Effect of magnesium on sustained ventricular tachycardia. Herz 1997, 22 (Suppl. S1), 51–55. [Google Scholar] [CrossRef] [PubMed]
- Vergara, P.; Tung, R.; Vaseghi, M.; Brombin, C.; Frankel, D.S.; Di Biase, L.; Nagashima, K.; Tedrow, U.; Tzou, W.S.; Sauer, W.H. Successful Ventricular Tachycardia Ablation in Patients with Electrical Storm Reduces Recurrences and Improves Survival. Heart Rhythm. 2018, 15, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Muser, D.; Liang, J.J.; Pathak, R.K.; Magnani, S.; Castro, S.A.; Hayashi, T.; Garcia, F.C.; Supple, G.E.; Riley, M.P.; Lin, D.; et al. Long-Term Outcomes of Catheter Ablation of Electrical Storm in Nonischemic Dilated Cardiomyopathy Compared with Ischemic Cardiomyopathy. JACC. Clin. Electrophysiol. 2017, 3, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Schaeffer, B.; Tanigawa, S.; Muthalaly, R.G.; John, R.M.; Michaud, G.F.; Tedrow, U.B. Stevenson WGCatheter Ablation of Polymorphic Ventricular Tachycardia/Fibrillation in Patients with and without Structural Heart Disease. Heart Rhythm. 2019, 16, 1021–1027. [Google Scholar] [CrossRef]
- Romero, J.; Stevenson, W.G.; Fujii, A.; Kapur, S.; Baldinger, S.H.; Mehta, N.K.; John, R.M.; Michaud, G.F.; Epstein, L.M.; Koplan, B.A.; et al. Impact of Number of Oral Antiarrhythmic Drug Failures Before Referral on Outcomes Following Catheter Ablation of Ventricular Tachycardia. JACC. Clin. Electrophysiol. 2018, 4, 810–819. [Google Scholar] [CrossRef]
- Frankel, D.S.; Mountantonakis, S.E.; Robinson, M.R.; Zado, E.S.; Callans, D.J.; Marchlinski, F.E. Ventricular Tachycardia Ablation Remains Treatment of Last Resort in Structural Heart Disease: Argument for Earlier Intervention. J. Cardiovasc. Electrophysiol. 2011, 22, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Della Bella, P.; Baratto, F.; Vergara, P.; Bertocchi, P.; Santamaria, M.; Notarstefano, P.; Calò, L.; Orsida, D.; Tomasi, L.; Piacenti, M.; et al. Does Timing of Ventricular Tachycardia Ablation Affect Prognosis in Patients with an Implantable Cardioverter Defibrillator? Results From the Multicenter Randomized PARTITA Trial. Circulation 2022, 145, 1829–1838. [Google Scholar] [CrossRef] [PubMed]
- Doytchinova, A.; Hassel, J.L.; Yuan, Y.; Lin, H.; Yin, D.; Adams, D.; Straka, S.; Wright, K.; Smith, K.; Wagner, D.; et al. Simultaneous Noninvasive Recording of Skin Sympathetic Nerve Activity and Electrocardiogram. Heart Rhythm. 2017, 14, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Shannon, K.; Saltzman, D.; Li, I.; Mokszycki, R.; Galletta, G. Ventricular Tachycardia Converts to Sinus Rhythm after Administration of Propofol. Am. J. Emerg. Med. 2021, 48, 377.e1–377.e3. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, J.S.; Jacobsen, P.K.; Grand, J.; Lindholm, M.G.; Hassager, C.; Pehrson, S.; Kjaergaard, J.; Bundgaard, H. Deep Sedation as Temporary Bridge to Definitive Treatment of Ventricular Arrhythmia Storm. Eur. Heart Journal. Acute Cardiovasc. Care 2020, 9, 657–664. [Google Scholar] [CrossRef]
- Martins, R.P.; Urien, J.M.; Barbarot, N.; Rieul, G.; Sellal, J.M.; Borella, L.; Clementy, N.; Bisson, A.; Guenancia, C.; Sagnard, A. Effectiveness of Deep Sedation for Patients with Intractable Electrical Storm Refractory to Antiarrhythmic Drugs. Circulation 2020, 142, 1599–1601. [Google Scholar] [CrossRef]
- Bourke, T.; Vaseghi, M.; Michowitz, Y.; Sankhla, V.; Shah, M.; Swapna, N.; Boyle, N.G.; Mahajan, A.; Narasimhan, C.; Lokhandwala, Y.; et al. Neuraxial Modulation for Refractory Ventricular Arrhythmias: Value of Thoracic Epidural Anesthesia and Surgical Left Cardiac Sympathetic Denervation. Circulation 2010, 121, 2255–2262. [Google Scholar] [CrossRef] [Green Version]
- Do, D.H.; Bradfield, J.; Ajijola, O.A.; Vaseghi, M.; Le, J.; Rahman, S.; Mahajan, A.; Nogami, A.; Boyle, N.G.; Shivkumar, K. Thoracic Epidural Anesthesia Can Be Effective for the Short-Term Management of Ventricular Tachycardia Storm. J. Am. Heart Assoc. Cardiovasc. Cerebrovasc. Dis. 2017, 6, e007080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fudim, M.; Qadri, Y.J.; Waldron, N.H.; Boortz-Marx, R.L.; Ganesh, A.; Patel, C.B.; Podgoreanu, M.V.; Sun, A.Y.; Milano, C.A.; Tong, B.C.; et al. Stellate Ganglion Blockade for the Treatment of Refractory Ventricular Arrhythmias. JACC. Clin. Electrophysiol. 2020, 6, 562–571. [Google Scholar] [CrossRef]
- Reinertsen, E.; Sabayon, M.; Riso, M.; Lloyd, M.; Spektor, B. Stellate Ganglion Blockade for Treating Refractory Electrical Storm: A Historical Cohort Study. Can. J. Anaesth. = J. Can. D’anesthesie 2021, 68, 1683–1689. [Google Scholar] [CrossRef]
- Vaseghi, M.; Barwad, P.; Malavassi Corrales, F.J.; Tandri, H.; Mathuria, N.; Shah, R.; Sorg, J.M.; Gima, J.; Mandal, K.; Sàenz Morales, L.C.; et al. Cardiac Sympathetic Denervation for Refractory Ventricular Arrhythmias. J. Am. Coll. Cardiol. 2017, 69, 3070–3080. [Google Scholar] [CrossRef]
- Prado, G.M.; Mahfoud, F.; Lopes, R.D.; Moreira, D.A.R.; Staico, R.; Damiani, L.P.; Ukena, C.; Armaganijan, L.V. Renal Denervation for the Treatment of Ventricular Arrhythmias: A Systematic Review and Meta-Analysis. J. Cardiovasc. Electrophysiol. 2021, 32, 1430–1439. [Google Scholar] [CrossRef] [PubMed]
- Ukena, C.; Mahfoud, F.; Ewen, S.; Bollmann, A.; Hindricks, G.; Hoffmann, B.A.; Linz, D.; Musat, D.; Pavlicek, V.; Scholz, E.; et al. Renal Denervation for Treatment of Ventricular Arrhythmias: Data from an International Multicenter Registry. Clin. Res. Cardiol. 2016, 105, 873–879. [Google Scholar] [CrossRef]
- Tsai, F.C.; Wang, Y.C.; Huang, Y.K.; Tseng, C.N.; Wu, M.Y.; Chang, Y.S.; Chu, J.J.; Lin, P.J. Extracorporeal Life Support to Terminate Refractory Ventricular Tachycardia. Crit. Care Med. 2007, 35, 1673–1676. [Google Scholar] [CrossRef] [PubMed]
- Palaniswamy, C.; Miller, M.A.; Reddy, V.Y.; Dukkipati, S.R. Hemodynamic Support for Ventricular Tachycardia Ablation. Cardiac Electrophysiology Clinics 2017, 9, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Dyer, S.; Mogni, B.; Gottlieb, M. Electrical Storm: A Focused Review for the Emergency Physician. Am. J. Emerg. Med. 2020, 38, 1481–1487. [Google Scholar] [CrossRef]
- Ninni, S.; Gallot-Lavallée, T.; Klein, C.; Longère, B.; Brigadeau, F.; Potelle, C.; Crop, F.; Rault, E.; Decoene, C.; Lacornerie, T.; et al. Stereotactic Radioablation for Ventricular Tachycardia in the Setting of Electrical Storm. Circ. Arrhythmia Electrophysiol. 2022, 15, e010955. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| TRIGGERS | PREDICTORS OF ONE-YEAR MORTALITY |
|---|---|
|
|
| Drug | Oral Dose | IV Dose | Timing a | Contraindication |
|---|---|---|---|---|
| Quinidine | 60–1600 mg Loading dose: start 200 mg every 3 h until effect (max 3 gr in first 24 h) | NO | Onset: 1–3 h Peak: 1 h Half-life: 6–8 gg | Thrombocytopenia |
| Mexiletine | 600–1200 mg Loading dose: 400 mg initially followed by 600 mg in the first 24 h | NO | Onset: 30 min–2 h Peak: 1–4 h Half-life: 10 h | Cardiogenic shock |
| Lidocaine | NO | Bolus: 50–200 mg Infusion: 2–4 mg/min | Onset: 45–90 s Peak: 1–2 min Half-life: 1–2 h | Low potassium |
| Procainamide | NO | Bolus: 100 mg, can be repeated after 5 min if no effect (max 500–750 mg/50 mg/min) Infusion: 2–6 mg/min | Onset: 10–30 min Peak: 1 h Half-life: 2.5–5 h | Marrow failure or cytopenia |
| Flecainide | 200–400 mg | 1–2 mg/kg over 10 min | Onset: 1–5 min Peak: 2–3 h Half-life: 7–22 h | High potassium or low potassium |
| Propafenone | 450–900 mg | Bolus: 0.5–2 mg/kg in 15–20 min), can be repeated after 60–90 min Infusion: 0.007 mg/kg/min (max 12 h) | Onset: 2 h Peak: 2–4 h Half-life: 6 h | AMI in the last 3 months and LVEF < 35% |
| Metoprolol | 25 mg twice a day up to 200 mg/day | Bolus: 2–5 mg every 5 min up to 3 doses in 15 min | Onset: some mins Peak: 20 min Half-life:3–7 h | Severe asthma |
| Propanolol | 80–320 mg/day | 160 mg/24 h | Onset: 30 min Peak: 60–90 min Half-life: 4–5 gg | Severe asthma |
| Landiolol | NO | Bolus: 100 mcg/kg in 1 min Infusion: 10–40 mcg/kg/min (max 80 mcg/kg/min) max per 24 h (max 57.6 mg/kg/day) | Onset: 30 s Peak: 5 min Half-life: 4 min | Severe asthma |
| Esmolol | NO | Bolus: 300–500 mcg/kg in 1 min Infusion: 25–50 mg/kg/min (max 250 mg/kg/min (uptitration 5–10 min) | Onset: 60 s Peak: 5 min Half-life: 9 min | Severe asthma |
| Amiodarone | 200–400 mg Loading dose: 600–1200 mg/24 h per 8–10 days | Loading dose: 5 mL/kg in 20 min–2 h Infusion: 600–1200 mg/24 h per 8–10 days | Onset: 10 min Peak: 15 min Half-life: 50 gg | Dysthyroidism |
| Sotalol | 160–640 mg | 0.5–1.5 mg/kg in 10 min. If necessary, it can be repeated after 6 h | Onset: 60 min Peak: 2–4 h Half-life: 10–20 h | Severe asthma |
| Verapamil | 120–480 mg | Bolus: 5–10 mg, slow; if necessary, it can be repeated in 30 min | Onset: 1–2 min Peak: 5–15 min Half-life: 3–8 h | QRS complex tachycardia of unknown mechanism |
| Isoproterenol | NO | 0.5–10 mcg/min | Onset: 1 min Peak:15–30 min Half-life: 2.5–5 min | Acute coronary syndromes |
| Magnesium sulfate | NO | Bolus: 2 gr in 5 min, can be repeated (max 4–6 g over 20 min) Infusion: 2–4 gr/h for 12–24 h | Onset: immediately Peak: in 30 min Half-life 5 h | Several renal failure, pulmonary edema |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarracini, F.; Bonvicini, E.; Zanon, S.; Martin, M.; Casagranda, G.; Mochen, M.; Coser, A.; Quintarelli, S.; Branzoli, S.; Mazzone, P.; et al. Emergency Management of Electrical Storm: A Practical Overview. Medicina 2023, 59, 405. https://doi.org/10.3390/medicina59020405
Guarracini F, Bonvicini E, Zanon S, Martin M, Casagranda G, Mochen M, Coser A, Quintarelli S, Branzoli S, Mazzone P, et al. Emergency Management of Electrical Storm: A Practical Overview. Medicina. 2023; 59(2):405. https://doi.org/10.3390/medicina59020405
Chicago/Turabian StyleGuarracini, Fabrizio, Eleonora Bonvicini, Sofia Zanon, Marta Martin, Giulia Casagranda, Marianna Mochen, Alessio Coser, Silvia Quintarelli, Stefano Branzoli, Patrizio Mazzone, and et al. 2023. "Emergency Management of Electrical Storm: A Practical Overview" Medicina 59, no. 2: 405. https://doi.org/10.3390/medicina59020405