
Placental Growth Factor and Pregnancy-Associated Plasma Protein-A as Potential Early Predictors of Gestational Diabetes Mellitus


Abstract
:1. Introduction
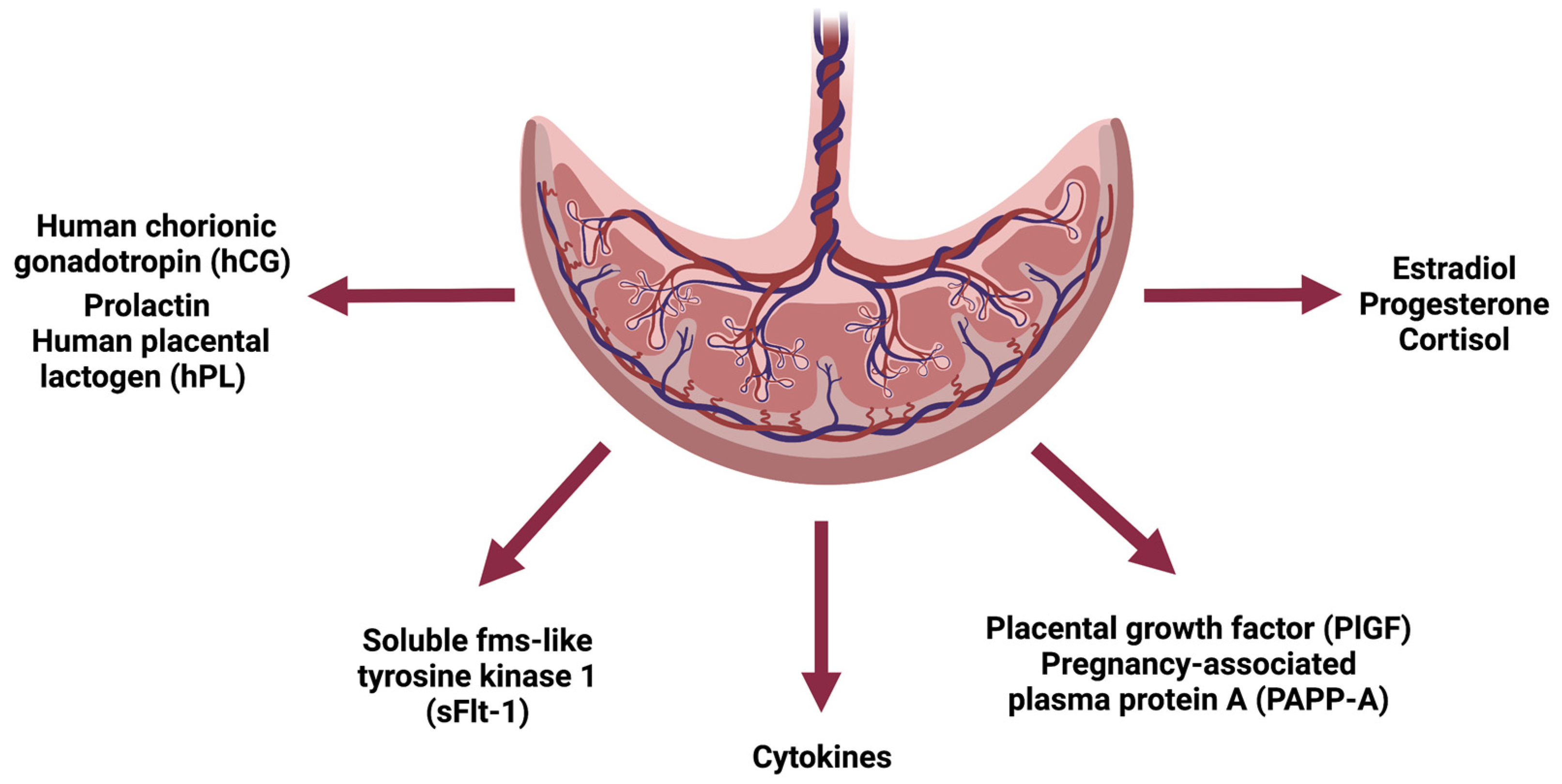
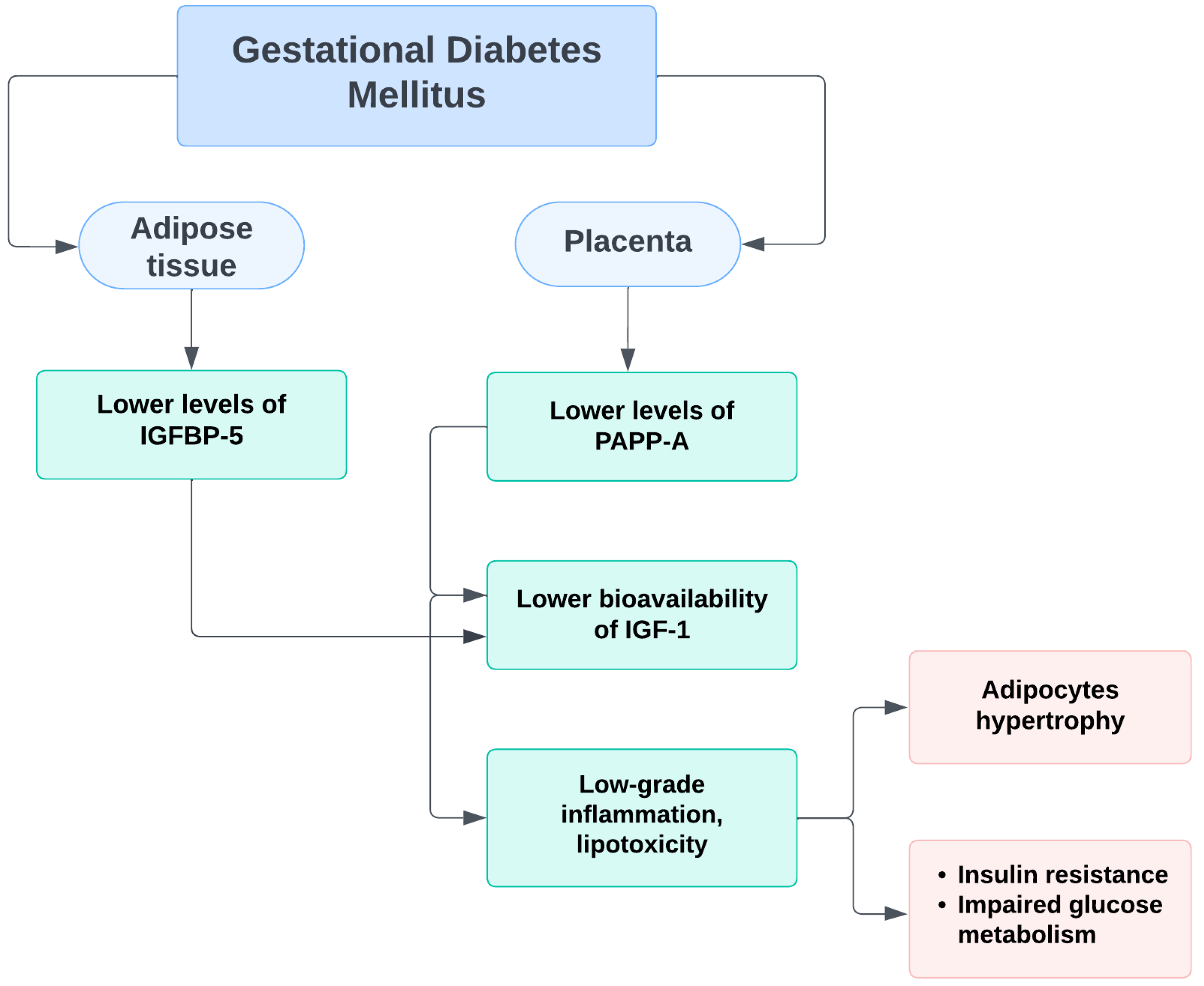
2. Pathogenesis of GDM
3. PAPP-A
4. PlGF
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes. Diabetes Care 2022, 45 (Suppl. S1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Modzelewski, R.; Stefanowicz-Rutkowska, M.M.; Matuszewski, W.; Bandurska-Stankiewicz, E.M. Gestational Diabetes Mellitus-Recent Literature Review. J. Clin. Med. 2022, 11, 5736. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care. Int. J. Gynaecol. Obstet. 2015, 131 (Suppl. S3), S173–S211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farahvar, S.; Walfisch, A.; Sheiner, E. Gestational diabetes risk factors and long-term consequences for both mother and offspring: A literature review. Expert Rev. Endocrinol. Metab. 2019, 14, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Davey, R.X.; Hamblin, P.S. Selective versus universal screening for gestational diabetes mellitus: An evaluation of predictive risk factors. Med. J. Aust. 2001, 174, 118–121. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Farrar, D.; Fairley, L.; Wright, J.; Tuffnell, D.; Whitelaw, D.; Lawlor, D.A. Evaluation of the impact of universal testing for gestational diabetes mellitus on maternal and neonatal health outcomes: A retrospective analysis. BMC Pregnancy Childbirth 2014, 14, 317. [Google Scholar] [CrossRef] [Green Version]
- Cosson, E.; Benbara, A.; Pharisien, I.; Nguyen, M.T.; Revaux, A.; Lormeau, B.; Sandre-Banon, D.; Assad, N.; Pillegand, C.; Valensi, P.; et al. Diagnostic and prognostic performances over 9 years of a selective screening strategy for gestational diabetes mellitus in a cohort of 18,775 subjects. Diabetes Care 2013, 36, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Miailhe, G.; Kayem, G.; Girard, G.; Legardeur, H.; Mandelbrot, L. Selective rather than universal screening for gestational diabetes mellitus? Eur. J. Obstet. Gynecol. Reprod. Boil. 2015, 191, 95–100. [Google Scholar] [CrossRef]
- Benhalima, K.; Mathieu, C.; Van Assche, A.; Damm, P.; Devlieger, R.; Mahmood, T.; Dunne, F. Survey by the European Board and College of Obstetrics and Gynaecology on Screening for Gestational Diabetes in Europe. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 201, 197–202. [Google Scholar] [CrossRef]
- Agha-Raffar, R.; Oliver, N.; Jhonston, D.; Robinson, S. Gestational diabetes mellitus: Does an effective prevention strategy exist? Nat. Rev. Endocrinol. 2016, 12, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Kampmann, U.; Knorr, S.; Fuglsang, J.; Ovesen, P. Determinants of Maternal Insulin Resistance during Pregnancy: An Updated Overview. J. Diabetes Res. 2019, 2019, 5320156. [Google Scholar] [CrossRef] [Green Version]
- Sonagra, A.D.; Biradar, S.M.; Dattatreya, K.; Jayaprakash Murthy, D.S. Normal Pregnancy—A State of Insulin Resistance. J. Clin. Diagn. Res. 2014, 8, CC01–CC03. [Google Scholar] [CrossRef]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19–39. [Google Scholar]
- Zavalza-Gómez, A.B.; Anaya-Prado, R.; Rincón-Sánchez, A.R.; Mora-Martínez, J.M. Adipokines and insulin resistance during pregnancy. Diabetes Res. Clin. Pract. 2008, 80, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F. Carbohydrate and lipid metabolism in pregnancy: Normal compared with gestational diabetes mellitus. Am. J. Clin. Nutr. 2000, 71, 1256S–1261S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trivett, C.; Lees, Z.J.; Freeman, D.J. Adipose tissue function in healthy pregnancy, gestational diabetes mellitus and pre-eclampsia. Eur. J. Clin. Nutr. 2021, 75, 1745–1756. [Google Scholar] [CrossRef]
- Moyce, B.L.; Dolinsky, V.W. Maternal β-Cell Adaptations in Pregnancy and Placental Signalling: Implications for Gestational Diabetes. Int. J. Mol. Sci. 2018, 19, 3467. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.A. The endocrine function of human placenta: An overview. Reprod. Biomed. Online 2016, 32, 14–43. [Google Scholar] [CrossRef] [Green Version]
- Webber, J.; Charlton, M.; Johns, N. Diabetes in pregnancy: Management of diabetes and its complications from preconception to the postnatal period (NG3). Br. J. Diabetes 2015, 15, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Rani, P.R.; Begum, J. Screening and Diagnosis of Gestational Diabetes Mellitus, Where Do We Stand. J. Clin. Diagn. Res. 2016, 10, QE01–QE04. [Google Scholar] [CrossRef]
- Kagan, K.O.; Sonek, J.; Wagner, P.; Hoopmann, M. Principles of first trimester screening in the age of non-invasive prenatal diagnosis: Screening for chromosomal abnormalities. Arch. Gynecol. Obstet. 2017, 296, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Saruhan, Z.; Ozekinci, M.; Simsek, M.; Mendilcioglu, I. Association of first trimester low PAPP-A levels with adverse pregnancy outcomes. Clin. Exp. Obstet. Gynecol. 2012, 39, 225–228. [Google Scholar] [PubMed]
- Pandya, P.; Wright, D.; Syngelaki, A.; Akolekar, R.; Nicolaides, K.H. Maternal serum placental growth factor in prospective screening for aneuploidies at 8-13 weeks’ gestation. Fetal Diagn Ther. 2012, 31, 87–93. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, N.; Wright, D.; Syngelaki, A.; Akolekar, R.; Wright, A.; Poon, L.C.; Nicolaides, K.H. Competing risks model in screening for preeclampsia by maternal factors and biomarkers at 11–13 weeks gestation. Am. J. Obstet. Gynecol. 2016, 214, 103.e1–103.e12. [Google Scholar] [CrossRef] [Green Version]
- Meloni, P.; D’Angeli, I.; Piazze, J.; Cerekya, A.; Simari, T.; Pala, A.; Anceschi, M.M.; Guglietta, M.; Izzo, P.; Izzo, L. First Trimester PAPP-A Levels Associated with Early Prediction of Pregnancy Induced Hypertension. Hypertens. Pregnancy 2009, 28, 361–368. [Google Scholar] [CrossRef]
- Petry, C.J.; Ong, K.K.; Hughes, I.A.; Acerini, C.L.; Frystyk, J.; Dunger, D.B. Early Pregnancy-Associated Plasma Protein A Concentrations Are Associated with Third Trimester Insulin Sensitivity. J. Clin. Endocrinol. Metab. 2017, 102, 2000–2008. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rodriguez, R.; Ziegler, R.; DeSouza, T.; Majid, S.; Madore, A.S.; Amir, N.; Pace, V.A.; Nachreiner, D.; Alfego, D.; Mathew, J.; et al. PAPPA-mediated adipose tissue remodeling mitigates insulin resistance and protects against gestational diabetes in mice and humans. Sci. Transl. Med. 2020, 12, eaay4145. [Google Scholar] [CrossRef]
- Talasaz, Z.H.; Sadeghi, R.; Askari, F.; Dadgar, S.; Vatanchi, A. First trimesters Pregnancy-Associated Plasma Protein-A levels value to Predict Gestational diabetes Mellitus: A systematic review and meta-analysis of the literature. Taiwan J. Obstet. Gynecol. 2018, 57, 181–189. [Google Scholar] [CrossRef]
- Donovan, B.M.; Nidey, N.L.; Jasper, E.A.; Robinson, J.G.; Bao, W.; Saftlas, A.F.; Ryckman, K.K. First trimester prenatal screening biomarkers and gestational diabetes mellitus, A systematic review and meta-analysis. PLoS ONE 2018, 13, e0201319. [Google Scholar] [CrossRef]
- Lin, T.M.; Halbert, S.P.; Spellacy, W.N. Measurement of pregnancy-associated plasma proteins during human gestation. J. Clin. Investig. 1974, 54, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Conover, C.A. Key Questions and Answers about Pregnancy-Associated Plasma Protein-A. Trends Endocrinol. Metab. 2012, 23, 242–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, J.B.; Oxvig, C.; Overgaard, M.T.; Sottrup-Jensen, L.; Gleich, G.J.; Hays, L.G.; Yates, J.R., 3rd; Conover, C.A. The insulin-like growth factor (IGF)-dependent IGF binding protein-4 protease secreted by human fibroblasts is pregnancy-associated plasma protein-A. Proc. Natl. Acad. Sci. USA 1999, 96, 3149–3153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, M.; Panchanadikar, T.M.; Wagh, G. Variation of PAPP-A level in the first trimester of pregnancy and its clinical outcome. J. Obstet. Gynaecol. India 2014, 64, 116–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sferruzzi-Perri, A.N.; Sandovici, I.; Constancia, M.; Fowden, A.L. Placental Phenotype and the Insulin-like Growth Factors: Resource Allocation to Fetal Growth. J. Physiol. 2017, 595, 5057–5093. [Google Scholar] [CrossRef] [Green Version]
- Clemmons, D.R. Metabolic actions of insulin-like growth factor-I in normal physiology and diabetes. Endocrinol. Metab. Clin. N. Am. 2012, 41, 425–443. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rodriguez, R.; Lifshitz, L.M.; Bellve, K.D.; Min, S.Y.; Pires, J.; Leung, K.; Boeras, C.; Sert, A.; Draper, J.T.; Corvera, S.; et al. Human adipose tissue expansion in pregnancy is impaired in gestational diabetes mellitus. Diabetologia 2015, 58, 2106–2114. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.Y.; Liao, A.W.; Spencer, K.; Munim, S.; Nicolaides, K.H. First trimester maternal serum free beta human chorionic gonadotrophin and pregnancy associated plasma protein A as predictors of pregnancy complications. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 1265–1270. [Google Scholar] [CrossRef]
- Beneventi, F.; Simonetta, M.; Lovati, E.; Albonico, G.; Tinelli, C.; Locatelli, E.; Spinillo, A. First trimester pregnancy-associated plasma protein-A in pregnancies complicated by subsequent gestational diabetes. Prenat. Diagn. 2011, 31, 523–528. [Google Scholar] [CrossRef]
- Lovati, E.; Beneventi, F.; Simonetta, M.; Laneri, M.; Quarleri, L.; Scudeller, L.; Albonico, G.; Locatelli, E.; Cavagnoli, C.; Tinelli, C.; et al. Gestational diabetes mellitus: Including serum pregnancy-associated plasma protein-A testing in the clinical management of primiparous women? A case–control study. Diabetes Res. Clin. Pr. 2013, 100, 340–347. [Google Scholar] [CrossRef]
- Spencer, K.; Cowans, N.J. The association between gestational diabetes mellitus and first trimester aneuploidy screening markers. Ann. Clin. Biochem. 2013, 50, 603–610. [Google Scholar] [CrossRef] [Green Version]
- Kulaksizoglu, S.; Kulaksizoglu, M.; Kebapcilar, A.G.; Torun, A.N.; Ozcimen, E.; Turkoglu, S. Can first-trimester screening program detect women at high risk for gestational diabetes mellitus? Gynecol Endocrinol. 2013, 29, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Beneventi, F.; Simonetta, M.; Locatelli, E.; Cavagnoli, C.; Badulli, C.; Lovati, E.; Garbin, G.; Genini, E.; Albertini, R.; Tinelli, C.; et al. Temporal variation in soluble human leukocyte antigen-G (sHLA-G) and pregnancy-associated plasma protein A (PAPP-A) in pregnancies complicated by gestational diabetes mellitus and in controls. Am. J. Reprod. Immunol. 2014, 72, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Bleicher, K.; Han, X.; McShane, M.; Chan, Y.F.; Bartlett, A.; White, C.; Lau, S.M. Maternal Diabetes, Large for Gestational Age Births and First Trimester Pregnancy Associated Plasma Protein-A. J. Clin. Endocrinol. Metab. 2015, 100, 2372–2379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syngelaki, A.; Kotecha, R.; Pastides, A.; Wright, A.; Nicolaides, K.H. First-trimester biochemical markers of placentation in screening for gestational diabetes mellitus. Metabolism 2015, 64, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Ferraz, T.; Pinto, P.; Martins, S.; Guimarães, J.T.; Montenegro, N.; Ramalho, C. 754: Serum PAPP-A as a predictor of gestational diabetes. Am. J. Obstet. Gynecol. 2015, 212, S366e7. [Google Scholar] [CrossRef]
- Xiao, D.; Chenhong, W.; Yanbin, X.; Lu, Z. Gestational diabetes mellitus and first trimester pregnancy-associated plasma protein A: A case-control study in a Chinese population. J. Diabetes Investig. 2018, 9, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, S.; Ahmadi, M.; Saqhafi, H.; Alipoor, M. Association of Pregnancy-Associated Plasma Protein A (PAPP-A) and Gestational Diabetes. Iran. J. Obstet. Gynecol. Infertil. 2017, 20, 61–69. [Google Scholar]
- Ramezani, S.; Doulabi, M.A.; Saqhafi, H.; Alipoor, M. Prediction of Gestational Diabetes by Measuring the Levels of Pregnancy Associated Plasma Protein-A (PAPP-A) During Gestation Weeks 11-14. J. Reprod. Infertil. 2020, 21, 130–137. [Google Scholar]
- Ren, Z.; Zhe, D.; Li, Z.; Sun, X.-P.; Yang, K.; Lin, L. Study on the correlation and predictive value of serum pregnancy-associated plasma protein A, triglyceride and serum 25-hydroxyvitamin D levels with gestational diabetes mellitus. World J. Clin. Cases 2020, 8, 864–873. [Google Scholar] [CrossRef]
- Caliskan, R.; Atis, A.; Aydin, Y.; Acar, D.; Kiyak, H.; Topbas, F. PAPP-A concentrations change in patients with gestational diabetes. J. Obstet Gynaecol. 2020, 40, 190–194. [Google Scholar] [CrossRef]
- Yanachkova, V.E.; Staynova, R.; Bochev, I.; Kamenov, Z. Potential role of biochemical placentation markers—Pregnancy associated plasma protein-A and human chorionic gonadotropin for early gestational diabetes screening—A pilot study. Ginekol. Pol. 2022, 93, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Kuc, S.; Wortelboer, E.; Koster, M.; de Valk, H.; Schielen, P.; Visser, G. Prediction of macrosomia at birth in type-1 and 2 diabetic pregnancies with biomarkers of early placentation. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 748–754. [Google Scholar] [CrossRef]
- Savvidou, M.D.; Syngelaki, A.; Muhaisen, M.; Emelyanenko, E.; Nicolaides, K.H. First trimester maternal serum free beta-human chorionic gonadotropin and pregnancy-associated plasma protein A in pregnancies complicated by diabetes mellitus. Br. J. Obstet. Gynaecol. 2012, 119, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, Q.K.; Lo, T.K.; Wong, S.F.; Lee, C.P. Association between pregnancy-associated plasma protein-A levels in the first trimester and gestational diabetes mellitus in Chinese women. Hong Kong Med. J. 2016, 22, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Tul, N.; Pusenjak, S.; Osredkar, J.; Spencer, K.; Novak-Antolic, Z. Predicting complications of pregnancy with first-trimester maternal serum free-betahCG, PAPP-A and inhibin-A. Prenat. Diagn. 2003, 23, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Husslein, H.; Lausegger, F.; Leipold, H.; Worda, C. Association between pregnancy-associated plasma protein-A and gestational diabetes requiring insulin treatment at 11–14 weeks of gestation. J. Matern. Fetal Neonatal Med. 2012, 25, 2230–2233. [Google Scholar] [CrossRef]
- Visconti, F.; Quaresima, P.; Chiefari, E.; Caroleo, P.; Arcidiacono, B.; Puccio, L.; Mirabelli, M.; Foti, D.P.; Di Carlo, C.; Vero, R.; et al. First Trimester Combined Test (FTCT) as a Predictor of Gestational Diabetes Mellitus. Int. J. Environ. Res. Public Health 2019, 16, 3654. [Google Scholar] [CrossRef] [Green Version]
- Maglione, D.; Guerriero, V.; Viglietto, G.; Delli-Bovi, P.; Persico, M.G. Isolation of a human placenta cDNA coding for a protein related to the vascular permeability factor. Proc. Natl. Acad. Sci. USA 1991, 88, 9267–9271. [Google Scholar] [CrossRef] [Green Version]
- De Falco, S. The discovery of placenta growth factor and its biological activity. Exp. Mol. Med. 2012, 44, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Depoix, C.; Tee, M.K.; Taylor, R.N. Molecular regulation of human placental growth factor (PlGF) gene expression in placental villi and trophoblast cells is mediated via the protein kinase a pathway. Reprod. Sci. 2011, 18, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Newell, L.F.; Holtan, S.G. Placental growth factor: What hematologists need to know. Blood Rev. 2017, 31, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Chau, K.; Hennessy, A.; Makris, A. Placental growth factor and pre-eclampsia. J. Hum. Hypertens. 2017, 31, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibiude, J.; Guibourdenche, J.; Dionne, M.D.; Le Ray, C.; Anselem, O.; Serreau, R.; Goffinet, F.; Tsatsaris, V. Placental growth factor for the prediction of adverse outcomes in patients with suspected preeclampsia or intrauterine growth restriction. PLoS ONE 2012, 7, e50208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cvitic, S.; Desoye, G.; Hiden, U. Glucose, insulin, and oxygen interplay in placental hypervascularisation in diabetes mellitus. BioMed. Res. Int. 2014, 2014, 145846. [Google Scholar] [CrossRef] [PubMed]
- Huynh, J.; Dawson, D.; Roberts, D.; Bentley-Lewis, R. A systematic review of placental pathology in maternal diabetes mellitus. Placenta 2015, 36, 101–114. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A.; Dunk, C.; Ahmad, S.; Khaliq, A. Regulation of placental vascular endothelial growth factor (VEGF) and placenta growth factor (PIGF) and soluble Flt-1 by oxygen—A review. Placenta 2000, 21, S16–S24. [Google Scholar] [CrossRef]
- Nuzzo, A.M.; Giuffrida, D.; Moretti, L.; Re, P.; Grassi, G.; Menato, G.; Rolfo, A. Placental and maternal sFlt1/PlGF expression in gestational diabetes mellitus. Sci. Rep. 2021, 11, 2312. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.Y.T.; Lao, T.T.; Spencer, K.; Nicolaides, K.H. Maternal serum level of placental growth factor in diabetic pregnancies. J. Reprod. Med. 2004, 49, 477–480. [Google Scholar] [PubMed]
- Eleftheriades, M.; Papastefanou, I.; Lambrinoudaki, I.; Kappou, D.; Lavranos, D.; Akalestos, A.; Souka, A.P.; Pervanidou, P.; Hassiakos, D.; Chrousos, G.P. Elevated placental growth factor concentrations at 11–14 weeks of gestation to predict gestational diabetes mellitus. Metabolism 2014, 63, 1419–1425. [Google Scholar] [CrossRef]
- Gorkem, U.; Togrul, C.; Arslan, E. Relationship between elevated serum level of placental growth factor and status of gestational diabetes mellitus. J. Matern. Fetal. Neonatal. Med. 2020, 33, 4159–4163. [Google Scholar] [CrossRef] [PubMed]
- Yanachkova, V.; Staynova, R.; Naseva, E.; Kamenov, Z. The Role of Placental Growth Factor in the Prediction of Carbohydrate and Thyroid Disorders during Pregnancy. Medicina 2022, 58, 232. [Google Scholar] [CrossRef]
- Mosimann, B.; Amylidi, S.; Risch, L.; Wiedemann, U.; Surbek, D.; Baumann, M.; Stettler, C.; Raio, L. First-Trimester Placental Growth Factor in Screening for Gestational Diabetes. Fetal Diagn. Ther. 2016, 39, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsiakkas, A.; Duvdevani, N.; Wright, A.; Wright, D.; Nicolaides, K.H. Serum placental growth factor in the three trimesters of pregnancy: Effects of maternal characteristics and medical history. Ultrasound Obstet. Gynecol. 2015, 45, 591–598. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors and Reference Number | Country | Year of Publication | Sample Size (Cases/Controls) | Study Design | Biochemical Markers | GDM | ||
|---|---|---|---|---|---|---|---|---|
| Tested Marker(s) | Time of Testing (Gestational Weeks) | Diagnosis | Time of Diagnosis (Gestational Weeks) | |||||
| Ong et al. [39] | UK | 2000 | 5584 (49/4297) | Cohort | PAPP-A; hGT | 10–14 | 75 g OGTT | 24–28 |
| Benevetti et al. [40] | Italy | 2011 | 459 (228/228) | Case-control | PAPP-A; hGT | 10–13 | 50 g and 100 g OGTT | 24–28 |
| Lovati et al. [41] | Italy | 2013 | 672 (307/366) | Case-control | PAPP-A; hGT | 10–13 | 75 g OGTT | 24–28 |
| Spencer et al. [42] | UK | 2013 | 7429 (870/6559) | Cohort | PAPP-A; hGT | 10–13 | 75 g OGTT | 24–28 |
| Kulaksizoglu et al. [43] | Turkey | 2013 | (60/60) | Case-control | PAPP-A | 11–13 | 75 g OGTT | 24–28 |
| Benevetti et al. [44] | Italy | 2014 | 347 (retro.112/retro. -112) pros-18/pros-105 | Retrospective and prospective case-control | PAPP-A; hGT | 10–13 | 100 g OGTT | 24–28 |
| Wells et al. [45] | Australia | 2015 | 1664 (274/1664) | Cohort | PAPP-A | 10–14 | 75 g OGTT or 50 g GCT | After first antenatal visit (15 w) or at 26–28 w |
| Syngelaki et al. [46] | UK | 2015 | 31 225 (787/30,438) | Case-control | PAPP-A; PlGF | 11–13 | 75 g OGTT | 24–28 |
| Ferraz et al. [47] | Portugal | 2016 | 2058 (205/1853) | Retrospective cohort | PAPP-A | 11–14 | 75 g OGTT | 24–28 |
| Petry et al. [28] | UK | 2017 | 821 | Prospective and longitudinal | PAPP-A bioactive IGF | 15 (on average) | 75 g OGTT | 28 |
| Xiao et al. [48] | China | 2017 | 1585 (599/986) | Case-control | PAPP-A; hGT | 10–14 | 75 g OGTT | 24–28 |
| Ramezani et al. [49] | Iran | 2017 | 250 (172/78) | Cohort | PAPP-A | 11–14 | 75 g OGTT | 24–27 |
| Ramezani et al. [50] | Iran | 2020 | 284 (201/83) | Prospective | PAPP-A | 11–14 | 75 g OGTT | 24–28 |
| Ren et al. [51] | China | 2020 | 99 | Cohort | PAPP-A | NA | 75 g OGTT | 24–28 |
| Caliskan et al. [52] | Turkey | 2020 | 278 (120/158) | Case-control | PAPP-A; hGT | 11–13 | 50 g and 100 g OGTT | 24–28 |
| Yanachkova et al. [53] | Bulgaria | 2022 | 662 (412/250) | Retrospective case-control | PAPP-A | 10–13 | 75 g OGTT | 9–12 or 24–28 |
| Authors and Reference Number | Country | Year of Publication | Sample Size (Cases/Controls) | Study Design | Biochemical Markers | GDM | ||
|---|---|---|---|---|---|---|---|---|
| Tested Marker(s) | Time of Testing (Gestational Weeks) | Diagnosis | Time of Diagnosis (Gestational Weeks) | |||||
| Ong et al. [70] | UK | 2004 | 482 (82/400) | Cohort | PlGF | 11–14 | 75 g OGTT | 24–28 |
| Eleftheriades et al. [71] | Greece | 2014 | 134 (40/94) | Case-control | PlGF; PAPP-A; hGT | 11–14 | 75 g OGTT | 24–28 |
| Gocrem et al. [72] | Turkey | 2020 | 158 (76/82) | Cross-sectional | PlGF | N/A | 50 g GCT or 100 g OGTT | 24–28 |
| Yanachkova et al. [73] | Bulgaria | 2022 | 662 (412/250) | Retrospective, Case-control | PlGF | 10–13 | 75 g OGTT | 9–12 or 24–28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanachkova, V.; Staynova, R.; Stankova, T.; Kamenov, Z. Placental Growth Factor and Pregnancy-Associated Plasma Protein-A as Potential Early Predictors of Gestational Diabetes Mellitus. Medicina 2023, 59, 398. https://doi.org/10.3390/medicina59020398
Yanachkova V, Staynova R, Stankova T, Kamenov Z. Placental Growth Factor and Pregnancy-Associated Plasma Protein-A as Potential Early Predictors of Gestational Diabetes Mellitus. Medicina. 2023; 59(2):398. https://doi.org/10.3390/medicina59020398
Chicago/Turabian StyleYanachkova, Vesselina, Radiana Staynova, Teodora Stankova, and Zdravko Kamenov. 2023. "Placental Growth Factor and Pregnancy-Associated Plasma Protein-A as Potential Early Predictors of Gestational Diabetes Mellitus" Medicina 59, no. 2: 398. https://doi.org/10.3390/medicina59020398