

Anterior Screw Insertion Results in Greater Tibial Tunnel Enlargement Rates after Single-Bundle Anterior Cruciate Ligament Reconstruction than Posterior Insertion: A Retrospective Study
Abstract
:1. Introduction
2. Materials and Methods
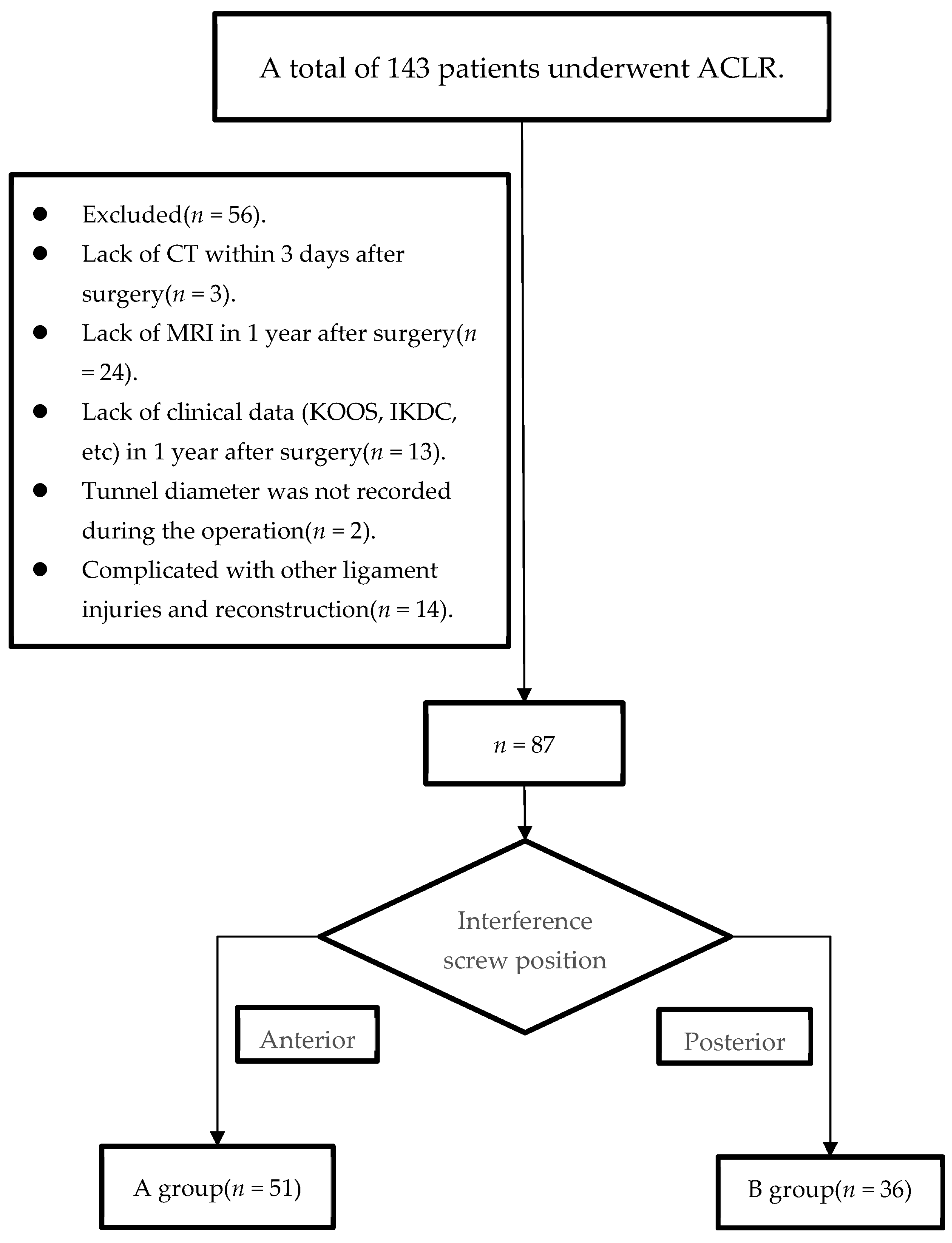
2.1. Participants
2.2. Surgical Technique
2.3. Rehabilitation
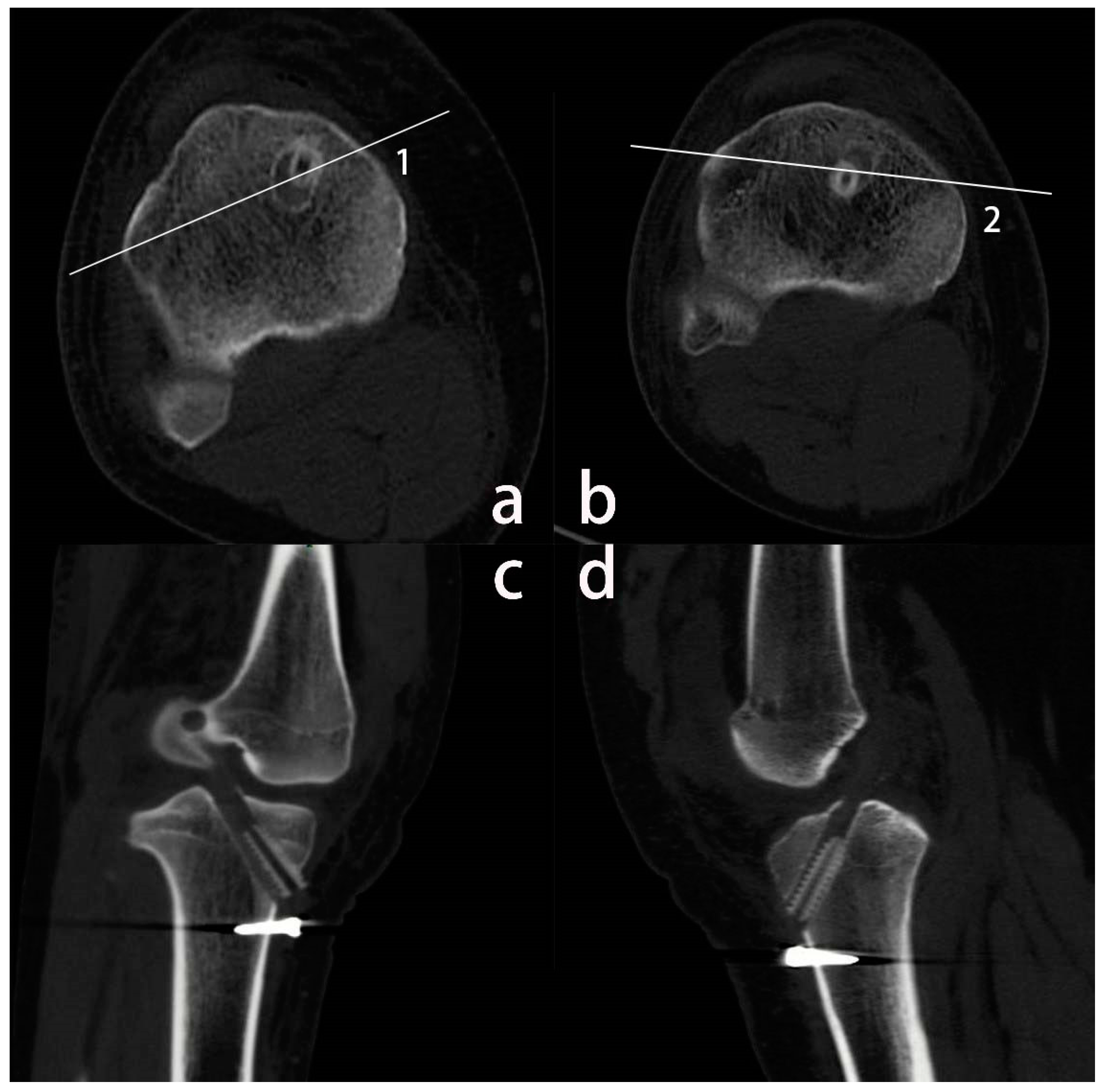
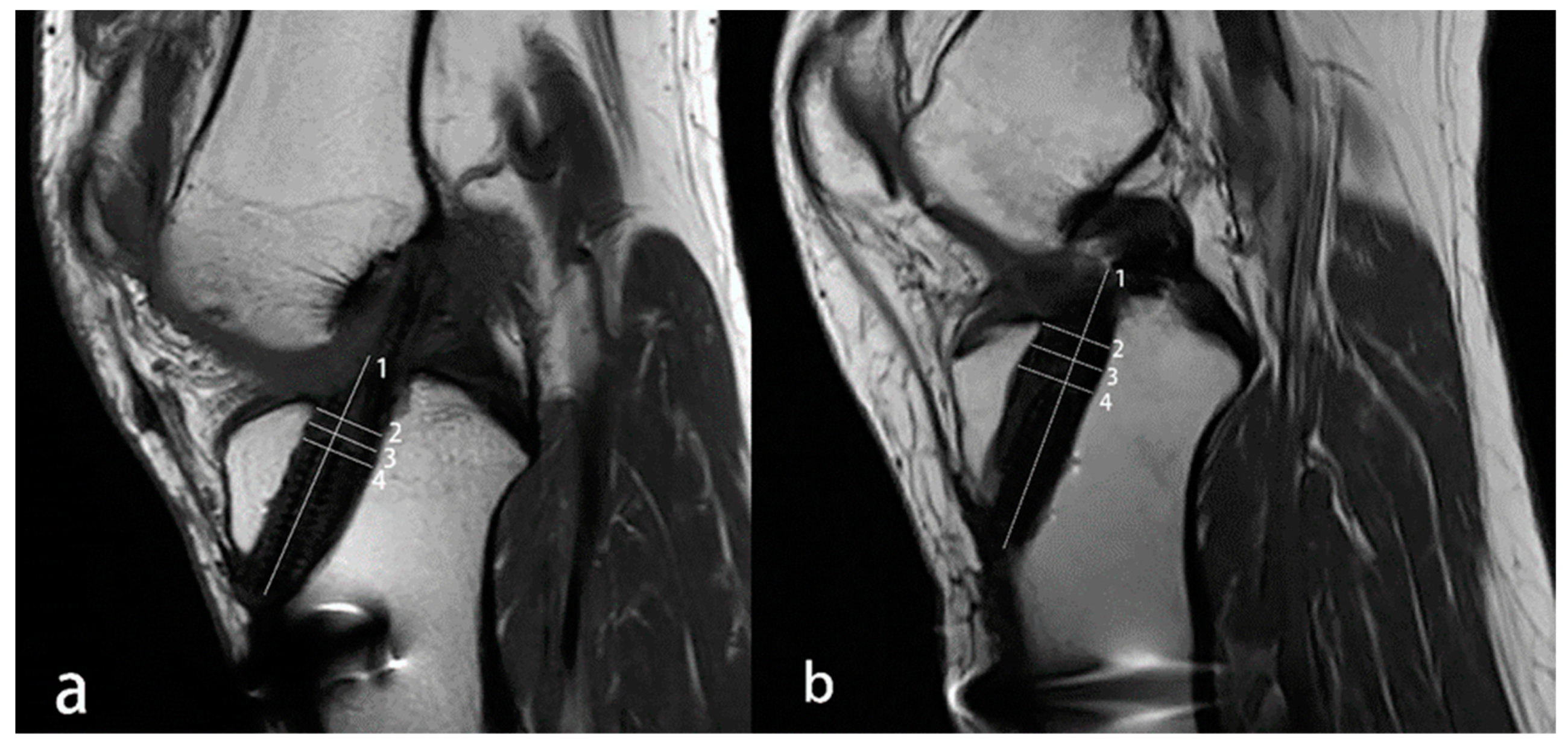
2.4. Imaging Evaluations
2.5. Clinical Evaluations
2.6. Statistical Analysis
2.7. Sample Size
3. Results
3.1. MRI Results
3.2. Clinical Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paudel, Y.R.; Sommerfeldt, M.; Voaklander, D. Increasing incidence of anterior cruciate ligament reconstruction: A 17-year population-based study. Knee Surg. Sports Traumatol. Arthrosc. 2023, 31, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Von Essen, C.; McCallum, S.; Barenius, B.; Eriksson, K. Acute reconstruction results in less sick-leave days and as such fewer indirect costs to the individual and society compared to delayed reconstruction for ACL injuries. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Mather, R.C., 3rd; Koenig, L.; Kocher, M.S.; Dall, T.M.; Gallo, P.; Scott, D.J.; Bach, B.R., Jr.; Spindler, K.P. Societal and economic impact of anterior cruciate ligament tears. J. Bone Joint Surg. Am. 2013, 95, 1751–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Graaff, S.J.A.; Meuffels, D.E.; Bierma-Zeinstra, S.M.A.; van Es, E.M.; Verhaar, J.A.N.; Eggerding, V.; Reijman, M. Why, When, and in Which Patients Nonoperative Treatment of Anterior Cruciate Ligament Injury Fails: An Exploratory Analysis of the COMPARE Trial. Am. J. Sports Med. 2022, 50, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: A systematic review and meta-analysis of the state of play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Shumborski, S.; Salmon, L.J.; Monk, C.; Heath, E.; Roe, J.P.; Pinczewski, L.A. Allograft Donor Characteristics Significantly Influence Graft Rupture After Anterior Cruciate Ligament Reconstruction in a Young Active Population. Am. J. Sports Med. 2020, 48, 2401–2407. [Google Scholar] [CrossRef]
- Kiekara, T.; Paakkala, A.; Suomalainen, P.; Huhtala, H.; Järvelä, T. Femoral and Tibial Tunnel Diameter and Bioabsorbable Screw Findings After Double-Bundle ACL Reconstruction in 5-Year Clinical and MRI Follow-up. Orthop J. Sports Med. 2017, 5, 2325967116685525. [Google Scholar] [CrossRef] [Green Version]
- Scrivens, B.; Kluczynski, M.A.; Fineberg, M.S.; Bisson, L.J. Computed Tomography Imaging of BioComposite Interference Screw After ACL Reconstruction With Bone-Patellar Tendon-Bone Graft. Orthop J. Sports Med. 2021, 9, 23259671211006477. [Google Scholar] [CrossRef]
- Siebold, R.; Cafaltzis, K. Differentiation between intraoperative and postoperative bone tunnel widening and communication in double-bundle anterior cruciate ligament reconstruction: A prospective study. Arthroscopy 2010, 26, 1066–1073. [Google Scholar] [CrossRef]
- Mermerkaya, M.U.; Atay, O.A.; Kaymaz, B.; Bekmez, S.; Karaaslan, F.; Doral, M.N. Anterior cruciate ligament reconstruction using a hamstring graft: A retrospective comparison of tunnel widening upon use of two different femoral fixation methods. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 2283–2291. [Google Scholar] [CrossRef]
- Weber, A.E.; Delos, D.; Oltean, H.N.; Vadasdi, K.; Cavanaugh, J.; Potter, H.G.; Rodeo, S.A. Tibial and Femoral Tunnel Changes After ACL Reconstruction: A Prospective 2-Year Longitudinal MRI Study. Am. J. Sports Med. 2015, 43, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Aga, C.; Wilson, K.J.; Johansen, S.; Dornan, G.; La Prade, R.F.; Engebretsen, L. Tunnel widening in single- versus double-bundle anterior cruciate ligament reconstructed knees. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1316–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Åhlén, M.; Roshani, L.; Lidén, M.; Struglics, A.; Rostgård-Christensen, L.; Kartus, J. Inflammatory cytokines and biomarkers of cartilage metabolism 8 years after anterior cruciate ligament reconstruction: Results from operated and contralateral knees. Am. J. Sports Med. 2015, 43, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Kingery, M.T.; Anil, U.; Berlinberg, E.J.; Clair, A.J.; Kenny, L.; Strauss, E.J. Changes in the Synovial Fluid Cytokine Profile of the Knee Between an Acute Anterior Cruciate Ligament Injury and Surgical Reconstruction. Am. J. Sports Med. 2022, 50, 451–460. [Google Scholar] [CrossRef]
- Amano, K.; Huebner, J.L.; Stabler, T.V.; Tanaka, M.; McCulloch, C.E.; Lobach, I.; Lane, N.E.; Kraus, V.B.; Ma, C.B.; Li, X. Synovial Fluid Profile at the Time of Anterior Cruciate Ligament Reconstruction and Its Association With Cartilage Matrix Composition 3 Years after Surgery. Am. J. Sports Med. 2018, 46, 890–899. [Google Scholar] [CrossRef]
- Lai, P.J.; Wong, C.C.; Chang, W.P.; Liaw, C.K.; Chen, C.H.; Weng, P.W. Comparison of two different types of hybrid Tibial fixations for anterior cruciate ligament reconstruction: A prospective comparative cohort study. BMC Musculoskelet Disord. 2022, 23, 1096. [Google Scholar] [CrossRef]
- Chiang, E.R.; Ma, H.L.; Wang, S.T.; Hung, S.C.; Liu, C.L.; Chen, T.H. Hamstring graft sizes differ between Chinese and Caucasians. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 916–921. [Google Scholar] [CrossRef]
- Frosch, K.H.; Sawallich, T.; Schütze, G.; Losch, A.; Walde, T.; Balcarek, P.; Konietschke, F.; Stürmer, K.M. Magnetic resonance imaging analysis of the bioabsorbable Milagro interference screw for graft fixation in anterior cruciate ligament reconstruction. Strategies Trauma Limb Reconstr 2009, 4, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Järvelä, T.; Moisala, A.S.; Paakkala, T.; Paakkala, A. Tunnel enlargement after double-bundle anterior cruciate ligament reconstruction: A prospective, randomized study. Arthroscopy 2008, 24, 1349–1357. [Google Scholar] [CrossRef]
- Kim, S.J.; Bae, J.H.; Song, S.H.; Lim, H.C. Bone tunnel widening with autogenous bone plugs versus bioabsorbable interference screws for secondary fixation in ACL reconstruction. J. Bone Joint Surg. Am. 2013, 95, 103–108. [Google Scholar] [CrossRef]
- Mayr, R.; Smekal, V.; Koidl, C.; Coppola, C.; Fritz, J.; Rudisch, A.; Kranewitter, C.; Attal, R. Tunnel widening after ACL reconstruction with aperture screw fixation or all-inside reconstruction with suspensory cortical button fixation: Volumetric measurements on CT and MRI scans. Knee 2017, 24, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Arama, Y.; Salmon, L.J.; Sri-Ram, K.; Linklater, J.; Roe, J.P.; Pinczewski, L.A. Bioabsorbable Versus Titanium Screws in Anterior Cruciate Ligament Reconstruction Using Hamstring Autograft: A Prospective, Blinded, Randomized Controlled Trial With 5-Year Follow-up. Am. J. Sports Med. 2015, 43, 1893–1901. [Google Scholar] [CrossRef] [PubMed]
- Chiang, E.R.; Chen, K.H.; Chih-Chang Lin, A.; Wang, S.T.; Wu, H.T.; Ma, H.L.; Chang, M.C.; Liu, C.L.; Chen, T.H. Comparison of Tunnel Enlargement and Clinical Outcome Between Bioabsorbable Interference Screws and Cortical Button-Post Fixation in Arthroscopic Double-Bundle Anterior Cruciate Ligament Reconstruction: A Prospective, Randomized Study With a Minimum Follow-Up of 2 Years. Arthroscopy 2019, 35, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Cai, Z.J.; Lu, W.H.; Pan, L.Y.; Yang, Y.T.; Li, Y.S.; Xiao, W.F. Eccentrically widened bone tunnels after all-inside anterior cruciate ligament reconstruction: A computed tomography and three-dimensional model-based analysis. Knee Surg. Sports Traumatol. Arthrosc. 2022. [Google Scholar] [CrossRef] [PubMed]
- Amano, H.; Tanaka, Y.; Kita, K.; Uchida, R.; Tachibana, Y.; Yonetani, Y.; Mae, T.; Shiozaki, Y.; Horibe, S. Significant anterior enlargement of femoral tunnel aperture after hamstring ACL reconstruction, compared to bone-patellar tendon-bone graft. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 461–470. [Google Scholar] [CrossRef]
- Taketomi, S.; Inui, H.; Sanada, T.; Yamagami, R.; Tanaka, S.; Nakagawa, T. Eccentric femoral tunnel widening in anatomic anterior cruciate ligament reconstruction. Arthroscopy 2014, 30, 701–709. [Google Scholar] [CrossRef]
- Buelow, J.U.; Siebold, R.; Ellermann, A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: Extracortical versus anatomical fixation. Knee Surg. Sports Traumatol. Arthrosc. 2002, 10, 80–85. [Google Scholar] [CrossRef]
- Siebold, R. Observations on bone tunnel enlargement after double-bundle anterior cruciate ligament reconstruction. Arthroscopy 2007, 23, 291–298. [Google Scholar] [CrossRef]
- Tachibana, Y.; Mae, T.; Shino, K.; Ohori, T.; Amano, H.; Yoshikawa, H.; Nakata, K. Femoral tunnel enlargement after anatomic anterior cruciate ligament reconstruction: Bone-patellar tendon-bone/single rectangular tunnel versus hamstring tendon/double tunnels. J. Orthop Sci. 2018, 23, 1011–1018. [Google Scholar] [CrossRef]
- Hatipoğlu, M.Y.; Bircan, R.; Özer, H.; Selek, H.Y.; Harput, G.; Baltacı, Y.G. Radiographic assessment of bone tunnels after anterior cruciate ligament reconstruction: A comparison of hamstring tendon and bone-patellar tendon-bone autografting technique. Jt. Dis. Relat Surg. 2021, 32, 122–128. [Google Scholar] [CrossRef]
- Ohori, T.; Mae, T.; Shino, K.; Tachibana, Y.; Yoshikawa, H.; Nakata, K. Tibial tunnel enlargement after anatomic anterior cruciate ligament reconstruction with a bone-patellar tendon-bone graft. Part 2: Factors related to the tibial tunnel enlargement. J. Orthop Sci. 2020, 25, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Bigoni, M.; Turati, M.; Gandolla, M.; Sacerdote, P.; Piatti, M.; Castelnuovo, A.; Franchi, S.; Gorla, M.; Munegato, D.; Gaddi, D.; et al. Effects of ACL Reconstructive Surgery on Temporal Variations of Cytokine Levels in Synovial Fluid. Mediators Inflamm 2016, 2016, 8243601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Fang, C.; Tao, M.; Shi, Q.; He, K.; Cheng, C.K. Hourglass-shaped grafts are superior to conventional grafts for restoring knee stability and graft force at knee flexion angle of 30° following anterior cruciate ligament reconstruction: A finite element analysis. Front Bioeng Biotechnol. 2022, 10, 967411. [Google Scholar] [CrossRef] [PubMed]
- Sinkler, M.A.; Furdock, R.J.; McMellen, C.J.; Calcei, J.G.; Voos, J.E. Biologics, Stem Cells, Growth Factors, Platelet-Rich Plasma, Hemarthrosis, and Scaffolds May Enhance Anterior Cruciate Ligament Surgical Treatment. Arthroscopy 2023, 39, 166–175. [Google Scholar] [CrossRef]
- Yao, S.; Yung, P.S.H.; Lui, P.P.Y. Tackling the Challenges of Graft Healing After Anterior Cruciate Ligament Reconstruction-Thinking From the Endpoint. Front Bioeng Biotechnol. 2021, 9, 756930. [Google Scholar] [CrossRef]
- Edwards, J.H.; Jones, G.L.; Herbert, A.; Fisher, J.; Ingham, E. Integration and functional performance of a decellularised porcine superflexor tendon graft in an ovine model of anterior cruciate ligament reconstruction. Biomaterials 2021, 279, 121204. [Google Scholar] [CrossRef]
- Baumfeld, J.A.; Diduch, D.R.; Rubino, L.J.; Hart, J.A.; Miller, M.D.; Barr, M.S.; Hart, J.M. Tunnel widening following anterior cruciate ligament reconstruction using hamstring autograft: A comparison between double cross-pin and suspensory graft fixation. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 1108–1113. [Google Scholar] [CrossRef]
- Tajima, T.; Yamaguchi, N.; Nagasawa, M.; Morita, Y.; Nakamura, Y.; Chosa, E. Early weight-bearing after anterior cruciate ligament reconstruction with hamstring grafts induce femoral bone tunnel enlargement: A prospective clinical and radiographic study. BMC Musculoskelet Disord. 2019, 20, 274. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.H.; Lee, E.S.; Lee, B.H. Paradoxical tunnel enlargement after ACL reconstruction with hamstring autografts when using β-TCP containing interference screws for tibial aperture fixation- prospectively comparative study. BMC Musculoskelet Disord. 2017, 18, 398. [Google Scholar] [CrossRef]
- Daneshvarhashjin, N.; Chizari, M.; Mortazavi, J.; Rouhi, G. Can the body slope of interference screw affect initial stability of reconstructed anterior cruciate ligament?: An in-vitro investigation. BMC Musculoskelet Disord. 2021, 22, 556. [Google Scholar] [CrossRef]
- Zhu, J.; Marshall, B.; Tang, X.; Linde, M.A.; Fu, F.H.; Smolinski, P. ACL graft with extra-cortical fixation rotates around the femoral tunnel aperture during knee flexion. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Taketomi, S. Editorial Commentary: Tunnel Widening After Anterior Cruciate Ligament Reconstruction May Increase Laxity and Complicate Revision. Arthroscopy 2021, 37, 2564–2566. [Google Scholar] [CrossRef] [PubMed]
- Jagodzinski, M.; Foerstemann, T.; Mall, G.; Krettek, C.; Bosch, U.; Paessler, H.H. Analysis of forces of ACL reconstructions at the tunnel entrance: Is tunnel enlargement a biomechanical problem? J. Biomech. 2005, 38, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Orozco, G.A.; Eskelinen, A.S.A.; Kosonen, J.P.; Tanaka, M.S.; Yang, M.; Link, T.M.; Ma, B.; Li, X.; Grodzinsky, A.J.; Korhonen, R.K.; et al. Shear strain and inflammation-induced fixed charge density loss in the knee joint cartilage following ACL injury and reconstruction: A computational study. J. Orthop Res. 2022, 40, 1505–1522. [Google Scholar] [CrossRef] [PubMed]
- Heilmeier, U.; Mamoto, K.; Amano, K.; Eck, B.; Tanaka, M.; Bullen, J.A.; Schwaiger, B.J.; Huebner, J.L.; Stabler, T.V.; Kraus, V.B.; et al. Infrapatellar fat pad abnormalities are associated with a higher inflammatory synovial fluid cytokine profile in young adults following ACL tear. Osteoarthritis Cartilage 2020, 28, 82–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigoni, M.; Sacerdote, P.; Turati, M.; Franchi, S.; Gandolla, M.; Gaddi, D.; Moretti, S.; Munegato, D.; Augusti, C.A.; Bresciani, E.; et al. Acute and late changes in intraarticular cytokine levels following anterior cruciate ligament injury. J. Orthop Res. 2013, 31, 315–321. [Google Scholar] [CrossRef]
- Zysk, S.P.; Fraunberger, P.; Veihelmann, A.; Dörger, M.; Kalteis, T.; Maier, M.; Pellengahr, C.; Refior, H.J. Tunnel enlargement and changes in synovial fluid cytokine profile following anterior cruciate ligament reconstruction with patellar tendon and hamstring tendon autografts. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 98–103. [Google Scholar] [CrossRef]
- Darabos, N.; Hundric-Haspl, Z.; Haspl, M.; Markotic, A.; Darabos, A.; Moser, C. Correlation between synovial fluid and serum IL-1beta levels after ACL surgery-preliminary report. Int. Orthop. 2009, 33, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Iorio, R.; Vadalà, A.; Di Vavo, I.; De Carli, A.; Conteduca, F.; Argento, G.; Ferretti, A. Tunnel enlargement after anterior cruciate ligament reconstruction in patients with post-operative septic arthritis. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 921–927. [Google Scholar] [CrossRef]
- Lee, B.H.; Seo, D.Y.; Bansal, S.; Kim, J.H.; Ahn, J.H.; Wang, J.H. Comparative Magnetic Resonance Imaging Study of Cross-Sectional Area of Anatomic Double Bundle Anterior Cruciate Ligament Reconstruction Grafts and the Contralateral Uninjured Knee. Arthroscopy 2016, 32, 321–329.e321. [Google Scholar] [CrossRef]
- Vignos, M.F.; Smith, C.R.; Roth, J.D.; Kaiser, J.M.; Baer, G.S.; Kijowski, R.; Thelen, D.G. Anterior Cruciate Ligament Graft Tunnel Placement and Graft Angle Are Primary Determinants of Internal Knee Mechanics After Reconstructive Surgery. Am. J. Sports Med. 2020, 48, 3503–3514. [Google Scholar] [CrossRef] [PubMed]
- Onodera, J.; Yasuda, K.; Masuda, T.; Tanabe, Y.; Kitamura, N.; Yagi, T.; Kondo, E. Is the Grafted Tendon Shifted Anteriorly in the Femoral Tunnel at the Postremodeling Phase After Anterior Cruciate Ligament Reconstruction? A Clinical MRI Study. Orthop J. Sports Med. 2017, 5, 2325967117711120. [Google Scholar] [CrossRef] [PubMed]
- Araki, D.; Kuroda, R.; Matsumoto, T.; Nagamune, K.; Matsushita, T.; Hoshino, Y.; Oka, S.; Nishizawa, Y.; Kurosaka, M. Three-dimensional analysis of bone tunnel changes after anatomic double-bundle anterior cruciate ligament reconstruction using multidetector-row computed tomography. Am. J. Sports Med. 2014, 42, 2234–2241. [Google Scholar] [CrossRef] [PubMed]
- Wilde, J.; Bedi, A.; Altchek, D.W. Revision anterior cruciate ligament reconstruction. Sports Health 2014, 6, 504–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Kubota, M.; Muramoto, K.; Kunii, T.; Sato, T.; Inui, T.; Ohno, R.; Ishijima, M. Clinical and radiographic results after ACL reconstruction using an adjustable-loop device. Asia Pac J. Sports Med. Arthrosc. Rehabil Technol 2021, 26, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Mall, N.A.; Chalmers, P.N.; Moric, M.; Tanaka, M.J.; Cole, B.J.; Bach, B.R., Jr.; Paletta, G.A., Jr. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am. J. Sports Med. 2014, 42, 2363–2370. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | p Value | |
|---|---|---|---|
| Patients, n | 51 | 36 | |
| Age, yr | 29.3 ± 9.1 | 29.5 ± 9.1 | 0.929 |
| Sex, n | 44 male and 7 Female | 29 male and 7 female | 0.475 |
| BMI (kg/m2) | 23.84 ± 2.23 | 23.82 ± 3.28 | 0.970 |
| MRI follow-up, mo | 14.86 ± 1.96 | 15.33 ± 2.02 | 0.282 |
| Tibial tunnel diameter, mm | 8.1 ± 0.6 | 8.1 ± 0.7 | 0.775 |
| Tibial tunnel length, mm | 43.8 ± 4.8 | 42.4 ± 4.5 | 0.175 |
| Graft length, mm | 83.1 ± 10.4 | 81.9 ± 10.5 | 0.593 |
| Meniscus tear, n | 26 | 17 | 0.730 |
| Meniscus suture, n | 19 | 13 | 0.913 |
| Cutting Levels | Interobserver | Intraobserver | |
|---|---|---|---|
| 1 | 2 | ||
| joint line level | 0.897 | 0.922 | 0.891 |
| center level | 0.881 | 0.870 | 0.883 |
| screw top level | 0.898 | 0.919 | 0.926 |
| Group A | Group B | p Value | |
|---|---|---|---|
| TER-joint line (SD), % | 43.77 ± 18.90 | 31.67 ± 19.05 | 0.004 |
| TER-center (SD), % | 43.99 ± 18.70 | 34.64 ± 21.08 | 0.032 |
| TER-screw top (SD), % | 41.75 ± 20.72 | 35.11 ± 22.33 | 0.157 |
| TER-average (SD), % | 43.17 ± 18.33 | 33.80 ± 19.30 | 0.024 |
| Group A | Group A | p Value for A vs. B, Postop | |||||
|---|---|---|---|---|---|---|---|
| Preop | Postop | p Value | Preop | Postop | p Value | ||
| Lachman test (+) | 43/51 | 2/51 | p < 0.01 | 28/36 | 3/36 | p < 0.01 | 0.687 |
| IKDC | 62.22 ± 12.78 | 83.75 ± 7.75 | 0.012 | 61.58 ± 15.19 | 80.78 ± 6.08 | 0.029 | 0.058 |
| KOOS | |||||||
| Symptoms | 73.79 ± 15.59 | 88.75 ± 6.51 | p < 0.01 | 75.30 ± 13.48 | 87.19 ± 6.31 | p < 0.01 | 0.268 |
| Pain | 84.03 ± 11.39 | 97.89 ± 1.47 | p < 0.01 | 83.77 ± 11.60 | 97.62 ± 1.86 | p < 0.01 | 0.460 |
| ADL | 84.95 ± 10.00 | 96.67 ± 1.93 | p < 0.01 | 84.38 ± 9.86 | 96.93 ± 1.64 | p < 0.01 | 0.519 |
| Sports | 46.23 ± 20.78 | 77.82 ± 11.39 | p < 0.01 | 41.78 ± 17.55 | 80.48 ± 10.27 | p < 0.01 | 0.268 |
| QOL | 28.44 ± 11.72 | 76.99 ± 12.96 | p < 0.01 | 26.67 ± 11.86 | 77.39 ± 15.54 | p < 0.01 | 0.897 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kong, Y.; Yin, L.; Zhang, H.; Yan, W.; Chen, J.; Zhou, A.; Zhang, J. Anterior Screw Insertion Results in Greater Tibial Tunnel Enlargement Rates after Single-Bundle Anterior Cruciate Ligament Reconstruction than Posterior Insertion: A Retrospective Study. Medicina 2023, 59, 390. https://doi.org/10.3390/medicina59020390
Kong Y, Yin L, Zhang H, Yan W, Chen J, Zhou A, Zhang J. Anterior Screw Insertion Results in Greater Tibial Tunnel Enlargement Rates after Single-Bundle Anterior Cruciate Ligament Reconstruction than Posterior Insertion: A Retrospective Study. Medicina. 2023; 59(2):390. https://doi.org/10.3390/medicina59020390
Chicago/Turabian StyleKong, Yangang, Lifeng Yin, Hua Zhang, Wenlong Yan, Jiaxing Chen, Aiguo Zhou, and Jian Zhang. 2023. "Anterior Screw Insertion Results in Greater Tibial Tunnel Enlargement Rates after Single-Bundle Anterior Cruciate Ligament Reconstruction than Posterior Insertion: A Retrospective Study" Medicina 59, no. 2: 390. https://doi.org/10.3390/medicina59020390