
Clinical Implications of Cardiac Symptoms and Electrocardiographic Abnormalities for Advanced Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Enrolled Participants
2.2. Acquisition and Definition of Clinical Variables
2.3. Definition of Nonalcoholic Fatty Liver Disease and Advanced Fibrosis
2.4. Assessment of ECG Abnormalities and Cardiac Symptoms
2.5. Statistical Analysis
3. Results
3.1. Baseline Demographic and Clinical Characteristics of the Participants
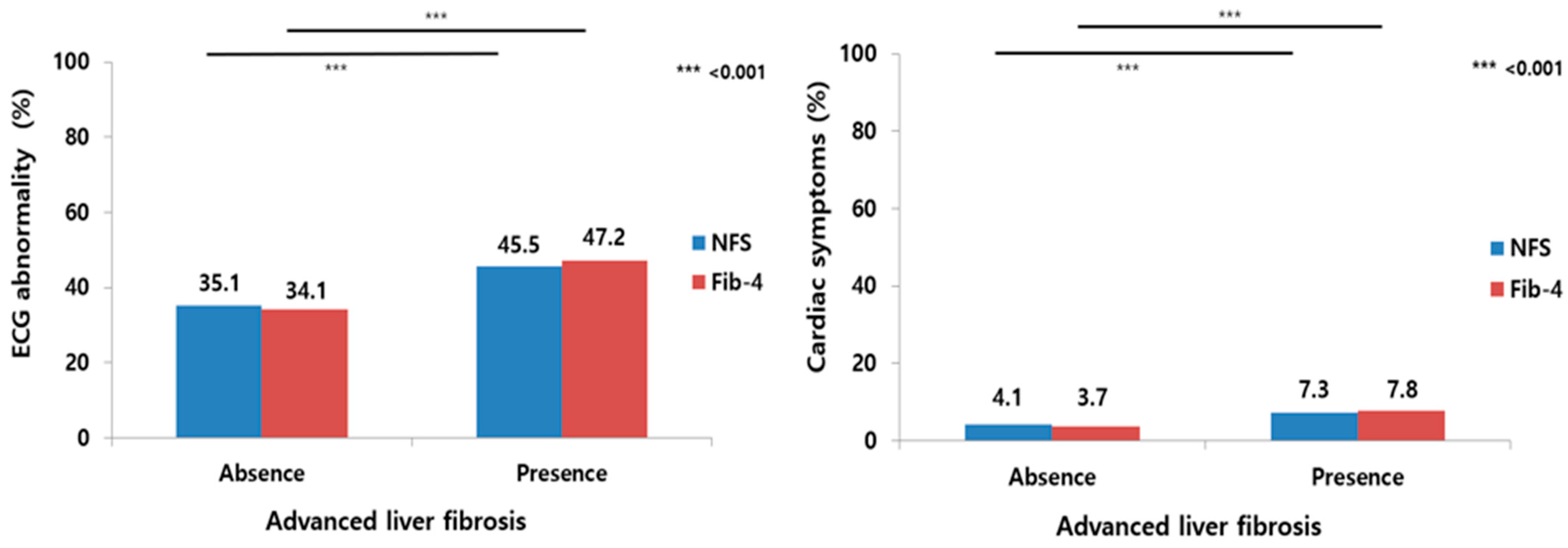
3.2. Percentage of Cardiac Manifestations According to the Presence or Absence of Advanced Liver Fibrosis, as Defined by Two Fibrosis Scoring Systems
3.3. Effects of ECG Abnormalities and Cardiac Symptoms on Advanced Liver Fibrosis in Patients with NAFLD
3.4. Variables Associated with Advanced Liver Fibrosis for Cardiac Symptoms with ECG Abnormalities in Patients with NAFLD
3.5. Step-Wise Adjustment to Identify the Association of Cardiac Symptoms with Abnormal ECGs and Advanced Fibrosis in Patients with NAFLD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kang, S.H.; Lee, H.W.; Yoo, J.-J.; Cho, Y.; Kim, S.U.; Lee, T.H.; Jang, B.K.; Kim, S.G.; Ahn, S.B.; Kim, H.; et al. KASL clinical practice guidelines: Management of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2021, 27, 363–401. [Google Scholar] [CrossRef] [PubMed]
- Le, M.H.; Yeo, Y.H.; Zou, B.; Barnet, S.; Henry, L.; Cheung, R.; Nguyen, M.H. Forecasted 2040 global prevalence of nonalcoholic fatty liver disease using hierarchical bayesian approach. Clin. Mol. Hepatol. 2022, 28, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F.; et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Roelstraete, B.; Khalili, H.; Hagström, H.; Ludvigsson, J.F. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: Results from a nationwide cohort. Gut 2021, 70, 1375–1382. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver; Clinical Practice Guideline Panel; EASL Governing Board Representative. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis–2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Adams, L.A.; Anstee, Q.M.; Tilg, H.; Targher, G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66, 1138–1153. [Google Scholar] [CrossRef] [Green Version]
- Henson, J.B.; Simon, T.G.; Kaplan, A.; Osganian, S.; Masia, R.; Corey, K.E. Advanced fibrosis is associated with incident cardiovascular disease in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2020, 51, 728–736. [Google Scholar] [CrossRef]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111S, 154170. [Google Scholar] [CrossRef]
- Targher, G.; Corey, K.E.; Byrne, C.D. NAFLD, and cardiovascular and cardiac diseases: Factors influencing risk, prediction and treatment. Diabetes Metab. 2021, 47, 101215. [Google Scholar] [CrossRef] [PubMed]
- Alon, L.; Corica, B.; Raparelli, V.; Cangemi, R.; Basili, S.; Proietti, M.; Romiti, G.F. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2022, 29, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Velasco, A.; Hage, F.G.; Reyes, E. Guidelines in review: Comparison of ESC and ACC/AHA guidelines for the diagnosis and management of patients with stable coronary artery disease. J. Nucl. Cardiol. 2018, 25, 509–515. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Grundy, S.M. Metabolic syndrome update. Trends Cardiovasc. Med. 2016, 26, 364–373. [Google Scholar] [CrossRef]
- Farrell, G.C.; Chitturi, S.; Lau, G.K.; Sollano, J.D.; Asia-Pacific Working Party on NAFLD. Guidelines for the assessment and management of non-alcoholic fatty liver disease in the Asia-Pacific region: Executive summary. J. Gastroenterol. Hepatol. 2007, 22, 775–777. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Chan, W.K.; Chitturi, S.; Chawla, Y.; Dan, Y.Y.; Duseja, A.; Fan, J.; Goh, K.-L.; Hamaguchi, M.; Hashimoto, E.; et al. Asia-Pacific Working Party on Non-alcoholic Fatty Liver Disease guidelines 2017-Part 1: Definition, risk factors and assessment. J. Gastroenterol. Hepatol. 2018, 33, 70–85. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J.; Nash Clinical Research Network. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, A.H.; Ribeiro, M.H.; Paixao, G.M.M.; Oliveira, D.M.; Gomes, P.R.; Canazart, J.A.; Ferreira, M.; Andersson, C.; Macfarlane, P.; Meira, W., Jr.; et al. Automatic diagnosis of the 12-lead ECG using a deep neural network. Nat. Commun. 2020, 11, 1760. [Google Scholar] [CrossRef] [Green Version]
- Parlati, L.; Regnier, M.; Guillou, H.; Postic, C. New targets for NAFLD. JHEP Rep. 2021, 3, 100346. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Di Minno, M.N.; Di Minno, A.; Ambrosino, P.; Songia, P.; Tremoli, E.; Poggio, P. Aortic valve sclerosis as a marker of atherosclerosis: Novel insights from hepatic steatosis. Int. J. Cardiol. 2016, 217, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Dauriz, M.; Sandri, D.; Bonapace, S.; Zoppini, G.; Tilg, H.; Byrne, C.D.; Targher, G. Association between non-alcoholic fatty liver disease and risk of atrial fibrillation in adult individuals: An updated meta-analysis. Liver Int. 2019, 39, 758–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijarnpreecha, K.; Lou, S.; Panjawatanan, P.; Cheungpasitporn, W.; Pungpapong, S.; Lukens, F.J.; Ungprasert, P. Association between diastolic cardiac dysfunction and nonalcoholic fatty liver disease: A systematic review and meta-analysis. Dig. Liver Dis. 2018, 50, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhou, X.; Wu, S.; Fan, D.; Van Poucke, S.; Chen, Y.; Fu, S.; Zheng, M. Nonalcoholic fatty liver disease contributes to subclinical atherosclerosis: A systematic review and meta-analysis. Hepatol. Commun. 2018, 2, 376–392. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Lee, Y.H.; Kim, Y.D.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; et al. Nonalcoholic Fatty Liver Disease and Sarcopenia Are Independently Associated With Cardiovascular Risk. Am. J. Gastroenterol. 2020, 115, 584–595. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Cao, Y.; Jin, J.; Hua, Q.; Li, Y.; Guo, Y.; Zhu, C.; Wu, N.; Gao, R.; Li, J. Liver Fibrosis Scoring Systems as Novel Tools for Predicting Cardiovascular Outcomes in Patients Following Elective Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2021, 10, e018869. [Google Scholar] [CrossRef]
- Gil Park, J.; Jung, J.; Verma, K.K.; Kang, M.K.; Madamba, E.; Lopez, S.; Yonan, A.Q.; Liu, A.; Bettencourt, R.; Sirlin, C.; et al. Liver stiffness by magnetic resonance elastography is associated with increased risk of cardiovascular disease in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2021, 53, 1030–1037. [Google Scholar]
- Yi, M.; Peng, W.; Teng, F.; Kong, Q.; Chen, Z. The role of noninvasive scoring systems for predicting cardiovascular disease risk in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2022, 34, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Hagström, H.; Talbäck, M.; Andreasson, A.; Walldius, G.; Hammar, N. Ability of noninvasive scoring systems to identify individuals in the population at risk for severe liver disease. Gastroenterology 2020, 158, 200–214. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Cardiac Symptoms n = 304 (4.8%) | No Cardiac Symptoms n = 5989 (95.2%) | p-Value |
|---|---|---|---|
| Age (yr) | 57.4 ± 9.8 | 51.8 ± 9.3 | <0.001 |
| Male, n (%) | 177 (58.2) | 3486 (58.2) | 0.975 |
| BMI, kg/m2 | 25.6 ± 2.7 | 25.2 ± 2.6 | 0.025 |
| WC (cm) | 85.5 ± 7.5 | 84.0 ± 7.3 | <0.001 |
| Comorbidities | |||
| Obesity, n (%) | 163 (53.6) | 2886 (48.2) | 0.074 |
| Diabetes mellitus, n (%) | 36 (11.8) | 560 (9.4) | 0.178 |
| Hypertension, n (%) | 58 (19.1) | 984 (16.4) | 0.257 |
| Metabolic syndrome, n (%) | 64 (21.1) | 1109 (18.5) | 0.302 |
| ECG findings | |||
| ECG abnormality, n (%) | 167 (54.9) | 2198 (36.7) | <0.001 |
| Atrial fibrillation, n (%) | 20 (6.6) | 39 (0.7) | <0.001 |
| Major cardiac symptoms | |||
| Chest discomfort, n (%) | 144 (47.4) | ||
| Palpitation, n (%) | 44 (14.5) | ||
| Chest pain, n (%) | 39 (12.8) | ||
| Shortness of breath, n (%) | 34 (11.2) | ||
| Near fainting (presyncope), n (%) | 22 (7.2) | ||
| Dizziness, n (%) | 21 (6.9) | ||
| Liver profile | |||
| AST, IU/L | 27.8 ± 12.8 | 26.9 ± 12.3 | 0.223 |
| ALT, IU/L | 30.5 ± 18.6 | 31.2 ± 20.5 | 0.474 |
| PLT, K/uL | 238.5 ± 53.8 | 249.3 ± 58.2 | 0.002 |
| GGT, IU/L | 33.7 ± 24.8 | 36.0 ± 37.7 | 0.117 |
| Albumin, g/dL | 4.7 ± 0.3 | 4.7 ± 0.6 | 0.069 |
| Metabolic profiles | |||
| FPG, mg/dL | 102.7 ± 20.3 | 101.6 ± 24.7 | 0.392 |
| TC, mg/dL | 205.4 ± 44.9 | 208.5 ± 39.0 | 0.246 |
| TG, mg/dL | 148.4 ± 99.7 | 150.7 ± 91.1 | 0.698 |
| HDL, mg/dL | 55.4 ± 14.0 | 53.7 ± 13.5 | 0.031 |
| LDL, mg/dL | 120.3 ± 42.5 | 124.7 ± 36.7 | 0.082 |
| hsCRP, mg/dL | 0.15 ± 0.25 | 0.13 ± 0.30 | 0.073 |
| Fibrosis scoring system | |||
| NAFLD fibrosis score | −1.8 ± 1.1 | −2.3 ± 1.1 | <0.001 |
| Fibrosis-4 index | 1.3 ± 0.6 | 1.1 ± 0.5 | <0.001 |
| Advanced fibrosis | |||
| NAFLD fibrosis score, n (%) | 78 (25.7) | 1127 (18.8) | 0.004 |
| Fibrosis-4 index, n (%) | 98 (32.2) | 1274 (21.3) | <0.001 |
| ECG Abnormality | Cardiac Symptoms | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| OR for advanced fibrosis by NFS | ||||
| Unadjusted | 1.37 (1.21–1.56) | <0.001 | 1.49 (1.14–1.94) | 0.003 |
| Sex adjusted | 1.35 (1.19–1.53) | <0.001 | 1.49 (1.14–1.94) | 0.003 |
| Model 1 | 1.35 (1.18–1.54) | <0.001 | 1.44 (1.10–1.88) | 0.008 |
| Model 2 | 1.40 (1.23–1.60) | <0.001 | 1.44 (1.09–1.89) | 0.009 |
| Model 3 | 1.38 (1.21–1.58) | <0.001 | 1.40 (1.06–1.85) | 0.018 |
| OR for advanced fibrosis by Fib-4 | ||||
| Unadjusted | 1.63 (1.45–1.84) | <0.001 | 1.76 (1.37–2.26) | <0.001 |
| Sex adjusted | 1.63 (1.45–1.84) | <0.001 | 1.76 (1.37–2.26) | <0.001 |
| Model 1 | 1.64 (1.45–1.85) | <0.001 | 1.72 (1.34–2.21) | <0.001 |
| Model 2 | 1.63 (1.44–1.84) | <0.001 | 1.67 (1.30–2.15) | <0.001 |
| Model 3 | 1.63 (1.44–1.85) | <0.001 | 1.67 (1.30–2.15) | <0.001 |
| Variables | Advanced Fibrosis Using NFS * | Advanced Fibrosis Using Fib-4 † | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate p-Value | Multivariable | Univariate p-Value | Multivariable | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| Age, years *,† | <0.001 | <0.001 | ||||||
| Male | 0.398 | 0.103 | ||||||
| T2DM * | <0.001 | 1.54 | 1.21–1.95 | <0.001 | ||||
| Hypertension | <0.001 | 1.87 | 1.53–2.28 | <0.001 | <0.001 | 1.57 | 1.29–1.90 | <0.001 |
| Obesity | <0.001 | 2.20 | 1.86–2.61 | <0.001 | 0.012 | |||
| FBS, mg/dL | <0.001 | 7.11 | 5.17–9.88 | <0.001 | 0.002 | |||
| GGT, U/L | 0.321 | 0.221 | ||||||
| Albumin, g/dL * | <0.001 | 0.69 | 0.53–0.92 | 0.011 | ||||
| hsCRP, mg/L | 0.001 | 1.01 | 1.00–1.03 | 0.028 | 0.300 | |||
| TC, mg/dL | <0.001 | <0.001 | ||||||
| TG, mg/dL | 0.281 | 0.072 | ||||||
| HDL-C, mg/dL | 0.002 | 0.333 | ||||||
| Symptoms with abnormal ECG | <0.001 | 2.36 | 1.67–3.31 | <0.001 | <0.001 | 3.02 | 2.19–4.15 | <0.001 |
| Cardiac Symptoms with Abnormal ECG | ||
|---|---|---|
| OR (95% CI) | p-Value | |
| OR for advanced fibrosis by NFS | ||
| Unadjusted | 2.59 (1.88–3.56) | <0.001 |
| Gender adjusted | 2.59 (1.88–3.56) | <0.001 |
| Model 1 | 2.45 (1.76–3.38) | <0.001 |
| Model 2 | 2.49 (1.78–3.47) | <0.001 |
| Model 3 | 2.43 (1.72–3.39) | <0.001 |
| OR for advanced fibrosis by Fib-4 | ||
| Unadjusted | 3.20 (2.33–4.37) | <0.001 |
| Gender adjusted | 3.22 (2.35–4.41) | <0.001 |
| Model 1 | 3.15 (2.30–4.33) | <0.001 |
| Model 2 | 3.09 (2.25–4.25) | <0.001 |
| Model 3 | 3.02 (2.19–4.15) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, M.-K.; Kim, M.-C. Clinical Implications of Cardiac Symptoms and Electrocardiographic Abnormalities for Advanced Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Medicina 2023, 59, 375. https://doi.org/10.3390/medicina59020375
Kang M-K, Kim M-C. Clinical Implications of Cardiac Symptoms and Electrocardiographic Abnormalities for Advanced Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Medicina. 2023; 59(2):375. https://doi.org/10.3390/medicina59020375
Chicago/Turabian StyleKang, Min-Kyu, and Min-Cheol Kim. 2023. "Clinical Implications of Cardiac Symptoms and Electrocardiographic Abnormalities for Advanced Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease" Medicina 59, no. 2: 375. https://doi.org/10.3390/medicina59020375