
Failed Attempt to Recommend Noise Cancelling Headphones for Knee Arthroplasty Surgeons—Results of a Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
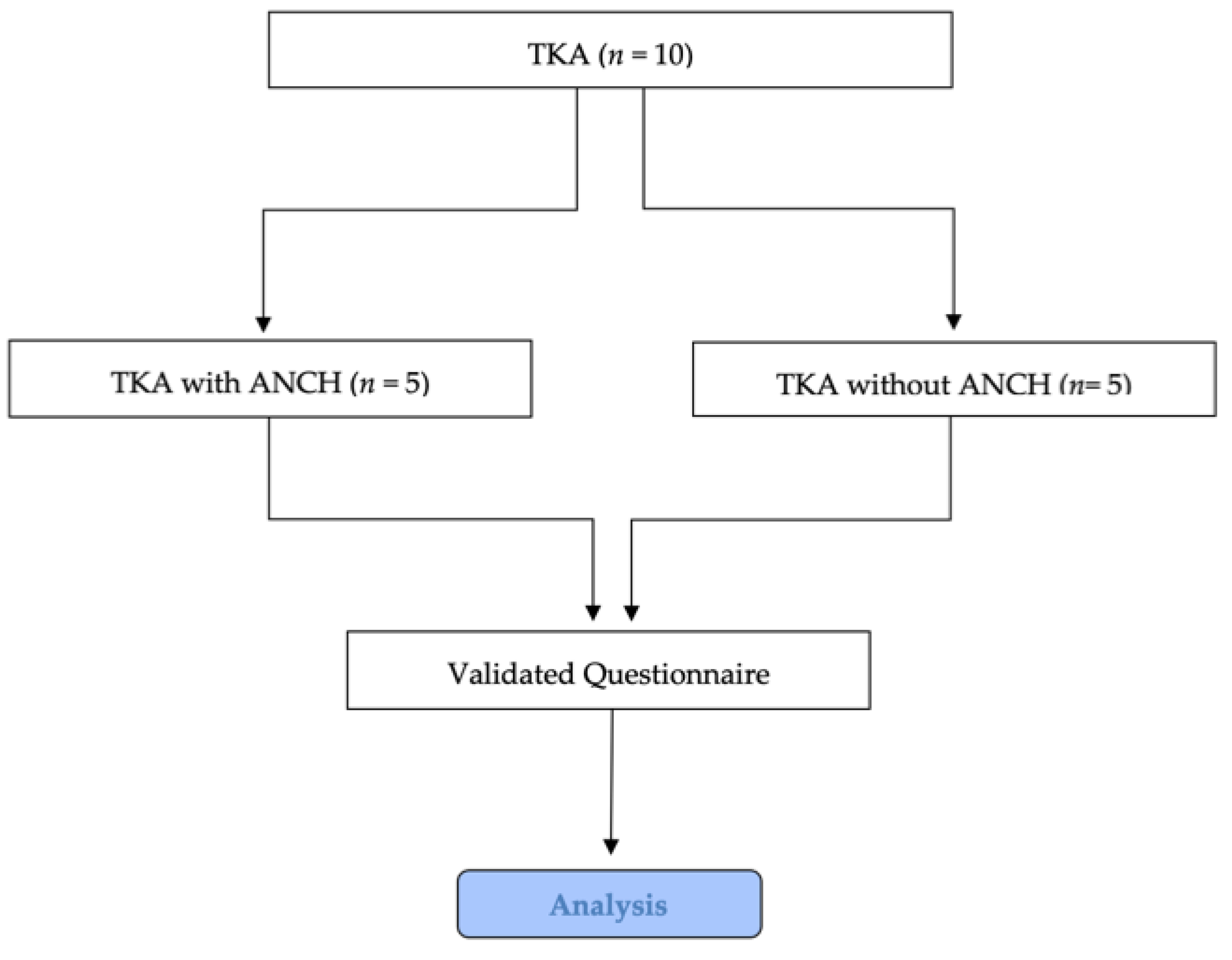
2.1. Study Design and Technical Implementation
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palmer, J.S.; Fraig, H.H.; Wilson, C.J.; Garrett, S.J.W. Noise Evaluation of Arthroplasty Theaters: Results From the NEAT Study. J. Arthroplast. 2020, 36, 1819–1822. [Google Scholar] [CrossRef]
- Simpson, J.; Hamer, A. How Noisy Are Total Knee and Hip Replacements? J. Perioper. Pract. 2017, 27, 292–295. [Google Scholar] [CrossRef]
- Hawi, N.; Alazzawi, S.; Schmitz, A.; Kreibich, T.; Gehrke, T.; Kendoff, D.; Haasper, C. Noise Levels during Total Hip Arthroplasty: The Silent Health Hazard. HIP Int. 2019, 30, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Murphy, W.; Franks, J. NIOSH Criteria for a Recommended Standard: Occupational Noise Exposure, Revised Criteria 1998. J. Acoust. Soc. Am. 2002, 111, 2397. [Google Scholar] [CrossRef]
- Siegel, M.G. The Risk of Noise-Induced Hearing Loss Performing Knee Replacement Surgery. Noise Health 2019, 21, 183–188. [Google Scholar] [CrossRef]
- Levin, M.; Zhou, K.; Sommer, E.C.; Purohit, H.; Wells, J.; Pugi, J.; Sommer, D.D. Noise in Endoscopic Sinus and Skull Base Surgery Operating Rooms. Am. J. Rhinol. Allergy 2021, 35, 541–547. [Google Scholar] [CrossRef]
- Hodge, B.; Thompson, J.F. Noise Pollution in the Operating Theatre. Lancet 1990, 335, 891–894. [Google Scholar] [CrossRef]
- Drzymalski, D.M.; Ceruzzi, J.; Camann, W.R. Noise in the Obstetric Operating Room. Int. J. Obstet. Anesth. 2017, 29, 87–88. [Google Scholar] [CrossRef]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and Non-Auditory Effects of Noise on Health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Brammer, A.J.; Laroche, C. Noise and Communication: A Three-Year Update. Noise Health 2012, 14, 281–286. [Google Scholar] [CrossRef]
- Keller, S.; Tschan, F.; Beldi, G.; Kurmann, A.; Candinas, D.; Semmer, N.K. Noise Peaks Influence Communication in the Operating Room. An Observational Study. Ergonomics 2016, 59, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Konkani, A.; Oakley, B. Noise in Hospital Intensive Care Units—A Critical Review of a Critical Topic. J. Crit. Care 2012, 27, 522.e1–522.e9. [Google Scholar] [CrossRef]
- Choiniere, D.B. The Effects of Hospital Noise. Nurs. Adm. Q. 2010, 34, 327–333. [Google Scholar]
- Busch-Vishniac, I.J.; West, J.E.; Barnhill, C.; Hunter, T.; Orellana, D.; Chivukula, R. Noise Levels in Johns Hopkins Hospital. J. Acoust. Soc. Am. 2005, 118, 3629–3645. [Google Scholar] [CrossRef]
- Willett, K. Noise-Induced Hearing Loss in Orthopaedic Staff. J. Bone Jt. Surgery. 1991, 73, 113–115. [Google Scholar] [CrossRef] [PubMed]
- Imam, L.; Hannan, S.A. Noise-Induced Hearing Loss: A Modern Epidemic? Br. J. Hosp. Med. 2017, 78, 286–290. [Google Scholar] [CrossRef]
- Thorne, P.; Ameratunga, S.; Stewart, J.; Reid, N.; Williams, W.; Purdy, S.; Dodd, G.; Wallaart, J. Epidemiology of Noise Induced Hearing Loss In New Zealand. New Zealand Med. J. 2008, 121, 33–44. [Google Scholar]
- Cheriyan, S.; Mowery, H.; Ruckle, D.; Keheila, M.; Myklak, K.; Alsyouf, M.; Atiga, C.; Khuri, J.; Khater, N.; Faaborg, D.; et al. The Impact of Operating Room Noise Upon Communication During Percutaneous Nephrostolithotomy. J. Endourol. 2016, 30, 1062–1066. [Google Scholar] [CrossRef]
- Fu, V.X.; Oomens, P.; Merkus, N.; Jeekel, J. The Perception and Attitude Toward Noise and Music in the Operating Room: A Systematic Review. J. Surg. Res. 2021, 263, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Dholakia, S.; Jeans, J.P.; Khalid, U.; Dholakia, S.; D’Souza, C.; Nemeth, K. The Association of Noise and Surgical-Site Infection in Day-Case Hernia Repairs. Surgery 2015, 157, 1153–1156. [Google Scholar] [CrossRef]
- Engelmann, C.R.; Neis, J.P.; Kirschbaum, C.; Grote, G.; Ure, B.M. A Noise-Reduction Program in a Pediatric Operation Theatre Is Associated With Surgeon’s Benefits and a Reduced Rate of Complications: A Prospective Controlled Clinical Trial. Ann. Surg. 2014, 259, 1025–1033. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.S.; Kuo, S.M. An Integrated Audio and Active Noise Control Headset. IEEE Trans. Consum. Electron. 2002, 48, 242–247. [Google Scholar] [CrossRef]
- Foo, S.W.; Senthilkumar, T.N.; Averty, C. Active Noise Cancellation Headset. In Proceedings of the IEEE International Symposium on Circuits and Systems (ISCAS), Kobe, Japan, 23–26 May 2005; Volume 1, pp. 268–271. [Google Scholar] [CrossRef]
- Akhtar, S.; Weigle, C.G.M.; Cheng, E.Y.; Toohill, R.; Berens, R.J. Use of Active Noise Cancellation Devices in Caregivers in the Intensive Care Unit. Crit. Care Med. 2000, 28, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, S.; Enki, D.; Stevens, S.; Bennett, M.J. An Experimental Model to Measure the Ability of Headphones with Active Noise Control to Reduce Patient’s Exposure to Noise in an Intensive Care Unit. Intensive Care Med. Exp. 2017, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Townsend, C.B.; Bravo, D.; Jones, C.; Matzon, J.L.; Ilyas, A.M. Noise-Canceling Headphones and Music Decrease Intraoperative Patient Anxiety During Wide-Awake Hand Surgery: A Randomized Controlled Trial. J. Hand Surg. Glob. Online 2021, 3, 254–259. [Google Scholar] [CrossRef]
- Lee, B.C.; Kim, H.O.; Chung, H.S.; Heo, S.H.; Jeong, Y.Y.; Kim, M.S.; Hwang, E.C.; Jung, S.I.; Kwon, D.; Park, K. Does Music from Noise-Canceling Headphones Have a Beneficial Effect on Men Undergoing Transrectal Ultrasound-Guided Prostate Biopsy? Prostate Int. 2021, 9, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Weldon, S.-M.; Korkiakangas, T.; Bezemer, J.; Kneebone, R. Music and Communication in the Operating Theatre. J. Adv. Nurs. 2015, 71, 2763–2774. [Google Scholar] [CrossRef]
- Tsafrir, Z.; Janosek-Albright, K.; Aoun, J.; Diaz-Insua, M.; Abd-El-Barr, A.-E.-R.; Schiff, L.; Talukdar, S.; Menon, M.; Munkarah, A.; Theoharis, E.; et al. The Impact of a Wireless Audio System on Communication in Robotic-Assisted Laparoscopic Surgery: A Prospective Controlled Trial. PLoS ONE 2020, 15, e0220214. [Google Scholar] [CrossRef] [PubMed]
- Sexton, J.B.; Helmreich, R.L.; Neilands, T.B.; Rowan, K.; Vella, K.; Boyden, J.; Roberts, P.R.; Thomas, E.J. The Safety Attitudes Questionnaire: Psychometric Properties, Benchmarking Data, and Emerging Research. BMC Health Serv. Res. 2006, 6, 44. [Google Scholar] [CrossRef]
- Watts, B.V.; Percarpio, K.; West, P.; Mills, P.D. Use of the Safety Attitudes Questionnaire as a Measure in Patient Safety Improvement. J. Patient Saf. 2010, 6, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Weldon, S.-M.; Korkiakangas, T.; Bezemer, J.; Kneebone, R. Communication in the Operating Theatre. Br. J. Surg. 2013, 100, 1677–1688. [Google Scholar] [CrossRef]
- Gawande, A.A.; Zinner, M.J.; Studdert, D.M.; Brennan, T.A. Analysis of Errors Reported by Surgeons at Three Teaching Hospitals. Surgery 2003, 133, 614–621. [Google Scholar] [CrossRef]
- Suliburk, J.W.; Buck, Q.M.; Pirko, C.J.; Massarweh, N.N.; Barshes, N.R.; Singh, H.; Rosengart, T.K. Analysis of Human Performance Deficiencies Associated With Surgical Adverse Events. JAMA Netw. Open 2019, 2, e198067. [Google Scholar] [CrossRef]
- McNeer, R.R.; Bennett, C.L.; Horn, D.B.; Dudaryk, R. Factors Affecting Acoustics and Speech Intelligibility in the Operating Room: Size Matters. Anesth. Analg. 2017, 124, 1978–1985. [Google Scholar] [CrossRef] [PubMed]
- Mcleod, R.; Myint-Wilks, L.; Davies, S.; Elhassan, H. The Impact of Noise in the Operating Theatre: A Review of the Evidence. Ann. R. Coll. Surg. Engl. 2021, 103, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Shamji, F.M.; Deslauriers, J. Sharing the Airway: The Importance of Good Communication Between Anesthesiologist and Surgeon. Thorac. Surg. Clin. 2018, 28, 257–261. [Google Scholar] [CrossRef]
- Goffin, J.S.O.; MacDonald, D.R.W.; Neilly, D.; Munro, C.; Ashcroft, G.P. Evaluation of Sound Levels in Elective Orthopaedic Theatres during Primary Hip and Knee Arthroplasty. Surgeon 2021, 20, 225–230. [Google Scholar] [CrossRef]
- Hönecke, T.; Schwarze, M.; Wangenheim, M.; Savov, P.; Windhagen, H.; Ettinger, M. Noise Exposure during Robot-Assisted Total Knee Arthroplasty. Arch. Orthop. Trauma Surg. 2022. [Google Scholar] [CrossRef]
- Love, H. Noise Exposure in the Orthopaedic Operating Theatre: A Significant Health Hazard. ANZ J. Surg. 2003, 73, 836–838. [Google Scholar] [CrossRef]
- El Boghdady, M.; Ewalds-Kvist, B.M. The Influence of Music on the Surgical Task Performance: A Systematic Review. Int. J. Surg. 2020, 73, 101–112. [Google Scholar] [CrossRef]
- Mosaed, S.; Vahidi, R.; Lin, K.Y. Effect of Music Tempo on Operating Room Preparation Time. J. Perioper. Pract. 2020, 30, 141–144. [Google Scholar] [CrossRef]
- Janhofer, D.E.; Lakhiani, C.; Chadab, T.M.; Song, D.H. “Alexa, Stop!” Voice-Controlled Devices in the Operating Room. Plast. Reconstr. Surg. 2019, 143, 460e–461e. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Question/Statement: | Surgeon with ANCH | Surgeon without ANCH | Assistant with ANCH | Assistant without ANCH | Nurse with ANCH | Nurse without ANCH | Anaesthesist with ANCH | Anaesthesist without ANCH |
|---|---|---|---|---|---|---|---|---|
| I heard clearly during the case. | 9.0 ± 1.0 | 9.4 ± 0.5 | 7.8 ± 1.1 | 9.2 ± 1.0 | 6.0 ± 1.2 | 9.6 ± 0.5 | 7.8 ± 0.4 | 8.4 ± 0.9 |
| I had to repeat myself because people didn’t understand/hear my message the first time. | 9.0 ± 0.8 | 8.6 ± 0.5 | 9.4 ± 0.9 | 9.4 ± 0.5 | 6.4 ± 1.1 | 8.4 ± 0.5 | 6.8 ± 0.8 | 8.0 ± 0.0 |
| Overall, I felt that OR team communication was? | 8.2 ± 0.4 | 8.4 ± 0.4 | 8.0 ± 0.7 | 7.8 ± 1.1 | 9.2 ± 0.8 | 8.6 ± 0.5 | 8.4 ± 0.5 | 8.2 ± 0.4 |
| I would grade my focus and concentration during this case. | 9.8 ± 0.4 | 9.4 ± 0.5 | 9.4 ± 1.3 | 8.2 ± 1.6 | 9.8 ± 0.4 | 9.0 ± 0.0 | 10.0 ± 0.0 | 8.4 ± 0.9 |
| Steps took longer than necessary because I or others had to repeat/clarify what they were saying. | 8.6 ± 0.6 | 9.0 ± 0.2 | 9.0 ± 0.2 | 9.4 ± 0.5 | 9.4 ± 0.9 | 9.4 ± 0.5 | 9.0 ± 0.0 | 9.2 ± 0.4 |
| Based on the team’s performance during this case, I would feel perfectly safe being treated here. | 9.8 ± 0.4 | 8.6 ± 0.5 | 9.2 ± 1.1 | 9.2 ± 1.1 | 9.8 ± 0.4 | 9.0 ± 0.7 | 9.0 ± 0.0 | 7.2 ± 0.4 |
| How successful were you in performing your task? | 9.8 ± 0.4 | 9.0 ± 0.2 | 9.6 ± 0.9 | 9.0 ± 1.0 | 9.4 ± 0.5 | 9.4 ± 0.5 | 10.0 ± 0.0 | 7.4 ± 0.9 |
| Team morale during this case was high. | 9.4 ± 0.5 | 9.2 ± 0.4 | 10.0 ± 0.0 | 9.4 ± 0.5 | 9.4 ± 0.9 | 7.6 ± 0.5 | 9.0 ± 0.0 | 7.6 ± 0.5 |
| I felt comfortable intervening in this procedure when I had concerns about what was occurring. | 9.4 ± 0.5 | 9.2 ± 0.4 | 9.2 ± 0.4 | 8.4 ± 1.5 | 9.8 ± 0.4 | 8.0 ± 0.1 | 7.2 ± 2.0 | 7.0 ± 0.0 |
| Overall, we worked efficiently as a team. | 9.4 ± 0.5 | 8.0 ± 0.2 | 9.8 ± 0.4 | 8.8 ± 1.1 | 8.8 ± 1.1 | 8.8 ± 1.0 | 9.0 ± 0.2 | 7.8 ± 0.4 |
| I felt fatigued/exhausted after this case. | 8.6 ± 0.5 | 8.4 ± 0.5 | 8.2 ± 0.8 | 8.4 ± 1.5 | 9.6 ± 0.9 | 7.6 ± 0.5 | 10.0 ± 0.0 | 8.6 ± 0.5 |
| I was irritated, stressed, or annoyed during this case. | 8.2 ± 1.1 | 8.4 ± 0.5 | 7.8 ± 0.8 | 8.8 ± 1.1 | 9.4 ± 1.3 | 9.0 ± 0.0 | 9.2 ± 0.8 | 8.6 ± 0.5 |
| How hard did you have to work mentally and physically to accomplish your task? | 7.0 ± 1.6 | 8.8 ± 0.4 | 6.8 ± 1.1 | 6.8 ± 1.3 | 7.2 ± 0.4 | 8.6 ± 0.5 | 8.4 ± 0.5 | 5.6 ± 1.3 |
| I was distracted, annoyed, stressed, or bothered by the noise level in the room. | 7.0 ± 1.6 | 8.8 ± 0.4 | 6.4 ± 1.3 | 7.2 ± 0.8 | 9.6 ± 0.9 | 7.6 ± 0.5 | 8.8 ± 0.8 | 8.8 ± 0.4 |
| Overall Score | 123.3 ± 2.3 | 122.6 ± 1.7 | 120.6 ± 6.3 | 120.0 ± 9.2 | 123.8 ± 5.3 | 120.6 ± 2.3 | 122.6 ± 4.4 | 110.8 ± 3.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stadler, C.; Luger, M.; Schauer, B.; Stevoska, S.; Gotterbarm, T.; Klasan, A. Failed Attempt to Recommend Noise Cancelling Headphones for Knee Arthroplasty Surgeons—Results of a Pilot Study. Medicina 2023, 59, 320. https://doi.org/10.3390/medicina59020320
Stadler C, Luger M, Schauer B, Stevoska S, Gotterbarm T, Klasan A. Failed Attempt to Recommend Noise Cancelling Headphones for Knee Arthroplasty Surgeons—Results of a Pilot Study. Medicina. 2023; 59(2):320. https://doi.org/10.3390/medicina59020320
Chicago/Turabian StyleStadler, Christian, Matthias Luger, Bernhard Schauer, Stella Stevoska, Tobias Gotterbarm, and Antonio Klasan. 2023. "Failed Attempt to Recommend Noise Cancelling Headphones for Knee Arthroplasty Surgeons—Results of a Pilot Study" Medicina 59, no. 2: 320. https://doi.org/10.3390/medicina59020320