
Basosquamous Cell Carcinoma of the Nipple-Areola Complex—Report of a Case
 ,
,  , , , , , and
, , , , , and 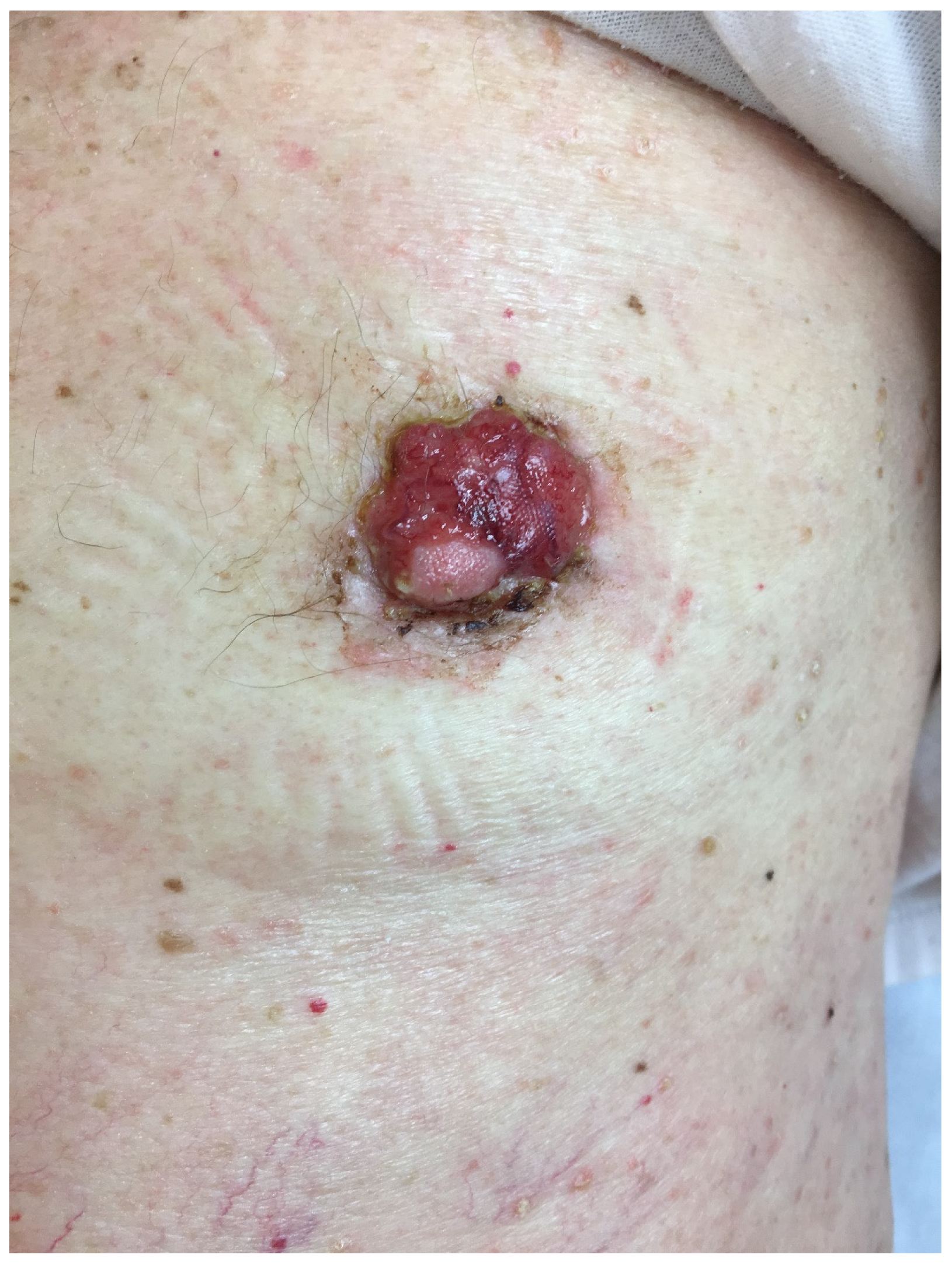{kind=link}
{kind=link}
Abstract
:1. Introduction
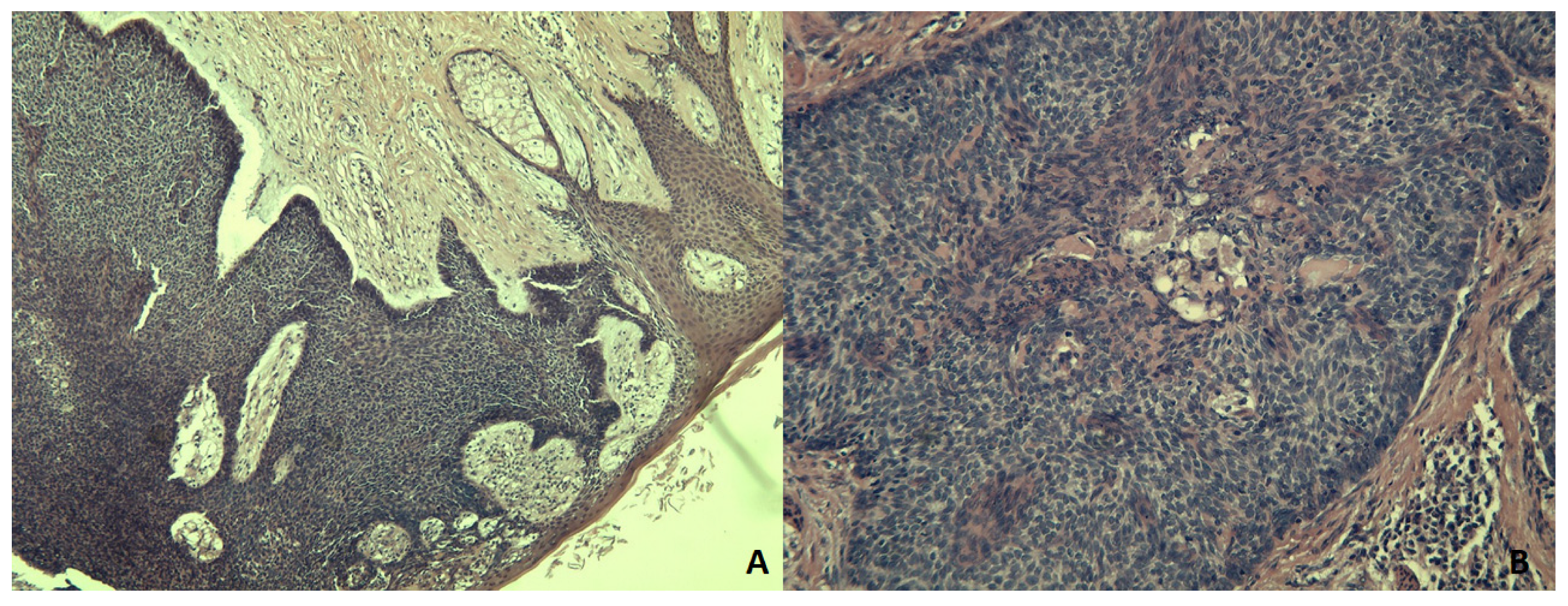
2. Case Presentation and Results
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gandhi, S.A.; Kampp, J. Skin Cancer Epidemiology, Detection, and Management. Med. Clin. N. Am. 2015, 99, 1323–1335. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.; Poletti, E.; Crowson, A.N. Basosquamous carcinoma. J. Am. Acad. Dermatol. 2009, 60, 137–143. [Google Scholar] [CrossRef] [PubMed]
- LeBoit, P.E.; International Agency for Research on Cancer; World Health Organization; International Academy of Pathology; European Organization for Research on Treatment of Cancer; UniversitätsSpital Zürich. Pathology and Genetics of Skin Tumours; IARC Press: Lyon, France, 2006. [Google Scholar]
- Tarallo, M.; Cigna, E.; Frati, R.; Delfino, S.; Innocenzi, D.; Fama, U.; Scuderi, N. Metatypical basal cell carcinoma: A clinical review. J. Exp. Clin. Cancer Res. 2008, 27, 65. [Google Scholar] [CrossRef] [PubMed]
- Rigel, D.S. Cutaneous ultraviolet exposure and its relationship to the development of skin cancer. J. Am. Acad. Dermatol. 2008, 58 (Suppl. S2), S129–S132. [Google Scholar] [CrossRef]
- Narayanan, D.L.; Saladi, R.N.; Fox, J.L. Ultraviolet radiation and skin cancer. Int. J. Dermatol. 2010, 49, 978–986. [Google Scholar] [CrossRef]
- Ouhtit, A.; Nakazawa, H.; Yamasaki, H.; Armstrong, B.K.; Kricker, A.; Tan, E.; English, D.R. UV radiation specific p53 mutation frequency in normal skin as a predictor of risk of basal cell carcinoma. Natl. Cancer Inst. 1998, 90, 523–531. [Google Scholar] [CrossRef]
- Tan, C.Z.; Rieger, K.E.; Sarin, K.Y. Basosquamous carcinoma: Controversy, advances, and future directions. Dermatol. Surg. 2017, 43, 23–31. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE guidelines: Consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, 2013, bcr2013201554. [Google Scholar] [CrossRef]
- Martin, R.C., 2nd; Edwards, M.J.; Cawte, T.G.; Sewell, C.L.; McMasters, K.M. Basosquamous carcinoma: Analysis of prognostic factors influencing recurrence. Cancer 2000, 88, 1365–1369. [Google Scholar] [CrossRef]
- Bowman, P.H.; Ratz, J.L.; Knoepp, T.G.; Barnes, C.J.; Finlay, R.E. Basosquamous carcinoma. Dermatol. Surg. 2003, 29, 830–832. [Google Scholar]
- Wermker, K.; Roknic, N.; Goessling, K.; Klein, M.; Schulze, H.-J.; Hallermann, C. Basosquamous Carcinoma of the Head and Neck: Clinical and Histologic Characteristics and Their Impact on Disease Progression. Neoplasia 2015, 17, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Schuller, D.E.; Berg, J.W.; Sherman, G.; Krause, C.J. Cutaneous Basosquamous Carcinoma of the Head and Neck: A Comparative Analysis. Otolaryngol. Neck Surg. 1979, 87, 420–427. [Google Scholar] [CrossRef]
- Borel, D.M. Cutaneous basosquamous carcinoma. Review of the literature and report of 35 cases. Arch. Pathol. 1973, 95, 293–297. [Google Scholar]
- Leibovitch, I.; Huilgol, S.C.; Selva, D.; Richards, S.; Paver, R. Basosquamous carcinoma: Treatment with Mohs micrographic surgery. Cancer 2005, 104, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.; Desai, S.; Nodzenski, M.; Dubina, M.; Kim, N.; Martini, M.; Fife, D.; Reid, D.; Pirigyi, M.; Poon, E.; et al. Active ascertainment of recurrence rate after treatment of primary basal cell carcinoma (BCC). J. Am. Acad. Dermatol. 2015, 73, 323–325. [Google Scholar] [CrossRef]
- Gallagher, R.P.; Hill, G.B.; Bajdik, C.D.; Fincham, S.; Coldman, A.J.; McLean, D.I.; Threlfall, W.J. Sunlight exposure, pigmentary factors, and risk of nonmelanocytic skin cancer, I: Basal cell carcinoma. Arch. Dermatol. 1995, 131, 157–163. [Google Scholar] [CrossRef]
- Ferguson, M.S.; Nouraei, S.A.; Davies, B.J.; McLean, N.R. Basal cell carcinoma of the nipple-areola complex. Dermatologic surgery. Dermatol. Surg. 2009, 35, 1771–1775. [Google Scholar] [CrossRef]
- The American Cancer Society. Ultraviolet (UV) Radiation. Available online: https://www.cancer.org/healthy/cancer-causes/radiation-exposure/uv-radiation.html (accessed on 10 November 2022).
- Cakir, M.; Tekin, A.; Kücükkartallar, T.; Vatansev, C.; Aksoy, F.; Kartal, A.; Tuncer, F.B. Axillary lymph node status in multicentric breast tumors and breast tumors with nipple involvement. Breast Care 2012, 7, 394–396. [Google Scholar] [CrossRef]
- Yang, J.; Yang, Q.; Mukherjee, A.; Lv, Q. Distance Between the Tumour and Nipple as a Predictor of Axillary Lymph Node Involvement in Breast Cancer. Cancer Manag. Res. 2021, 13, 193–199. [Google Scholar] [CrossRef]
- Ansari, B.; Morton, M.J.; Adamczyk, D.L.; Jones, K.N.; Brodt, J.K.; Degnim, A.C.; Jakub, J.W.; Lohse, C.M.; Boughey, J.C. Distance of breast cancer from the skin and nipple impacts axillary nodal metastases. Ann. Surg. Oncol. 2011, 18, 3174–3180. [Google Scholar] [CrossRef]
- Samain, A.; Boullié, M.C.; Duval-Modeste, A.B.; Joly, P. Cryosurgery and curettage-cryosurgery for basal cell carcinomas of the mid-face. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1291–1296. [Google Scholar] [CrossRef] [PubMed]
- Griffin, L.L.; Lear, J.T. Photodynamic Therapy and Non-Melanoma Skin Cancer. Cancers 2016, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Ulanja, M.B.; Taha, M.E.; Al-Mashhadani, A.A.; Al-Tekreeti, M.M.; Elliot, C.; Ambika, S. Basal Cell Carcinoma of the Female Breast Masquerading as Invasive Primary Breast Carcinoma: An Uncommon Presentation Site. Case Rep. Oncol. Med. 2018, 2018, 5302185. [Google Scholar] [CrossRef] [PubMed]
- Upasham, S.P.; VinodKiri, M.; Sudhamani, S. One more common tumor in an uncommon location: Squamous cell carcinoma on nipple areola complex. Indian J. Cancer 2014, 51, 376–377. [Google Scholar] [CrossRef]
- Wyatt, A.P. Basal cell carcinoma of the male breast. Proc. R. Soc. Med. 1965, 58, 509–510. [Google Scholar] [CrossRef]
- Benharroch, D.; Geffen, D.B.; Peiser, J.; Rosenberg, L. Basal cell carcinoma of the male nipple. Case report and review of the literature. J. Dermatol. Surg. Oncol. 1993, 19, 137–139. [Google Scholar] [CrossRef]
- Kim, J.H.; Oh, J.W.; Shin, D.H.; Kim, S.I.; Park, B.W. Basal cell carcinoma of the nipple-areolar complex. J. Korean Surg. Soc. 2007, 72, 143–146. [Google Scholar]
- Jones, R.; Wayte, D.M.; Mitchell, E.; Beer, W.E. Basal-cell carcinoma of the breast–treatment with retinoids. Clin. Exp. Dermatol. 1991, 16, 448–450. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raimondo, G.; Gallo, G.; D’Onghia, G.; Gabriele, G.; Izzo, L.; Polistena, A.; Esposito, L.; Giancontieri, P.; Macci, L.; D’Andrea, V.; et al. Basosquamous Cell Carcinoma of the Nipple-Areola Complex—Report of a Case. Medicina 2023, 59, 316. https://doi.org/10.3390/medicina59020316
Raimondo G, Gallo G, D’Onghia G, Gabriele G, Izzo L, Polistena A, Esposito L, Giancontieri P, Macci L, D’Andrea V, et al. Basosquamous Cell Carcinoma of the Nipple-Areola Complex—Report of a Case. Medicina. 2023; 59(2):316. https://doi.org/10.3390/medicina59020316
Chicago/Turabian StyleRaimondo, Gabriele, Gaetano Gallo, Giuliano D’Onghia, Giovanni Gabriele, Luciano Izzo, Andrea Polistena, Luca Esposito, Paola Giancontieri, Leonardo Macci, Vito D’Andrea, and et al. 2023. "Basosquamous Cell Carcinoma of the Nipple-Areola Complex—Report of a Case" Medicina 59, no. 2: 316. https://doi.org/10.3390/medicina59020316