

A Combination of Ilizarov Frame, Externalized Locking Plate and Tibia Bridging for an Adult with Large Tibial Defect and Severe Varus Deformity Due to Chronic Osteomyelitis in Childhood: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
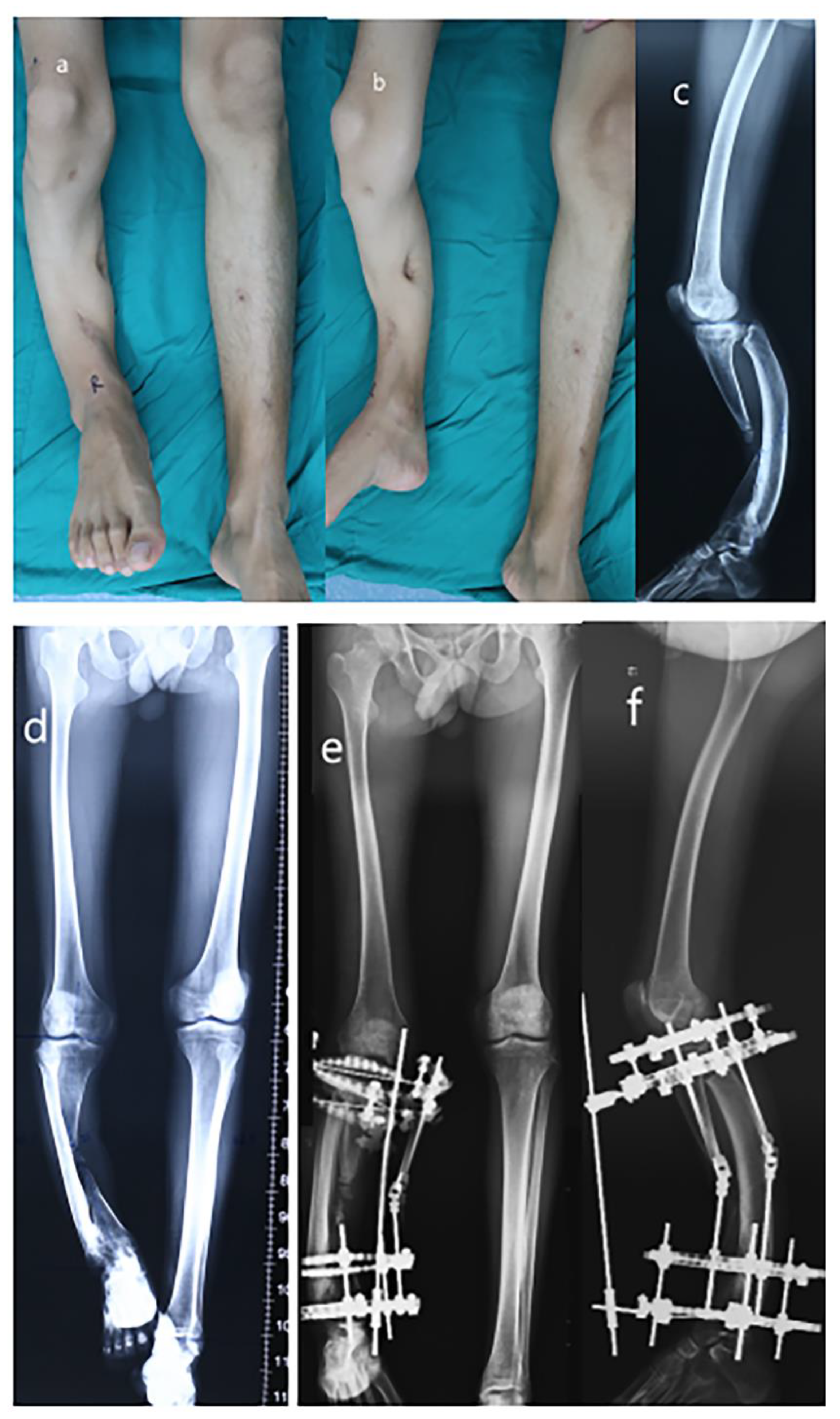
2. Case Presentation
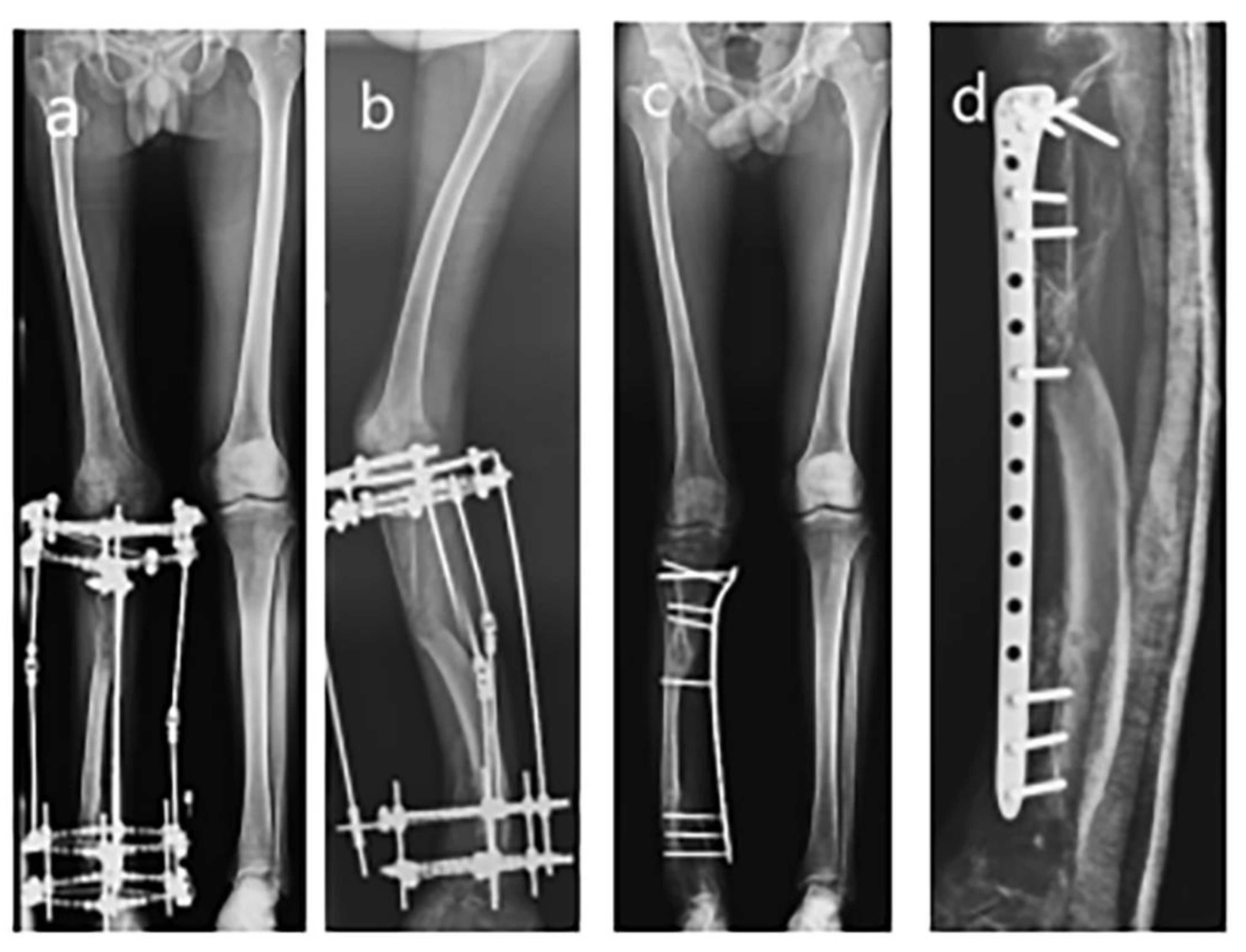
3. Surgical Technique
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ikpeme, I.; Ngim, N.; Ikpeme, A. Diagnosis and treatment of pyogenic bone infections. Afr. Health Sci. 2010, 10, 82–88. [Google Scholar]
- Wirbel, R.; Hermans, K. Surgical treatment of chronic osteomyelitis in children admitted from developing countries. Afr. J. Paediatr. Surg. 2014, 11, 297. [Google Scholar] [CrossRef] [PubMed]
- Koryllou, A.; Mejbri, M.; Theodoropoulou, K.; Hofer, M.; Carlomagno, R. Chronic Nonbacterial Osteomyelitis in Children. Children 2021, 8, 551. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, S.K. Osteomyelitis. Infect. Dis. Clin. N. Am. 2017, 31, 325–338. [Google Scholar] [CrossRef]
- García-Gareta, E.; Coathup, M.J.; Blunn, G.W. Osteoinduction of bone grafting materials for bone repair and regeneration. Bone 2015, 81, 112–121. [Google Scholar] [CrossRef]
- Aktuglu, K.; Erol, K.; Vahabi, A. Ilizarov bone transport and treatment of critical-sized tibial bone defects: A narrative review. J. Orthop. Traumatol. 2019, 20, 22. [Google Scholar] [CrossRef] [Green Version]
- Paley, D. PRECICE intramedullary limb lengthening system. Expert Rev. Med. Devices 2015, 12, 231–249. [Google Scholar] [CrossRef]
- Fenton, C.; Henderson, D.; Samchukov, M.; Cherkashin, A.; Sharma, H. Comparative Stiffness Characteristics of Ilizarov- and Hexapod-type External Frame Constructs. Strateg. Trauma Limb Reconstr. 2021, 16, 138–143. [Google Scholar]
- Henderson, D.J.; Rushbrook, J.L.; Harwood, P.J.; Stewart, T.D. What Are the Biomechanical Properties of the Taylor Spatial Frame™? Clin. Orthop. Relat. Res. 2017, 475, 1472–1482. [Google Scholar] [CrossRef] [Green Version]
- Alford, A.I.; Nicolaou, D.; Hake, M.; McBride-Gagyi, S. Masquelet’s induced membrane technique: Review of current concepts and future directions. J. Orthop. Res. 2021, 39, 707–718. [Google Scholar] [CrossRef]
- Alhadhoud, M.; Alsiri, N.; Alsaffar, M.; Glazebrook, M. Cross-cultural adaptation and validation of an Arabic version of the American Orthopedics Foot and Ankle Score (AOFAS). Foot Ankle Surg. 2020, 26, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Caravelli, S.; Ambrosino, G.; Vocale, E.; Di Ponte, M.; Puccetti, G.; Perisano, C. Custom-Made Implants in Ankle Bone Loss: A Retrospective Assessment of Reconstruction/Arthrodesis in Sequelae of Septic Non-Union of the Tibial Pilon. Medicina 2022, 58, 1641. [Google Scholar] [CrossRef] [PubMed]
- Sailhan, F. Bone lengthening (distraction osteogenesis): A literature review. Osteoporos. Int. 2011, 22, 2011–2015. [Google Scholar] [CrossRef] [PubMed]
- Aiyer, A.A.; Zachwieja, E.C.; Lawrie, C.M.; Kaplan, J.R.M. Management of Isolated Lateral Malleolus Fractures. J. Am. Acad. Orthop. Surg. 2019, 27, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Abulaiti, A.; Liu, Y.; Cai, F.; Ren, P.; Yusufu, A. Risk factors of pin tract infection during bone transport using unilateral external fixator in the treatment of bone defects. BMC Surg. 2021, 21, 377. [Google Scholar] [CrossRef] [PubMed]
- Rogers, L.C.; Bevilacqua, N.J.; Frykberg, R.G.; Armstrong, D.G. Predictors of postoperative complications of Ilizarov external ring fixators in the foot and ankle. J. Foot Ankle Surg. 2007, 46, 372–375. [Google Scholar] [CrossRef]
- Sen, C.; Kocaoglu, M.; Eralp, L.; Gulsen, M.; Cinar, M. Bifocal compression–distraction in the acute treatment of grade III open tibia fractures with bone and soft-tissue loss: A report of 24 cases. J. Orthop. Trauma 2004, 18, 150–157. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Zhong, W.R.; Cheng, L.; Wang, C.Y.; Wen, G.; Han, P.; Chai, Y.M. The Combined Use of a Neurocutaneous Flap and the Ilizarov Technique for Reconstruction of Large Soft Tissue Defects and Bone Loss in the Tibia. Ann. Plast. Surg. 2017, 78, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Sella, E.J. Prevention and management of complications of the Ilizarov treatment method. Foot Ankle Spec. 2008, 1, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Donnan, L.T.; Gomes, B.; Donnan, A.; Harris, C.; Torode, I.; Heidt, C. Ilizarov tibial lengthening in the skeletally immature patient. Bone Jt. J. 2016, 98, 1276–1282. [Google Scholar] [CrossRef]
- Hosny, G.A. Limb lengthening history, evolution, complications and current concepts. J. Orthop. Traumatol. 2020, 21, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebraheim, N.A.; Carroll, T.; Hanna, M.; Zhang, J.; Liu, J. Staged treatment of proximal tibial fracture using external locking compression plate. Orthop. Surg. 2014, 6, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, K.; Dieter, U.; Stachowiak, G.; Gächter, A.; Kuster, M.S. Biomechanical testing of the LCP—How can stability in locked internal fixators be controlled? Injury 2003, 34, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Nanda, R.; Bajwa, A.S.; Candal-Couto, J.; Green, S.; Hui, A.C. Biomechanical testing of the locking compression plate: When does the distance between bone and implant significantly reduce construct stability? Injury 2007, 38, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Kanchanomai, C.; Phiphobmongkol, V. Biomechanical evaluation of fractured tibia externally fixed with an LCP. J. Appl. Biomech. 2012, 28, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Ang, B.F.H.; Chen, J.Y.; Yew, A.K.S.; Chua, S.K.; Chou, S.M.; Chia, S.L.; Koh, J.S.B.; Howe, T.S. How externalised locking compression plate as an alternative to the unilateral external fixator: A biomechanical comparative study of axial and torsional stiffness. Bone Jt. Res. 2017, 6, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Kawoosa, A.A.; Butt, M.F.; Halwai, M.A. Deformity correction and massive lengthening on a centralized fibula with the Ilizarov technique. Acta Orthop. Belg. 2008, 74, 704–708. [Google Scholar]
- Alkenani, N.S.; Alosfoor, M.A.; Al-Araifi, A.K.; Alnuaim, H.A. Ilizarov bone transport after massive tibial trauma: Case report. Int. J. Surg. Case Rep. 2016, 28, 101–106. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, P.; Ding, Y.; Xu, R.; Rai, S.; Liu, R.; Li, J. A Combination of Ilizarov Frame, Externalized Locking Plate and Tibia Bridging for an Adult with Large Tibial Defect and Severe Varus Deformity Due to Chronic Osteomyelitis in Childhood: A Case Report. Medicina 2023, 59, 262. https://doi.org/10.3390/medicina59020262
Hong P, Ding Y, Xu R, Rai S, Liu R, Li J. A Combination of Ilizarov Frame, Externalized Locking Plate and Tibia Bridging for an Adult with Large Tibial Defect and Severe Varus Deformity Due to Chronic Osteomyelitis in Childhood: A Case Report. Medicina. 2023; 59(2):262. https://doi.org/10.3390/medicina59020262
Chicago/Turabian StyleHong, Pan, Yuhong Ding, Ruijing Xu, Saroj Rai, Ruikang Liu, and Jin Li. 2023. "A Combination of Ilizarov Frame, Externalized Locking Plate and Tibia Bridging for an Adult with Large Tibial Defect and Severe Varus Deformity Due to Chronic Osteomyelitis in Childhood: A Case Report" Medicina 59, no. 2: 262. https://doi.org/10.3390/medicina59020262