
Pancreatic Cystic Tumors: A Single-Center Observational Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
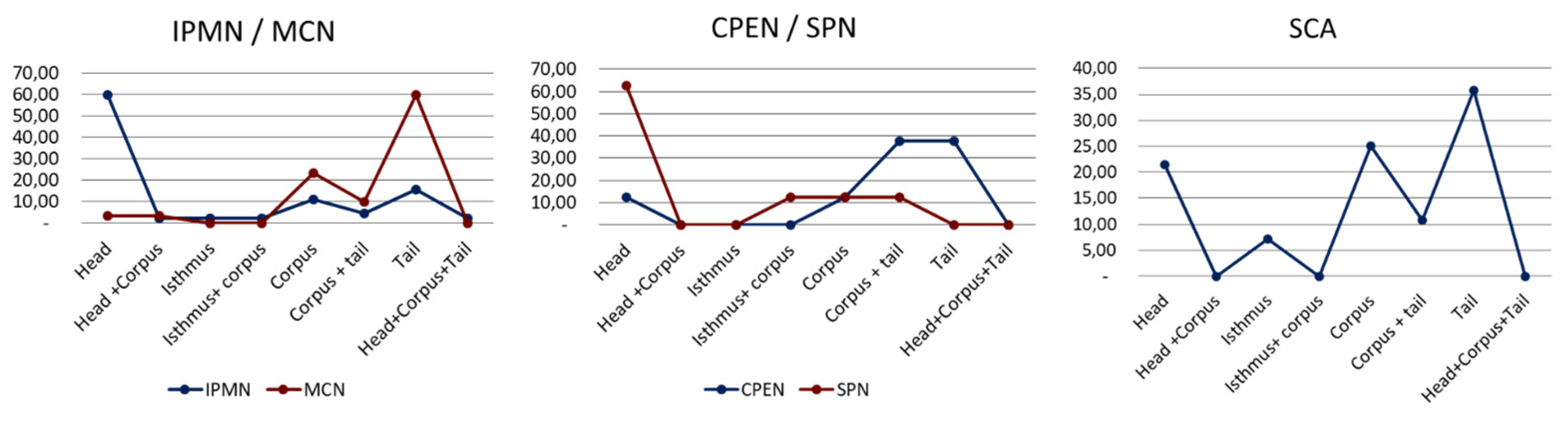
3.1. Characteristics of Pancreatic Cystic Tumors
3.2. Surgical Details and Postoperative Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spence, R.A.; Dasari, B.; Love, M.; Kelly, B.; Taylor, M. Overview of the investigation and management of cystic neoplasms of the pancreas. Dig. Surg. 2011, 28, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.J. Pancreatic Cysts and Guidelines. Dig. Dis. Sci. 2017, 62, 1827–1839. [Google Scholar] [CrossRef]
- Tanaka, M.; Fernández-Del Castillo, C.; Adsay, V.; Chari, S.; Falconi, M.; Jang, J.Y.; Kimura, W.; Levy, P.; Pitman, M.B.; Schmidt, C.M.; et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012, 12, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Vege, S.S.; Ziring, B.; Jain, R.; Moayyedi, P. American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts. Gastroenterology 2015, 148, 819–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.R.; Park, J.K.; Jang, J.Y.; Kwon, W.; Yoon, J.H.; Kim, S.W. Incidental pancreatic cystic neoplasms in an asymptomatic healthy population of 21,745 individuals Large-scale, single-center cohort study. Medicine 2016, 95, e5535. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, S.A.; Attiyeh, M.A.; Seier, K.; Gönen, M.; Schattner, M.; Haviland, D.L.; Balachandran, V.P.; Kingham, T.P.; D’Angelica, M.I.; DeMatteo, R.P.; et al. Should Patients with Cystic Lesions of the Pancreas Undergo Long-term Radiographic Surveillance?: Results of 3024 Patients Evaluated at a Single Institution. Ann. Surg. 2017, 266, 536–544. [Google Scholar] [CrossRef]
- Hasan, A.; Visrodia, K.; Farrell, J.J.; Gonda, T.A. Overview and comparison of guidelines for management of pancreatic cystic neoplasms. World J. Gastroenterol. 2019, 25, 4405–4413. [Google Scholar] [CrossRef]
- Wlaźlak, M.; Oleśna, A.; Danilewicz, M.; Strzelczyk, J. Pancreatic cysts or pancreatic cystic neoplasms? Analysis of 145 cases. Pol. J. Surg. 2018, 90, 22–26. [Google Scholar]
- Jabłońska, B.; Braszczok, L.; Szczęsny-Karczewska, W.; Dubiel-Braszczok, B.; Lampe, P. Surgical treatment of pancreatic cystic tumors. Pol. J. Surg. 2017, 89, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, C.F.; Adsay, N.V. Intraductal papillary mucinous neoplasms of the pancreas. Gastroenterology 2010, 139, 708–713.e2. [Google Scholar] [CrossRef] [PubMed]
- Kohoutova, D.; Zar, S.; Repak, R.; Vlavianos, P.; Bures, J. Pancreatic Cysts: Diagnostic Role of EUS-Guided Microforceps Biopsy and Confocal Laser Endomicroscopy. Gastroenterol. Res. Pract. 2019, 2019, 3431048. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Ahmed, N.; Krishna, S.G. Pancreatic Cystic Lesions: A Focused Review on Cyst Clinicopathological Features and Advanced Diagnostics. Diagnostics 2022, 13, 65. [Google Scholar] [CrossRef] [PubMed]
- Keane, M.G.; Afghani, E. A Review of the Diagnosis and Management of Premalignant Pancreatic Cystic Lesions. J. Clin. Med. 2021, 10, 1284. [Google Scholar] [CrossRef]
- El Gammal, A.T.; Izbicki, J.R. Incidental Intraductal Papillary Mucinous Neoplasm, Cystic or Premalignant Lesions of the Pancreas: The Case for Aggressive Management. Surg. Clin. 2018, 98, 141–155. [Google Scholar] [CrossRef]
- Sugiyama, M.; Atomi, Y. Intraductal papillary mucinous tumors of the pancreas: Imaging studies and treatment strategies. Ann. Surg. 1998, 228, 685–691. [Google Scholar] [CrossRef]
- Basturk, O.; Tan, M.; Bhanot, U.; Allen, P.; Adsay, V.; Scott, S.N.; Shah, R.; Berger, M.F.; Askan, G.; Dikoglu, E.; et al. The oncocytic subtype is genetically distinct from other pancreatic intraductal papillary mucinous neoplasm subtypes. Mod. Pathol. 2016, 29, 1058–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Liu, X.; Zhang, J.; Yang, L. Intraductal Papillary Mucinous Neoplasms of the Pancreas: Correlation of Helical Computed Tomography (CT) Features With Pathologic Findings. Acad Radiol. 2017, 24, 609–614. [Google Scholar] [CrossRef]
- Correa-Gallego, C.; Ferrone, C.R.; Thayer, S.P.; Wargo, J.A.; Warshaw, A.L.; Fernández-Del Castillo, C. Incidental pancreatic cysts: Do we really know what we are watching? Pancreatology 2010, 10, 144–150. [Google Scholar] [CrossRef] [Green Version]
- Cho, C.S.; Russ, A.J.; Loeffler, A.G.; Rettammel, R.J.; Oudheusden, G.; Winslow, E.R.; Weber, S.M. Preoperative classification of pancreatic cystic neoplasms: The clinical significance of diagnostic inaccuracy. Ann. Surg. Oncol. 2013, 20, 3112–3119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvia, R.; Malleo, G.; Marchegiani, G.; Pennacchio, S.; Paiella, S.; Paini, M.; Pea, A.; Butturini, G.; Pederzoli, P.; Bassi, C. Pancreatic resections for cystic neoplasms: From the surgeon’s presumption to the pathologist’s reality. Surgery 2012, 152 (Suppl. 3), S135–S142. [Google Scholar] [CrossRef] [PubMed]
- Jais, B.; Rebours, V.; Malleo, G.; Salvia, R.; Fontana, M.; Maggino, L.; Bassi, C.; Manfredi, R.; Moran, R.; Lennon, A.M.; et al. Serous cystic neoplasm of the pancreas: A multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas). Gut 2016, 65, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Galanis, C.; Zamani, A.; Cameron, J.L.; Campbell, K.A.; Lillemoe, K.D.; Caparrelli, D.; Chang, D.; Hruban, R.H.; Yeo, C.J. Resected Serous Cystic Neoplasms of the Pancreas: A Review of 158 Patients with Recommendations for Treatment. J. Gastrointest. Surg. 2007, 11, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Song, I.H.; An, S.; Kim, S.Y.; Kim, H.J.; Song, K.B.; Hwang, D.W.; Lee, S.S.; Byun, J.H.; Seo, D.W.; et al. Pancreatic serous cystic neoplasms accompanying other pancreatic tumors. Hum. Pathol. 2017, 60, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Strobel, O.; Z’graggen, K.; Schmitz-Winnenthal, F.H.; Friess, H.; Kappeler, A.; Zimmermann, A.; Uhl, W.; Büchler, M.W. Risk of malignancy in serous cystic neoplasms of the pancreas. Digestion 2003, 68, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Compagno, J.; Oertel, J.E. Mucinous cystic neoplasms of the pancreas with overt and latent malignancy (cystadenocarcinoma and cystadenoma). A clinicopathologic study of 41 cases. Am. J. Clin. Pathol. 1978, 69, 573–580. [Google Scholar] [CrossRef]
- Burk, K.S.; Knipp, D.; Sahani, D.V. Cystic Pancreatic Tumors. Magn. Reson. Imaging Clin. 2018, 26, 405–420. [Google Scholar] [CrossRef]
- Scott, J.; Martin, I.; Redhead, D.; Hammond, P.; Garden, O.J. Mucinous cystic neoplasms of the pancreas: Imaging features and diagnostic difficulties. Clin. Radiol. 2000, 55, 187–192. [Google Scholar] [CrossRef]
- Morel, A.; Marteau, V.; Chambon, E.; Gayet, B.; Zins, M. Pancreatic mucinous cystadenoma communicating with the main pancreatic duct on MRI. Br. J. Radiol. 2009, 82, 243–246. [Google Scholar] [CrossRef] [Green Version]
- Modarres, S.R.; Siadati, S.; Momeni, Z. Voluminous pancreatic mucinous cystadenoma in a non-pregnant woman with rheumatoid arthritis. Iran. Red Crescent Med. J. 2011, 13, 595–596. [Google Scholar]
- Goh, B.K.P.; Tan, Y.M.; Chung, Y.F.A.; Chow, P.K.H.; Cheow, P.C.; Wong, W.K.; Ooi, L.L. A review of mucinous cystic neoplasms of the pancreas defined by ovarian-type stroma: Clinicopathological features of 344 patients. World J. Surg. 2006, 30, 2236–2245. [Google Scholar] [CrossRef]
- Yu, P.F.; Hu, Z.A.; Wang, X.B.; Guo, J.M.; Cheng, X.D.; Zhang, Y.L.; Xu, Q. Solid pseudopapillary neoplasm of the pancreas: A review of 553 cases in Chinese literature. World J. Gastroenterol. 2010, 16, 1209–1214. [Google Scholar] [CrossRef]
- Dewhurst, C.E.; Mortele, K.J. Cystic Tumors of the Pancreas: Imaging and Management. Radiol. Clin. N. Am. 2012, 50, 467–486. [Google Scholar] [CrossRef] [PubMed]
- Mulkeen, A.L.; Yoo, P.S.; Cha, C. Less common neoplasms of the pancreas. World J. Gastroenterol. 2006, 12, 3180–3185. [Google Scholar] [CrossRef] [PubMed]
- Geers, C.; Pierre, M.; Jean-François, G.; Birgit, W.; Pierre, D.; Jacques, R.; Christine, S. Solid and pseudopapillary tumor of the pancreas—Review and new insights into pathogenesis. Am. J. Surg. Pathol. 2006, 30, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.P.; Kristensen, T.S.; Storkholm, J.H.; Federspiel, B.H. Solid pseudopapillary neoplasm of the pancreas: Clinical-pathological features and management, a single-center experience. Rare Tumors. 2019, 11, 2036361319878513. [Google Scholar] [CrossRef]
- Shi, S.; Zhou, Y.; Hu, C. Clinical manifestations and multi-slice computed tomography characteristics of solid pseudopapillary neoplasms of the pancreas between males and females. BMC Med. Imaging 2019, 19, 87. [Google Scholar] [CrossRef]
- Nishihara, K.; Nagoshi, M.; Tsuneyoshi, M.; Yamaguchi, K.; Hayashi, I. Papillary cystic tumors of the pancreas assessment of their malignant potential. Cancer 1993, 71, 82–92. [Google Scholar] [CrossRef]
- Tang, L.H.; Aydin, H.; Brennan, M.F.; Klimstra, D.S. Clinically aggressive Solid pseudopapillary neoplasms of the pancreas: A report of two cases with components of undifferentiated carcinoma and a comparative clinicopathologic analysis of 34 conventional cases. Am. J. Surg. Pathol. 2005, 29, 512–519. [Google Scholar] [CrossRef]
- Hurtado-Pardo, L.; Cienfuegos, J.A.; Ruiz-Canela, M.; Panadero, P.; Benito, A.; Hernández-Lizoain, J.L. Cystic pancreatic neuroendocrine tumors (CPENs): A systematic review and meta-analysis of case series. Rev. Española Enferm. Dig. 2017, 109, 778–787. [Google Scholar]
- Anonymous. StatBite: Pancreatic neuroendocrine tumors: Incidence by age and sex. J. Natl. Cancer Inst. 2011, 103, 626. [Google Scholar] [CrossRef]
- Kotoulas, C.; Panayiotides, J.; Antiochos, C.; Sambaziotis, D.; Papadopoulos, G.; Karameris, A. Huge non-functioning pancreatic cystic neuroendocrine tumour: A case report. Eur. J. Surg. Oncol. 1998, 24, 74–76. [Google Scholar] [CrossRef] [PubMed]
- Schindl, M.; Kaczirek, K.; Kaserer, K.; Niederle, B. Is the new classification of neuroendocrine pancreatic tumors of clinical help? World J. Surg. 2000, 24, 1312–1318. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Isayama, H.; Nakai, Y.; Yoshikawa, T.; Ishigaki, K.; Matsubara, S.; Yamamoto, N.; Ijichi, H.; Tateishi, K.; Tada, M.; et al. Prevalence of pancreatic cystic lesions is associated with diabetes mellitus and obesity. Pancreas 2017, 46, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.T.; Tien, Y.W.; Jeng, Y.M.; Yang, C.Y.; Liang, P.C.; Wong, J.M.; Chang, M.C. Overweight Increases the Risk of Malignancy in Patients with Pancreatic Mucinous Cystic Neoplasms. Medicine 2015, 94, e797. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Masuda, A.; Toyama, H.; Shiomi, H.; Zen, Y.; Sofue, K.; Takenaka, M.; Kobayashi, T.; Yagi, Y.; Yamanaka, K.; et al. Smoking Status and the Incidence of Pancreatic Cancer Concomitant with Intraductal Papillary Mucinous Neoplasm. Pancreas 2017, 46, 582–588. [Google Scholar] [CrossRef]
- Shoup, M.; Brennan, M.F.; McWhite, K.; Leung, D.H.Y.; Klimstra, D.; Conlon, K.C. The value of splenic preservation with distal pancreatectomy. Arch. Surg. 2002, 137, 164–168. [Google Scholar] [CrossRef]
- Chaudhari, V.A.; Pradeep, R.; Ramesh, H.; Bhandare, M.S.; Dhar, P.; Pal, S.; Palaniswamy, S.; Jeswanth, S.; Menon, R.N.; Singh, A.N.; et al. Surgery for cystic tumors of pancreas: Report of high-volume, multicenter Indian experience over a decade. Surgery 2019, 166, 1011–1016. [Google Scholar] [CrossRef]
- Valsangkar, N.P.; Morales-Oyarvide, V.; Thayer, S.P.; Ferrone, C.R.; Wargo, J.A.; Warshaw, A.L.; Fernández-del Castillo, C. 851 resected cystic tumors of the pancreas: A 33-year experience at the Massachusetts General Hospital. Surgery 2012, 152 (Suppl. 1), S4–S12. [Google Scholar] [CrossRef] [Green Version]
- Del Chiaro, M.; Segersvärd, R.; Pozzi Mucelli, R.; Rangelova, E.; Kartalis, N.; Ansorge, C.; Arnelo, U.; Blomberg, J.; Löhr, M.; Verbeke, C. Comparison of preoperative conference-based diagnosis with histology of cystic tumors of the pancreas. Ann. Surg. Oncol. 2014, 21, 1539–1544. [Google Scholar] [CrossRef]
- Pancreatic Surgery of Chinese Academic Society of Young Surgeons. The current status of diagnosis and treatment of pancreatic cystic neoplasms in China: A report of 2251 cases. Chin. J. Surg. 2018, 56, 24–29. (In Chinese) [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | n | Median | Lower Quartile | Upper Quartile | Min. | Max. |
|---|---|---|---|---|---|---|
| IPMN | 45 | 66.847 | 62.783 | 70.967 | 40.681 | 79.65 |
| MCN | 30 | 46.714 | 36.755 | 60.64 | 25.228 | 72.353 |
| SCN | 28 | 62.725 | 53.179 | 68.458 | 29.853 | 78.467 |
| CPEN | 8 | 58.542 | 48.676 | 63.847 | 22.839 | 68.331 |
| SPN | 8 | 33.799 | 25.828 | 43.398 | 22.908 | 55.778 |
| Chi-Square Test | Female | Male | p | ||
|---|---|---|---|---|---|
| p(IPMN:MCN) | IPMN 21 | MCN 30 | IPMN 24 | MCN 0 | p < 0.0001 |
| p(IPMN:SCN) | IPMN 21 | SCN 27 | IPMN 24 | SCN 1 | p < 0.0001 |
| p(IPMN:SPN) | IPMN 21 | SPN 8 | IPMN 24 | SPN 0 | 0.00101 |
| p(MCN:CPEN) | MCN 30 | CPEN 5 | MCN 0 | CPEN 3 | 0.00126 |
| p(SCN:CPEN) | SCN 27 | CPEN 5 | SCN 1 | CPEN 3 | 0.0151 |
| p(CPEN:SPN) | CPEN 5 | SPN 8 | CPEN 3 | SPN 0 | 0.0275 |
| Size (cm) | |||||
|---|---|---|---|---|---|
| Type | n | Average | Min. | Max. | Standard Deviation |
| IPMN | 45 | 2.95 | 0.6 | 10 | 1.82 |
| MCN | 30 | 6.78 | 1.5 | 19 | 4.029 |
| SCN | 28 | 4.59 | 1.9 | 11 | 2.621 |
| CPEN | 8 | 3.44 | 1.5 | 9 | 2.628 |
| SPN | 8 | 4.35 | 1.3 | 14 | 4.143 |
| IPMN (n = 45) | MCN (n = 30) | SCA (n = 28) | CPEN (n = 8) | SPN (n = 8) | |
|---|---|---|---|---|---|
| Head | 27 (60%) | 1 (3.33%) | 6 (21.43%) | 1 (12.5%) | 5 (62.5%) |
| Head + corpus | 1 (2.22%) | 1 (3.33%) | 0 | 0 | 0 |
| Isthmus | 1 (2.22%) | 0 | 3 (7.14%) | 0 | 0 |
| Isthmus +corpus | 1 (2.22%) | 0 | 0 | 0 | 1 (12.5%) |
| Corpus | 5 (11.11%) | 7 (23.33%) | 7 (25%) | 1 (12.5%) | 1 (12.5%) |
| Corpus + tail | 2 (4.44%) | 3 (10%) | 3 (10.71%) | 3 (37.5%) | 1 (12.5%) |
| Tail | 7 (15.56%) | 18 (60%) | 10 (35.71%) | 3 (37.5%) | 0 |
| Head + corpus + tail | 1 (2.22%) | 0 | 0 | 0 | 0 |
| PCT Type | ||||||
|---|---|---|---|---|---|---|
| IPMN (n = 45) | MCN (n = 30) | SCN (n = 28) | SPN (n = 8) | CPEN (n = 8) | All | |
| Pancreatoduodenectomy | 20 (44.44%) | 0 | 6 (21.43%) | 4 (50%) | 1 (12.5%) | 31 |
| Traverso | 17 (37.78%) | 0 | 6 (21.43%) | 4 (50%) | 1 (12.5%) | 28 |
| Whipple | 2 (4.44%) | 0 | 0 | 0 | 0 | 2 |
| Clagett | 1 (2.22%) | 0 | 0 | 0 | 0 | 1 |
| Distal pancreatectomy with splenectomy | 3 (6.67%) | 13 (43.33%) | 10 (35.71%) | 0 | 1 (12.5%) | 30 |
| Extended distal pancreatectomy with splenectomy | 2 (4.44%) | 9 (30%) | 7 (25%) | 0 | 4 (50%) | 22 |
| Extended distal pancreatectomy | 6 (13.33%) | 2 (6.67%) | 1 (3.57%) | 1 (12.5%) | 1 (12.5%) | 12 |
| Distal pancreatectomy | 2 (4.44%) | 4 (13.33%) | 1 (3.57%) | 0 | 0 | 7 |
| Total resection | 5 (11.11%) | 0 | 0 | 0 | 0 | 5 |
| Subtotal resection | 4 (8.89%) | 0 | 0 | 0 | 0 | 5 |
| Central pancreatectomy | 1 (2.22%) | 0 | 2 (7.14%) | 2 (25%) | 0 | 5 |
| Enucleation | 0 | 1 (3.33%) | 1 (3.57%) | 0 | 1 (12.5%) | 3 |
| Others | 2 (4.44%) | 1 (3.33%) | 0 | 1 (12.5%) | 0 | 4 |
| Postoperative Complications Following Surgery for Pancreatic Cystic Tumors | ||
|---|---|---|
| Type of Complication | Number of Complications | Types of Surgical Procedures |
| Overall postoperative morbidity | 43 (34.68%) | 25/43 DP 13/43 PD 2/43 CP 2/43 TP 1/43 Enucleation |
| Intra-abdominal fluid collection | 21 (16.94%) | 11/21 DP 6/21 PD 3/21 TP 1 Enucleation |
| Pancreatic postoperative fistula (POPF) | 18 (14.52%) | 15/18 DP 2/18 PD 1/18 CP |
| Biliary fistula | 8 (6.45%) | 5/8 PD 2/8 TP 1/8 DP |
| Acute pancreatitis | 4 (3.2% | 3/4 DP 1/4 CP |
| Wound infection | 5 (4.03%) | 2/5 DP 2/5 PD 1/5 CP |
| Dehiscence of gastrojejunal anastomosis | 1 (0.8%) | 1/1 PD |
| Dehiscence of duodenojejunal anastomosis | 1 (0.8%) | 1/1 PD |
| Intra-abdominal hemorrhage | 1 (0.8%) | 1/1 DP |
| Pulmonary embolism | 1 (0.8%) | 1/1 DP |
| Reoperation rate | 15 (12.1%) | 8/15 DP 4/15 PD 3/15 TP |
| Mortality | 2 (1.61%) | 1/2 CP 1/2 TP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jabłońska, B.; Gudz, A.; Hinborch, T.; Bujała, B.; Biskup, K.; Mrowiec, S. Pancreatic Cystic Tumors: A Single-Center Observational Study. Medicina 2023, 59, 241. https://doi.org/10.3390/medicina59020241
Jabłońska B, Gudz A, Hinborch T, Bujała B, Biskup K, Mrowiec S. Pancreatic Cystic Tumors: A Single-Center Observational Study. Medicina. 2023; 59(2):241. https://doi.org/10.3390/medicina59020241
Chicago/Turabian StyleJabłońska, Beata, Arkadiusz Gudz, Tomasz Hinborch, Bartosz Bujała, Katarzyna Biskup, and Sławomir Mrowiec. 2023. "Pancreatic Cystic Tumors: A Single-Center Observational Study" Medicina 59, no. 2: 241. https://doi.org/10.3390/medicina59020241