
Interstitial Ectopic Pregnancy—Case Reports and Medical Management

Abstract
:1. Introduction
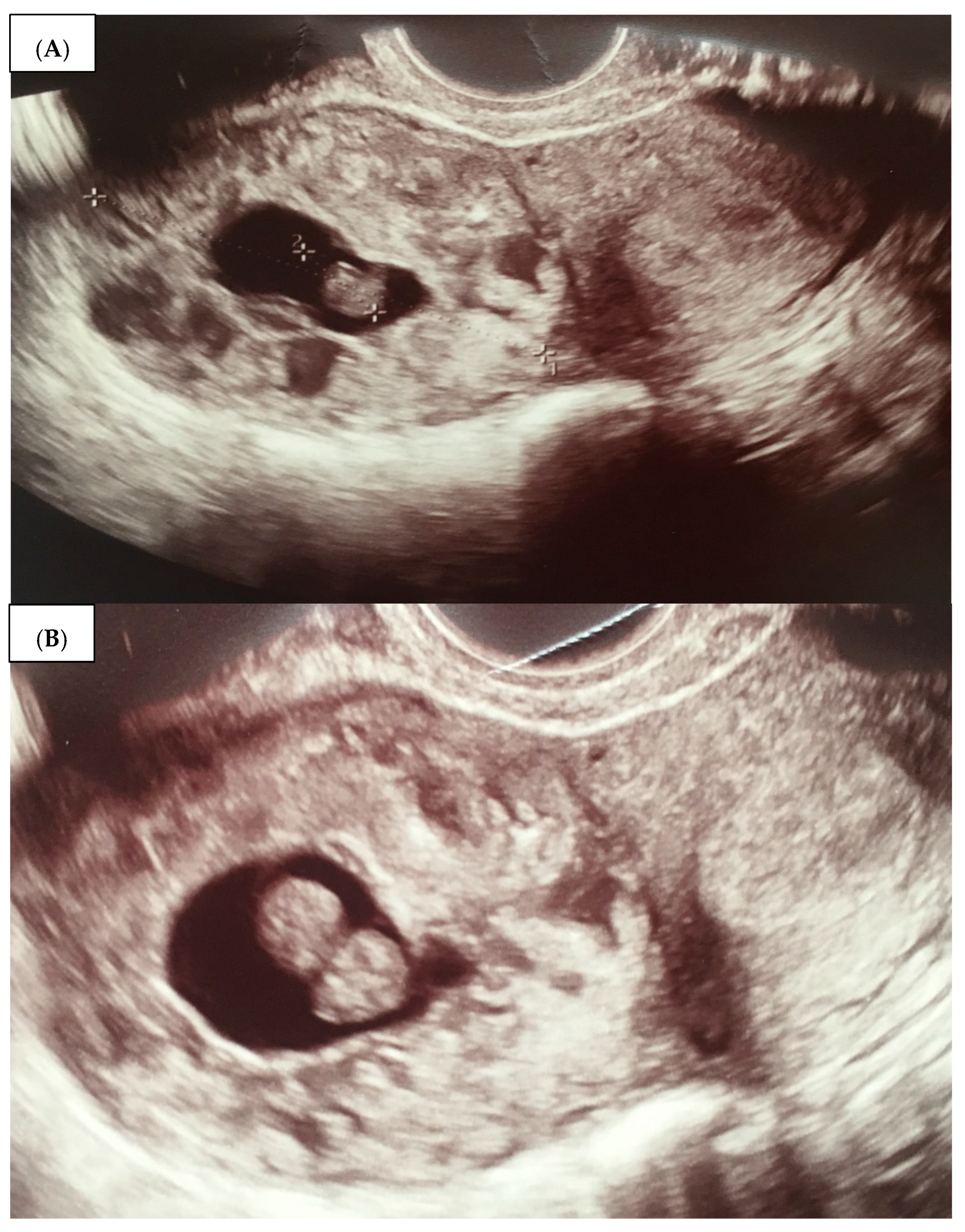
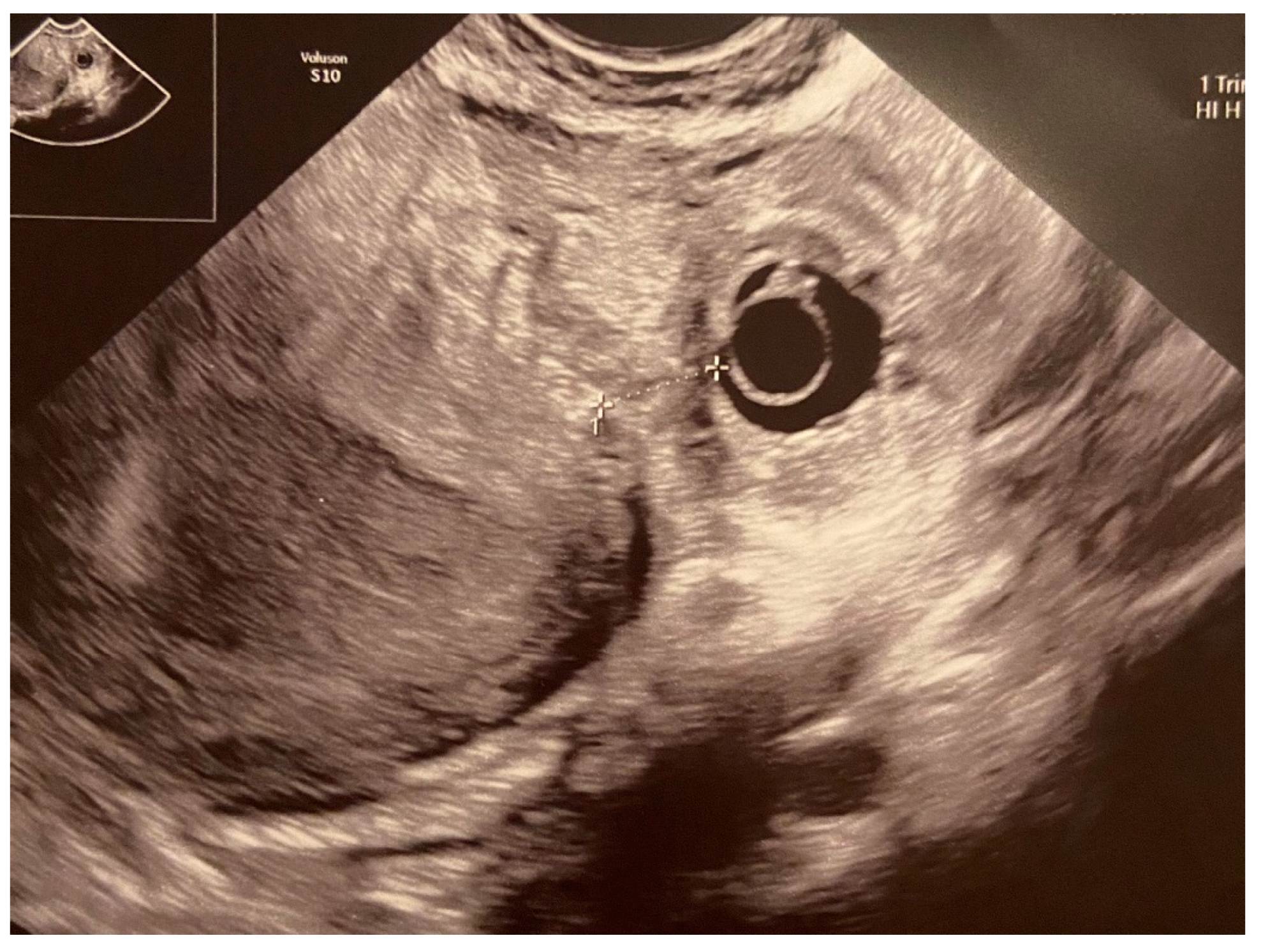
- An empty uterine cavity;
- A chorionic sac located eccentrically and at >1 cm from the lateral edge of the uterine cavity;
- A thin (<5 mm) myometrial layer surrounding the chorionic sac;
- The interstitial line sign;
- No double decidual sac sign, typically seen in the intrauterine pregnancy.
2. Presentation of Case Reports
2.1. Case 1 (Patient A)
2.2. Case 2 (Patient B)
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dagar, M.; Srivastava, M.; Ganguli, I.; Bhardwaj, P.; Sharma, N.; Chwala, D. Interstitial and Cornual Ectopic Pregnancy: Conservative Surgical and Medical Management. J. Obs. Gynaecol. India 2018, 68, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Ilea, C.; Ilie, O.-D.; Marcu, O.-A.; Stoian, I.; Doroftei, B. The Very First Romanian Unruptured 13-Weeks Gestation Tubal Ectopic Pregnancy. Medicina 2022, 58, 1160. [Google Scholar] [CrossRef]
- Stabile, G.; Romano, F.; Zinicola, G.; Topouzova, G.A.; Di Lorenzo, G.; Mangino, F.P.; Ricci, G. Interstitial Ectopic Pregnancy: The Role of Mifepristone in the Medical Treatment. Int. J. Environ. Res. Public Health 2021, 18, 9781. [Google Scholar] [CrossRef]
- Brewer, H.; Gefroh, S.; Bork, M.; Munkarah, A.; Hawkins, R.; Redman, M. Asymptomatic rupture of a cornual ectopic in the third trimester. J. Reprod. Med. 2005, 50, 715–718. [Google Scholar]
- Durand, Y.G.; Capoccia-Brugger, R.; Vial, Y.; Balaya, V. Diagnostic dilemma between angular and interstitial ectopic pregnancy: 3D ultrasound features. J. Ultrasound 2022, 25, 989–994. [Google Scholar] [CrossRef]
- Piecha, D.; Pluta, D.; Pas, P.; Plonka, J.; Kowalczyk, K. Interstitial ectopic pregnancy following ipsilateral salpingectomy. Ginekol. Pol. 2020, 91, 478–479. [Google Scholar] [CrossRef]
- Saichandran, S.; Samal, S. Asymptomatic rupture of cornual gestation presented as abdominal mass. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 2, 746–748. [Google Scholar] [CrossRef] [Green Version]
- Eyvazzadeh, A.D.; Levine, D. Imaging of Pelvic Pain in the First Trimester of Pregnancy. Radiol. Clin. N. Am. 2006, 44, 863–877. [Google Scholar] [CrossRef] [PubMed]
- Hamon, N.G.; Peng, N.G.; Sharon, L. Laparoscopic Treatment of an Interstitial Pregnancy. Gynecol. Obs. 2014, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Brincat, M.; Bryant-Smith, A.; Holland, T.K. The diagnosis and management of interstitial ectopic pregnancies: A review. Gynecol. Surg. 2019, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Chan, L.Y.; Yuen, P.M. Successful treatment of ruptured interstitial pregnancy with laparoscopic surgery. A report of 2 cases. J. Reprod. Med. 2003, 48, 569–571. [Google Scholar] [PubMed]
- Faraj, R.; Steel, M. Management of cornual (interstitial) pregnancy. Obs. Gynaecol. 2007, 9, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Garavaglia, E.; Quaranta, L.; Redaelli, A.; Colombo, G.; Pasi, F.; Candiani, M. Interstitial Pregnancy after In Vitro Fertilization and Embryo Transfer Following Bilateral Salpingectomy: Report of Two Cases and Literature Review. Int. J. Fertil. Steril. 2012, 6, 131–134. [Google Scholar] [PubMed]
- Stabile, G.; Romano, F.; Buonomo, F.; Zinicola, G.; Ricci, G. Conservative Treatment of Interstitial Ectopic Pregnancy with the Combination of Mifepristone and Methotrexate: Our Experience and Review of the Literature. Biomed. Res. Int. 2020, 2020, 8703496. [Google Scholar] [CrossRef]
- Elson, C.J.; Salim, R.; Potdar, N.; Chetty, M.; Ross, J.A.; Kirk, E.J.; on behalf of the Royal College of Obstetricians and Gynaecologists. Diagnosis and management of ectopic pregnancy. BJOG 2016, 123, e15–e55. [Google Scholar]
- Panelli, D.M.; Phillips, C.H.; Brady, P.C. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: A review. Fertil. Res. Pract. 2015, 1, 15. [Google Scholar] [CrossRef] [Green Version]
- Po, L.; Thomas, J.; Mills, K.; Zakhari, A.; Tulandi, T.; Shuman, M.; Page, A. Guideline No. 414: Management of Pregnancy of Unknown Location and Tubal and Nontubal Ectopic Pregnancies. J. Obs. Gynaecol. Can. 2021, 43, 614–630.e1. [Google Scholar] [CrossRef]
- Casadio, P.; Arena, A.; Verrelli, L.; Ambrosio, M.; Fabbri, M.; Giovannico, K.; Magnarelli, G.; Seracchioli, R. Methotrexate injection for interstitial pregnancy: Hysteroscopic conservative mini-invasive approach. Facts Views Vis. Obgyn. 2021, 13, 73–76. [Google Scholar] [CrossRef]
- Santos, L.T.R.; Oliveira, S.C.S.; Rocha, L.G.A.; Sousa, N.D.S.; Figueiredo, R.S. Interstitial Pregnancy: Case Report of Atypical Ectopic Pregnancy. Cureus 2020, 13, e8081. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.; Tulandi, T. Conservative medical and surgical management of interstitial ectopic pregnancy. Fertil. Steril. 1999, 72, 9. [Google Scholar] [CrossRef]
- Mangino, F.P.; Romano, F.; Di Lorenzo, G.; Buonomo, F.; De Santo, D.; Scrimin, F.; Ricci, G. Total hysteroscopic treatment of cervical pregnancy: The 2-step technique. J. Minim. Invasive Gynecol. 2019, 26, 1011–1012. [Google Scholar] [CrossRef] [PubMed]
- Tantchev, L.; Kotzev, A.; Yordanov, A.A. Disturbed interstitial pregnancy: A first case of successful treatment using a mini-laparoscopic approach. Medicina 2019, 55, 215. [Google Scholar] [CrossRef] [Green Version]
- Warda, H.; Mamik, M.M.; Ashraf, M.; Abuzeid, M.I. Interstitial Ectopic Pregnancy: Conservative Surgical Management. J. Soc. Laparoendosc. Surg. 2014, 18, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Moawad, N.S.; Mahajan, S.T.; Moniz, M.H.; Taylor, S.E.; Hurd, W.W. Current diagnosis and treatment of interstitial pregnancy. Am. J. Obstet. Gynecol. 2010, 202, 15–29. [Google Scholar] [CrossRef]
- Moawad, N.S.; Dayaratna, S.; Mahajan, S.T. Mini-cornual excision: A simple stepwise laparoscopic technique for the treatment of cornual pregnancy. J. Soc. Laparoendosc. Surg. 2009, 13, 87–91. [Google Scholar] [CrossRef]
- Bremner, T.; Cela, V.; Luciano, A.A. Surgical management of interstitial pregnancy. J. Am. Assoc. Gynecol. Laparosc. 2000, 7, 387–389. [Google Scholar] [CrossRef]
- Moon, H.S.; Choi, Y.J.; Park, Y.H.; Kim, S.G. New simple endoscopic operations for interstitial pregnancies. Am. J. Obs. Gynecol. 2000, 182, 114–121. [Google Scholar] [CrossRef]
- Gao, M.Y.; Zhu, H.; Zheng, F.Y. Interstitial Pregnancy after Ipsilateral Salpingectomy: Analysis of 46 Cases and a Literature Review. J. Minim. Invasive Gynecol. 2020, 27, 613–617. [Google Scholar] [CrossRef]
- Haestier, A. Guideline for the Medical Management of Ectopic Pregnancy with Methotrexate, Version 5. Norfolk and Norwich University Hospitals. NHS Foundation Trust. Date Approved: 17 July 2020. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiI1euUjJ_7AhVii8MKHertBL4QFnoECAoQAQ&url=https%3A%2F%2Fwww.nnuh.nhs.uk%2Fpublication%2Fdownload%2Fectopic-pregnancy-with-methotrexate-treatment-g27v5%2F&usg=AOvVaw0Kl_UTnnD55Jma5ehZYR_J (accessed on 27 September 2022).
- Tulandi, T.; Al-Jaroudi, D. Interstitial pregnancy: Results generated from the Society of Reproductive Surgeons’ Registry. Obs. Gynecol. 2004, 103, 47–50. [Google Scholar] [CrossRef]
- Alagbe, O.A.; Adeniyi, T.O.; Abayomi, O.A.; Onifade, E.O. Interstitial ectopic pregnancy: A case report. Pan. Afr. Med. J. 2017, 11, 135. [Google Scholar] [CrossRef]
- Katz, D.L.; Barrett, J.P.; Sanfilippo, J.S.; Badway, D.M. Combined hysteroscopy and laparoscopy in the treatment of interstitial pregnancy. Am. J. Obstet. Gynecol. 2003, 188, 1113–1114, ISSN 0002-9378. [Google Scholar] [CrossRef]
- Feng, Q.; Zhong, J.; Liu, Y.; Li, S.T.; Zong, L. Surgical treatment of interstitial pregnancy without cornual resection: A case report. Medicine 2022, 101, e29730. [Google Scholar] [CrossRef]
- Kahramanoglu, I.; Mammadov, Z.; Turan, H.; Urer, A.; Tuten, A. Management options for interstitial ectopic pregnancies: A case series. Pak. J. Med. Sci. 2017, 33, 476–482. [Google Scholar] [CrossRef]
- Marchand, G.; Masoud, A.T.; Sainz, K.; Azadi, A.; Ware, K.; Vallejo, J.; Anderson, S.; King, A.; Osborn, A.; Ruther, S.; et al. A systematic review and meta-analysis of laparotomy compared with laparoscopic management of interstitial pregnancy. Facts Views Vis. Obgyn. 2021, 12, 299–308. [Google Scholar] [PubMed]
- Marchand, G.; Masoud, A.T.; Galitsky, A.; Azadi, A.; Ware, K.; Vallejo, J.; Anderson, S.; King, A.; Ruther, S.; Brazil, G.; et al. Management of interstitial pregnancy in the era of laparoscopy: A meta-analysis of 855 case studies compared with traditional techniques. Obs. Gynecol. Sci. 2021, 64, 156–173. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Date | 31 July | 5 August | 8 August | 9 August | 14 August | 16 August |
|---|---|---|---|---|---|---|
| β-HCG (mIU/mL) | 22,344 | 29,502 | 15,735 | 17,138 | 13,171 | 6463 |
| Date | 8 December | 11 December | 14 December |
|---|---|---|---|
| β-HCG (mIU/mL) | 5632 | 5927 | 5739 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kampioni, M.; Chmaj-Wierzchowska, K.; Wszołek, K.; Wilczak, M. Interstitial Ectopic Pregnancy—Case Reports and Medical Management. Medicina 2023, 59, 233. https://doi.org/10.3390/medicina59020233
Kampioni M, Chmaj-Wierzchowska K, Wszołek K, Wilczak M. Interstitial Ectopic Pregnancy—Case Reports and Medical Management. Medicina. 2023; 59(2):233. https://doi.org/10.3390/medicina59020233
Chicago/Turabian StyleKampioni, Małgorzata, Karolina Chmaj-Wierzchowska, Katarzyna Wszołek, and Maciej Wilczak. 2023. "Interstitial Ectopic Pregnancy—Case Reports and Medical Management" Medicina 59, no. 2: 233. https://doi.org/10.3390/medicina59020233