
Levels of Inflammatory and Bone Metabolic Markers in the Gingival Crevicular Fluid of Individuals Undergoing Fixed Orthodontic Treatment in Comparison to Those Utilizing Invisalign

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Participants
2.2. Sample Size and Allocation of the Patients
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Periodontal Parameter Monitoring
2.6. Measuring and Collecting GCF
2.7. Analysis of Cytokines Using ELISA (Enzyme-Linked Immunosorbent Assay)
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonato, R.C.S.; Mapengo, M.A.A.; De Azevedo-Silva, L.J.; Janson, G.; De Carvalho Sales-Peres, S.H. Tooth Movement, Orofacial Pain, and Leptin, Interleukin-1β, and Tumor Necrosis Factor-α Levels in Obese Adolescents. Angle Orthod. 2022, 92, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C.C. Orthodontic Tooth Movement: The Biology and Clinical Implications. Kaohsiung J. Med. Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Dilsiz, A.; Kiliç, N.; Aydin, T.; Nesibe Ates, F.; Zihni, M.; Bulut, C. Leptin Levels in Gingival Crevicular Fluid during Orthodontic Tooth Movement. Angle Orthod. 2010, 80, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Reda, R.; Zanza, A.; Miccoli, G.; Di Nardo, D.; Testarelli, L. Can Peri-Implant Marginal Bone Loss Progression and a-MMP-8 Be Considered Indicators of the Subsequent Onset of Peri-Implantitis? A 5-Year Study. Diagnostics 2022, 12, 2599. [Google Scholar] [CrossRef] [PubMed]
- Vujacic, A.; Pavlovic, J.; Konic-Ristic, A. The Role of Cytokines in Orthodontic Tooth Movement. In Current Approaches in Orthodontics; IntechOpen: London, UK, 2019; ISBN 978-1-78985-182-3. [Google Scholar]
- Chen, Y.; Zhang, C. Role of Noncoding RNAs in Orthodontic Tooth Movement: New Insights into Periodontium Remodeling. J. Transl. Med. 2023, 21, 101. [Google Scholar] [CrossRef]
- Huang, H.; Williams, R.C.; Kyrkanides, S. Accelerated Orthodontic Tooth Movement: Molecular Mechanisms. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 620–632. [Google Scholar] [CrossRef]
- Alfano, M.C. The Origin of Gingival Fluid. J. Theor. Biol. 1974, 47, 127–136. [Google Scholar] [CrossRef]
- Khurshid, Z.; Mali, M.; Naseem, M.; Najeeb, S.; Zafar, M.S. Human Gingival Crevicular Fluids (GCF) Proteomics: An Overview. Dent. J. 2017, 5, 12. [Google Scholar] [CrossRef]
- Chelărescu, S.; Șurlin, P.; Decusară, M.; Oprică, M.; Bud, E.; Teodorescu, E.; Elsaafin, M.N.; Păcurar, M. Evaluation of IL1β and IL6 Gingival Crevicular Fluid Levels during the Early Phase of Orthodontic Tooth Movement in Adolescents and Young Adults. Appl. Sci. 2021, 11, 521. [Google Scholar] [CrossRef]
- Kunii, R.; Yamaguchi, M.; Tanimoto, Y.; Asano, M.; Yamada, K.; Goseki, T.; Kasai, K. Role of Interleukin-6 in Orthodontically Induced Inflammatory Root Resorption in Humans. Korean J. Orthod. 2013, 43, 294–301. [Google Scholar] [CrossRef]
- Kamran, M.A.; Alnazeh, A.A.; Almagbol, M.; Almoammar, S.; Alhaizaey, A.H.A.; Alshahrani, I. Role of Six Cytokines and Bone Metabolism Biomarkers in Gingival Crevicular Fluid in Patients Undergoing Fixed Orthodontic Appliance Treatment in Comparison with Aligners: A Clinical Study. Angle Orthod. 2023, 93, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.F.; Willershausen, B. Braces versus Invisalign®: Gingival Parameters and Patients’ Satisfaction during Treatment: A Cross-Sectional Study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Chami, V.O.; Nunes, L.; Capelli Júnior, J. Expression of Cytokines in Gingival Crevicular Fluid Associated with Tooth Movement Induced by Aligners: A Pilot Study. Dental Press J. Orthod. 2018, 23, 41–46. [Google Scholar] [CrossRef]
- Krishnan, V.; Davidovitch, Z. Cellular, Molecular, and Tissue-Level Reactions to Orthodontic Force. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 469.e1-32. [Google Scholar] [CrossRef] [PubMed]
- Castroflorio, T.; Gamerro, E.F.; Caviglia, G.P.; Deregibus, A. Biochemical Markers of Bone Metabolism during Early Orthodontic Tooth Movement with Aligners. Angle Orthod. 2017, 87, 74–81. [Google Scholar] [CrossRef]
- Barbieri, G.; Solano, P.; Alarcón, J.A.; Vernal, R.; Rios-Lugo, J.; Sanz, M.; Martín, C. Biochemical Markers of Bone Metabolism in Gingival Crevicular Fluid during Early Orthodontic Tooth Movement. Angle Orthod. 2013, 83, 63–69. [Google Scholar] [CrossRef]
- Goodyear, M.D.E.; Krleza-Jeric, K.; Lemmens, T. The Declaration of Helsinki. Br. Med. J. 2007, 335, 624–625. [Google Scholar] [CrossRef]
- Shimizu, M.; Yamaguchi, M.; Fujita, S.; Utsunomiya, T.; Yamamoto, H.; Kasai, K. Interleukin-17/T-Helper 17 Cells in an Atopic Dermatitis Mouse Model Aggravate Orthodontic Root Resorption in Dental Pulp. Eur. J. Oral Sci. 2013, 121, 101–110. [Google Scholar] [CrossRef]
- Alhadlaq, A.M. Biomarkers of Orthodontic Tooth Movement in Gingival Crevicular Fluid: A Systematic Review. J. Contemp. Dent. Pract. 2015, 16, 578–587. [Google Scholar] [CrossRef]
- Perinetti, G.; Primožič, J.; Castaldo, A.; Di Lenarda, R.; Contardo, L. Is Gingival Crevicular Fluid Volume Sensitive to Orthodontic Tooth Movement? A Systematic Review of Split-Mouth Longitudinal Studies. Orthod. Craniofacial Res. 2013, 16, 1–19. [Google Scholar] [CrossRef]
- Başaran, G.; Özer, T.; Kaya, F.A.; Hamamci, O. Interleukins 2, 6, and 8 Levels in Human Gingival Sulcus during Orthodontic Treatment. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 7.e1–7.e6. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Vissink, A. Cytokines in Crevicular Fluid and Orthodontic Tooth Movement. Eur. J. Oral Sci. 2008, 116, 89–97. [Google Scholar] [CrossRef]
- Bletsa, A.; Berggreen, E.; Brudvik, P. Interleukin-1α and Tumor Necrosis Factor-α Expression during the Early Phases of Orthodontic Tooth Movement in Rats. Eur. J. Oral Sci. 2006, 114, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Allgayer, S.; Macedo de Menezes, L.; Batista, E.L. Interleukin 17 (IL-17) and Interleukin 23 (IL-23) Levels Are Modulated by Compressive Orthodontic Forces in Humans. J. World Fed. Orthod. 2019, 8, 148–152. [Google Scholar] [CrossRef]
- Nunes, L.; Quintanilha, L.; Perinetti, G.; Capelli, J. Effect of Orthodontic Force on Expression Levels of Ten Cytokines in Gingival Crevicular Fluid. Arch. Oral Biol. 2017, 76, 70–75. [Google Scholar] [CrossRef]
- Van Gastel, J.; Teughels, W.; Quirynen, M.; Struyf, S.; Van Damme, J.; Coucke, W.; Carels, C. Longitudinal Changes in Gingival Crevicular Fluid after Placement of Fixed Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 735–744. [Google Scholar] [CrossRef]
- Almeida, R.C.; Capelli, J.; Teles, R.P. Levels of Gingival Crevicular Fluid Matrix Metalloproteinases in Periodontally Compromised Teeth under Orthodontic Forces. Angle Orthod. 2015, 85, 1009–1014. [Google Scholar] [CrossRef]
- Gujar, A.N.; Baeshen, H.A.; Alhazmi, A.; Bhandi, S.; Raj, A.T.; Patil, S.; Birkhed, D. Cytokine Levels in Gingival Crevicular Fluid during Orthodontic Treatment with Aligners Compared to Conventional Labial Fixed Appliances: A 3-Week Clinical Study. Acta Odontol. Scand. 2019, 77, 474–481. [Google Scholar] [CrossRef]
- Alfaqeeh, S.A.; Anil, S. Osteocalcin and N-Telopeptides of Type i Collagen Marker Levels in Gingival Crevicular Fluid during Different Stages of Orthodontic Tooth Movement. Am. J. Orthod. Dentofac. Orthop. 2011, 139, e553–e559. [Google Scholar] [CrossRef]
- Griffiths, G.S.; Moulson, A.M.; Petrie, A.; James, I.T. Evaluation of Osteocalcin and Pyridinium Crosslinks of Bone Collagen as Markers of Bone Turnover in Gingival Crevicular Fluid during Different Stages of Orthodontic Treatment. J. Clin. Periodontol. 1998, 25, 492–498. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
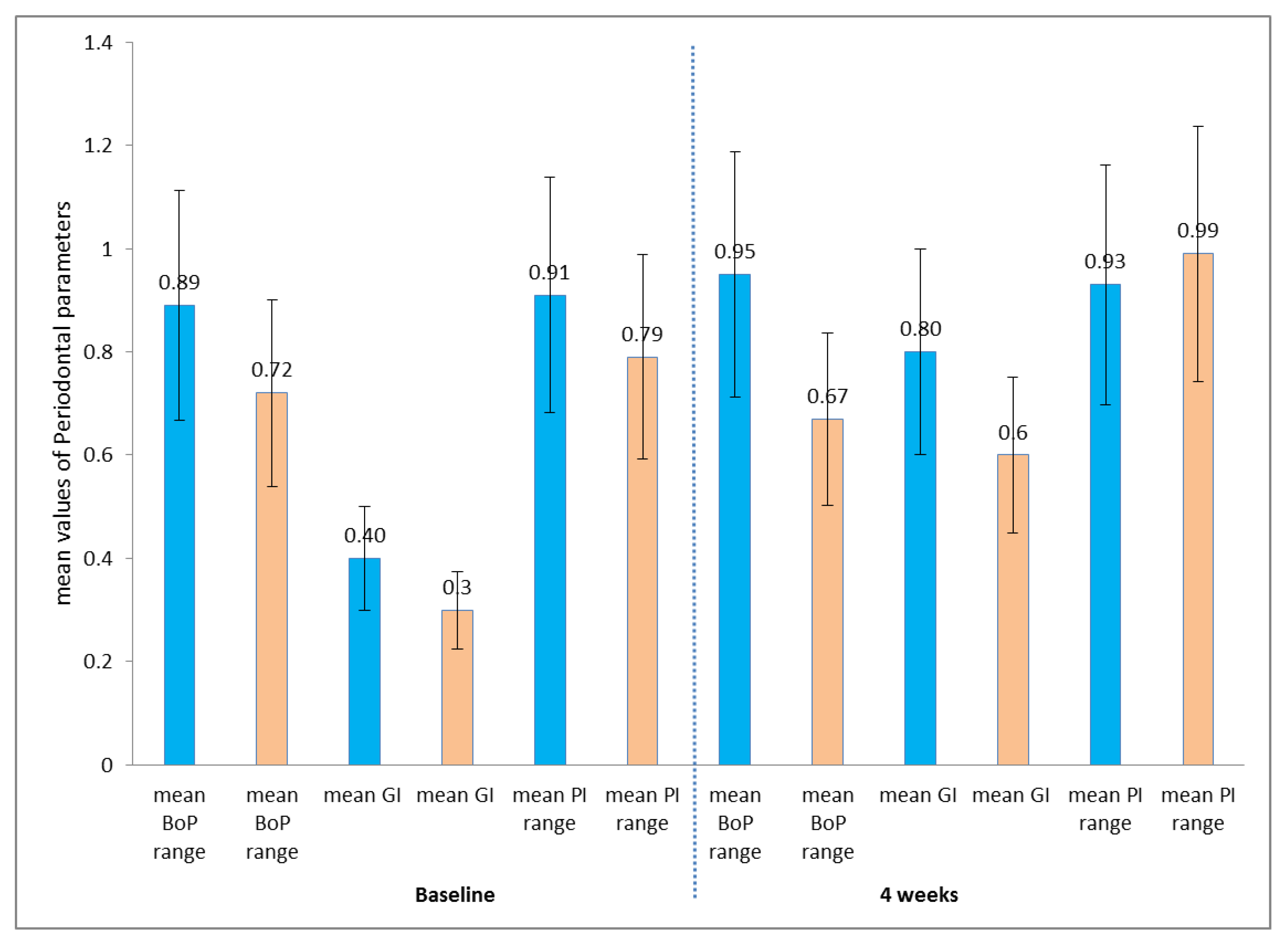
| Periodontal Parameters | Baseline N = 30 Each | 4 Weeks N = 30 Each | p-Value | ||
|---|---|---|---|---|---|
| FOT | Invisalign | FOT | Invisalign | ||
| Mean BoP range | 0.89 (0.3–1.2) | 0.72(0.3–0.9) | 0.95 (0.4–1.1) | 0.67 (0.2–0.6) | 0.312 |
| Mean GI | 0.4 (0.2–1.0) | 0.3 (0.3–0.8) | 0.8 (0.3–1.0) | 0.6 (0.2–0.4) | 0.574 |
| Mean PI range | 0.91 (0.4–1.3) | 0.79 (0.52–1.3) | 0.93 (0.6–1.4) | 0.99 (0.4–1.1) | 0.215 |
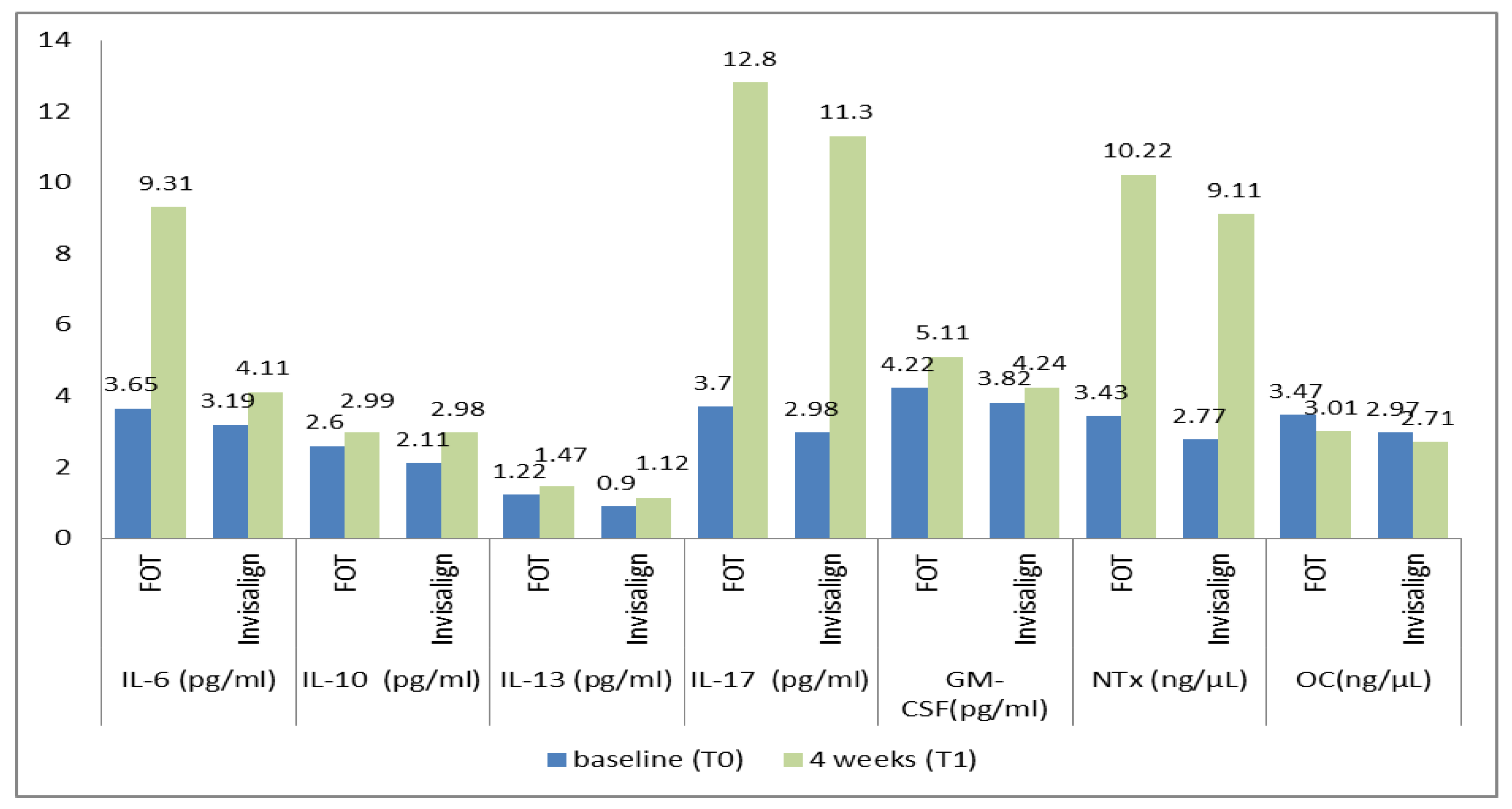
| Biomarkers in GCF | Groups | Mean ± SD Baseline (T0) | Mean ± SD 4 Weeks (T1) | p-Value |
|---|---|---|---|---|
| IL-6 (pg/mL) | FOT | 3.65 ± 1.21 | 9.31 ± 1.47 * | 0.014 |
| Invisalign | 3.19 ± 0.42 | 4.11 ± 0.33 * | 0.024 | |
| IL-10 (pg/mL) | FOT | 2.6 ± 0.42 | 2.99 ± 0.61 | 0.028 |
| Invisalign | 2.11 ± 0.21 | 2.98 ± 1.01 | 0.025 | |
| IL-13 (pg/mL) | FOT | 1.22 ± 0.11 | 1.47 ± 0.15 | 0.026 |
| Invisalign | 0.9 ± 0.04 | 1.12 ± 0.11 | 0.025 | |
| IL-17 (pg/mL) | FOT | 3.7 ± 1.23 | 12.8 ± 1.55 | 0.011 |
| Invisalign | 2.98 ± 1.01 | 11.3 ± 1.23 | 0.017 | |
| GM-CSF (pg/mL) | FOT | 4.22 ± 0.9 | 5.11 ± 1.41 | 0.024 |
| Invisalign | 3.82 ± 0.7 | 4.24 ± 1.21 | 0.026 | |
| NTx (ng/µL) | FOT | 3.43 ± 0.11 | 10.22 ± 0.15 * | 0.017 |
| Invisalign | 2.77 ± 0.8 | 9.11 ± 1.00 * | 0.019 | |
| OC (ng/µL) | FOT | 3.47 ± 0.34 | 3.01 ± 0.29 | 0.025 |
| Invisalign | 2.97 ± 0.21 | 2.71 ± 0. 11 | 0.023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnazeh, A.A.; Kamran, M.A.; Aseeri, Y.; Alrwuili, M.R.; Aljabab, M.A.; Baig, E.A.; Hameed, M.S. Levels of Inflammatory and Bone Metabolic Markers in the Gingival Crevicular Fluid of Individuals Undergoing Fixed Orthodontic Treatment in Comparison to Those Utilizing Invisalign. Medicina 2023, 59, 2107. https://doi.org/10.3390/medicina59122107
Alnazeh AA, Kamran MA, Aseeri Y, Alrwuili MR, Aljabab MA, Baig EA, Hameed MS. Levels of Inflammatory and Bone Metabolic Markers in the Gingival Crevicular Fluid of Individuals Undergoing Fixed Orthodontic Treatment in Comparison to Those Utilizing Invisalign. Medicina. 2023; 59(12):2107. https://doi.org/10.3390/medicina59122107
Chicago/Turabian StyleAlnazeh, Abdullah A., Muhammad Abdullah Kamran, Yahya Aseeri, Mohammad Raji Alrwuili, Mohammed Ahmed Aljabab, Eisha Abrar Baig, and Mohammad Shahul Hameed. 2023. "Levels of Inflammatory and Bone Metabolic Markers in the Gingival Crevicular Fluid of Individuals Undergoing Fixed Orthodontic Treatment in Comparison to Those Utilizing Invisalign" Medicina 59, no. 12: 2107. https://doi.org/10.3390/medicina59122107