
Impact of Syndesmotic Screw Removal on Quality of Life, Mobility, and Daily Living Activities in Patients Post Distal Tibiofibular Diastasis Repair
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Participant Selection and Sample Collection
2.3. Data Acquisition and Surveys
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Literature Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yuen, C.P.; Lui, T.H. Distal Tibiofibular Syndesmosis: Anatomy, Biomechanics, Injury and Management. Open Orthop. J. 2017, 11, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Carto, C.; Lezak, B.; Varacallo, M. Anatomy, Bony Pelvis and Lower Limb: Distal Tibiofibular Joint (Tibiofibular Syndesmosis). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK547655/ (accessed on 8 August 2023).
- Pogliacomi, F.; De Filippo, M.; Casalini, D.; Longhi, A.; Tacci, F.; Perotta, R.; Pagnini, F.; Tocco, S.; Ceccarelli, F. Acute syndesmotic injuries in ankle fractures: From diagnosis to treatment and current concepts. World J. Orthop. 2021, 12, 270–291. [Google Scholar] [CrossRef] [PubMed]
- Hunt, K.J. Syndesmosis injuries. Curr. Rev. Musculoskelet. Med. 2013, 6, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Magan, A.; Golano, P.; Maffulli, N.; Khanduja, V. Evaluation and management of injuries of the tibiofibular syndesmosis. Br. Med. Bull. 2014, 111, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.-M.; Zhang, Y.-W.; Hu, S.-Y.; Rui, Y.-F. A systematic review of ankle fracture-dislocations: Recent update and future prospects. Front. Surg. 2022, 9, 965814. [Google Scholar] [CrossRef]
- Yawar, B.; Hanratty, B.; Asim, A.; Niazi, A.K.; Khan, A.M. Suture-Button Versus Syndesmotic Screw Fixation of Ankle Fractures: A Comparative Retrospective Review Over One Year. Cureus 2021, 13, e17826. [Google Scholar] [CrossRef]
- Corte-Real, N.; Caetano, J. Ankle and syndesmosis instability: Consensus and controversies. EFORT Open Rev. 2021, 6, 420–431. [Google Scholar] [CrossRef]
- Baxter, S.; Farris, E.; Johnson, A.H.; Brennan, J.C.; Friedmann, E.M.; Turcotte, J.J.; Keblish, D.J. Transosseous Fixation of the Distal Tibiofibular Syndesmosis: Comparison of Interosseous Suture and Endobutton Across Age Groups. Cureus 2023, 15, e40355. [Google Scholar] [CrossRef]
- Sipahioglu, S.; Zehir, S.; Isikan, U.E. Syndesmotic screw fixation in tibiofibular diastasis. Niger. J. Clin. Pr. 2018, 21, 692–697. [Google Scholar] [CrossRef]
- Kapadia, B.H.; Sabarese, M.J.; Chatterjee, D.; Aylyarov, A.; Zuchelli, D.M.; Hariri, O.K.; Uribe, J.A.; Tsai, J. Evaluating success rate and comparing complications of operative techniques used to treat chronic syndesmosis injuries. J. Orthop. 2020, 22, 225–230. [Google Scholar] [CrossRef]
- Walley, K.C.; Hofmann, K.J.; Velasco, B.T.; Kwon, J.Y. Removal of Hardware After Syndesmotic Screw Fixation: A Systematic Literature Review. Foot Ankle Spéc. 2017, 10, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Schepers, T. To retain or remove the syndesmotic screw: A review of literature. Arch. Orthop. Trauma Surg. 2011, 131, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Ijezie, N.; Fraig, H.; Abolaji, S. Outcomes of the Routine Removal of the Syndesmotic Screw. Cureus 2022, 14, e26675. [Google Scholar] [CrossRef] [PubMed]
- Zeng, M.; Xu, Z.; Song, Z.Q.; Li, J.X.; Tang, Z.W.; Xiao, S.; Wen, J. Diagnosis and treatment of chronic osteomyelitis based on nanomaterials. World J. Orthop. 2023, 14, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef]
- Moon, Y.J.; Kim, D.H.; Lee, K.B. Is it necessary to remove syndesmotic screw before weight-bearing ambulation? Medicine 2020, 99, e19436. [Google Scholar] [CrossRef]
- Schnetzke, M.; Vetter, S.Y.; Beisemann, N.; Swartman, B.; Grützner, P.A.; Franke, J. Management of syndesmotic injuries: What is the evidence? World J. Orthop. 2016, 7, 718–725. [Google Scholar] [CrossRef]
- Kujanpää, T.; Jokelainen, J.; Auvinen, J.; Timonen, M. Generalised anxiety disorder symptoms and utilisation of health care services. A cross-sectional study from the “Northern Finland 1966 Birth Cohort”. Scand. J. Prim. Health Care 2016, 34, 151–158. [Google Scholar] [CrossRef]
- Mao, W.; Shalaby, R.; Agyapong, V.I.O. Interventions to Reduce Repeat Presentations to Hospital Emergency Departments for Mental Health Concerns: A Scoping Review of the Literature. Healthcare 2023, 11, 1161. [Google Scholar] [CrossRef]
- Buccino, F.; Bunt, A.; Lazell, A.; Vergani, L.M. Mechanical Design Optimization of Prosthetic Hand’s Fingers: Novel Solutions towards Weight Reduction. Materials 2022, 15, 2456. [Google Scholar] [CrossRef]
- Buccino, F.; Martinoia, G.; Vergani, L.M. Torsion—Resistant Structures: A Nature Addressed Solution. Materials 2021, 14, 5368. [Google Scholar] [CrossRef]
- Millstein, S.G.; Heger, H.; Hunter, G. Prosthetic Use in Adult Upper Limb Amputees: A Comparison of the Body Powered and Electrically Powered Prostheses. Prosthet. Orthot. Int. 1986, 10, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Hosin, S.; Vermesan, D.; Prejbeanu, R.; Crisan, D.; Al-Qatawneh, M.; Pop, D.; Mioc, M.; Bratosin, F.; Feciche, B.; Hemaswini, K.; et al. Avoiding the Removal of Syndesmotic Screws after Distal Tibiofibular Diastasis Repair: A Benefit or a Drawback? J. Clin. Med. 2022, 11, 6412. [Google Scholar] [CrossRef] [PubMed]
- Bragg, J.T.; Masood, R.M.; Spence, S.S.; Citron, J.E.; Moon, A.S.; Salzler, M.J.; Ryan, S.P. Predictors of Hardware Removal in Orthopaedic Trauma Patients Undergoing Syndesmotic Ankle Fixation with Screws. Foot Ankle Orthop. 2023, 8, 24730114231198841. [Google Scholar] [CrossRef] [PubMed]
- Desouky, O.; Elseby, A.; Ghalab, A.H. Removal of Syndesmotic Screw After Fixation in Ankle Fractures: A Systematic Review. Cureus 2021, 13, e15435. [Google Scholar] [CrossRef] [PubMed]
- Steindel, S.J. International classification of diseases, 10th edition, clinical modification and procedure coding system: Descriptive overview of the next generation HIPAA code sets. J. Am. Med. Inform. Assoc. 2010, 17, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, L.L.D.; Nunes, I.G.; Nogueira, R.R.; Martins, G.E.V.; Mesencio, A.C.; Kobata, S.I. Reproducibility of the Lauge-Hansen, Danis-Weber, and AO classifications for ankle fractures. Rev. Bras. De Ortop. 2017, 53, 101–106. [Google Scholar] [CrossRef]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef]
- Snaith, R.P. The Hospital Anxiety And Depression Scale. Health Qual. Life Outcomes 2003, 1, 29. [Google Scholar] [CrossRef]
- Vahedi, S. World Health Organization Quality-of-Life Scale (WHOQOL-BREF): Analyses of Their Item Response Theory Properties Based on the Graded Responses Model. Iran. J. Psychiatry 2010, 5, 140–153. [Google Scholar]
- Huang, C.T.; Huang, P.J.; Lu, C.C.; Shih, C.L.; Cheng, Y.M.; Chen, S.J. Syndesmosis Changes before and after Syndesmotic Screw Removal: A Retrospective Radiographic Study. Medicina 2022, 58, 445. [Google Scholar] [CrossRef]
- Pogliacomi, F.; Artoni, C.; Riccoboni, S.; Calderazzi, F.; Vaienti, E.; Ceccarelli, F. The management of syndesmotic screw in ankle fractures. Acta Biomed. 2018, 90, 146–149. [Google Scholar] [CrossRef]
- Kim, J.; Kwon, M.; Day, J.; Seilern und Aspang, J.; Shim, J.; Cho, J. The Impact of Suture Button Removal in Syndesmosis Fixation. J. Clin. Med. 2021, 10, 3726. [Google Scholar] [CrossRef]
- Dao, T.T.; LeResche, L. Gender differences in pain. J. Orofac. Pain 2000, 14, 169–195. [Google Scholar] [PubMed]
- Dingemans, S.A.; Birnie, M.F.N.; Sanders, F.R.K.; Bekerom, M.P.J.v.D.; Backes, M.; van Beeck, E.; Bloemers, F.W.; van Dijkman, B.; Flikweert, E.; Haverkamp, D.; et al. Routine versus on demand removal of the syndesmotic screw; a protocol for an international randomised controlled trial (RODEO-trial). BMC Musculoskelet. Disord. 2018, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Briceno, J.; Wusu, T.; Kaiser, P.; Cronin, P.; Leblanc, A.; Miller, C.; Kwon, J.Y. Effect of Syndesmotic Implant Removal on Dorsiflexion. Foot Ankle Int. 2019, 40, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Boyle, M.J.; Gao, R.; Frampton, C.M.A.; Coleman, B. Removal of the syndesmotic screw after the surgical treatment of a fracture of the ankle in adult patients does not affect one-year outcomes. Bone Jt. J. 2014, 96-B, 1699–1705. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Screw Removal (n = 93) | Conservative Approach (n = 51) | p-Value * |
|---|---|---|---|
| Age, years | 32.8 ± 12.5 | 33.5 ± 14.1 | 0.759 |
| Sex (men, %) | 56 (60.2%) | 23 (45.1%) | 0.081 |
| Overweight (>25.0 kg/m2) | 36 (38.7%) | 24 (47.1%) | 0.331 |
| Area of residence (urban) | 58 (62.4%) | 28 (54.9%) | 0.382 |
| Relationship status (married) | 62 (66.7%) | 37 (72.5%) | 0.466 |
| Level of income (average or higher) | 53 (57.0%) | 29 (56.9%) | 0.988 |
| Level of education (higher education) | 66 (71.0%) | 31 (60.8%) | 0.212 |
| Occupation (employed) | 51 (54.8%) | 32 (62.7%) | 0.358 |
| Frequent alcohol consumption | 10 (10.8%) | 8 (15.7%) | 0.392 |
| Frequent smoker | 25 (26.9%) | 17 (33.3%) | 0.415 |
| CCI > 2 | 8 (8.6%) | 3 (5.9%) | 0.556 |
| Fracture type | 0.762 | ||
| Unimalleolar | 24 (25.8%) | 12 (23.5%) | |
| Bimalleolar | 49 (52.7%) | 24 (47.1%) | |
| Lauge–Hansen classification | 0.185 | ||
| SER | 42 (45.2%) | 17 (33.3%) | |
| PER | 30 (32.3%) | 14 (27.5%) | |
| SA | 10 (10.8%) | 11 (21.6%) | |
| PA | 11 (11.8%) | 8 (15.7%) |
| Questions | Screw Removal (n = 93) | Conservative Approach (n = 51) | p-Value * |
|---|---|---|---|
| Q1: How satisfied are you with your overall mobility since the surgical procedure? | 7.8 ± 2.5 | 6.7 ± 2.9 | 0.018 |
| Q2: To what extent do you believe the removal (or retention) of the syndesmotic screw impacted better your ability to perform daily living activities? | 8.1 ± 2.1 | 6.5 ± 3.0 | <0.001 |
| Q3: How often do you experience pain or discomfort in the area of the surgical procedure? | 5.3 ± 2.7 | 6.8 ± 3.2 | 0.003 |
| Q4: Would you recommend the same treatment approach to someone else with a similar condition? (1 being not likely, 10 being highly likely) | 7.6 ± 1.9 | 7.4 ± 2.6 | 0.591 |
| Q5: How has this surgical procedure impacted your quality of life? (higher is better) | 6.9 ± 3.3 | 7.1 ± 2.8 | 0.714 |
| Q6: How confident are you in your decision (either removal or retention of the screw)? | 8.9 ± 1.6 | 7.8 ± 2.4 | 0.013 |
| Q7: Have you noticed any limitations in daily activities due to the surgical procedure? | 5.6 ± 2.9 | 6.9 ± 3.3 | 0.016 |
| Q8: On a scale of 1 to 10, how would you rate the information provided to you regarding the pros and cons of screw removal versus retention? | 8.4 ± 1.8 | 8.0 ± 2.0 | 0.222 |
| Scores (Mean ± SD) | Screw Removal (n = 93) | Conservative Approach (n = 51) | p-Value * |
|---|---|---|---|
| SF-36—Physical | 55.9 ± 6.6 | 53.3 ± 6.8 | 0.027 |
| SF-36—Mental | 54.9 ± 7.2 | 53.0 ± 7.6 | 0.140 |
| SF-36—Total | 56.4 ± 7.8 | 55.1 ± 8.2 | 0.349 |
| WHOQOL-BREF (Mean ± SD) | Screw Removal (n = 93) | Conservative Approach (n = 51) | p-Value * |
|---|---|---|---|
| Physical domain | 64.8 ± 12.2 | 60.9 ± 11.6 | 0.064 |
| Mental domain | 62.3 ± 13.8 | 66.4 ± 12.8 | 0.082 |
| Social domain | 60.8 ± 12.9 | 65.5 ± 13.1 | 0.039 |
| Environmental domain | 63.8 ± 11.6 | 62.0 ± 13.3 | 0.399 |
| HADS (Mean ± SD) | Screw Removal (n = 93) | Conservative Approach (n = 51) | p-Value * |
|---|---|---|---|
| Anxiety | 5.8 ± 3.4 | 7.3 ± 2.5 | 0.006 |
| Depression | 6.3 ± 2.3 | 6.9 ± 1.8 | 0.109 |
| Total score | 12.1 ± 4.6 | 13.0 ± 4.3 | 0.252 |
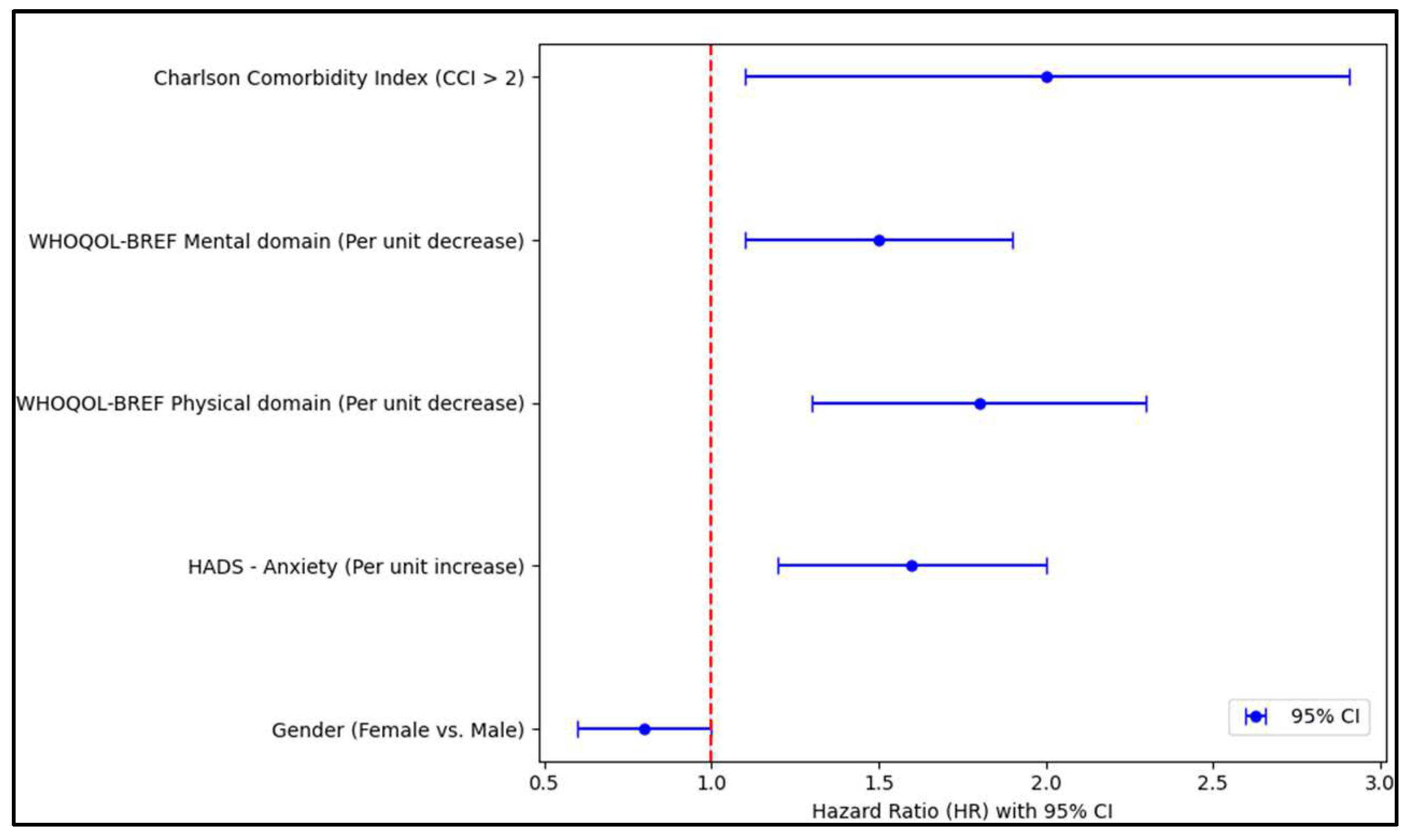
| Independent Variables | HR—Exp (B) | 95% CI | p-Value |
|---|---|---|---|
| Gender (Female vs. Male) | 0.8 | 0.6–1.1 | 0.014 |
| Age (Per year increase) | 1.02 | 0.97–1.19 | 0.132 |
| Overweight (>25.0 kg/m2) | 1.4 | 1.0–1.9 | 0.072 |
| Area of residence (Urban vs. Rural) | 1.1 | 0.8–1.4 | 0.621 |
| Relationship status (Relationship vs. Single) | 0.9 | 0.6–1.3 | 0.466 |
| Level of income (Average or higher vs. Below average) | 1.2 | 0.9–2.6 | 0.201 |
| Level of education (Higher vs. Below higher) | 1.1 | 0.8–1.5 | 0.499 |
| Occupation (Employed vs. Unemployed) | 0.9 | 0.7–1.1 | 0.173 |
| Frequent alcohol consumption (Yes vs. No) | 0.8 | 0.6–1.2 | 0.091 |
| Frequent smoker (Yes vs. No) | 1.2 | 0.9–1.6 | 0.212 |
| Fracture type (Unimalleolar vs. Bimalleolar) | 1.2 | 0.9–2.2 | 0.193 |
| HADS—Anxiety (Per unit increase) | 1.6 | 1.2–3.1 | 0.006 |
| HADS—Depression (Per unit increase) | 1.1 | 0.9–2.0 | 0.218 |
| WHOQOL-BREF Physical domain | 1.8 | 1.3–2.5 | <0.001 |
| WHOQOL-BREF Mental domain | 1.5 | 1.1–2.8 | 0.013 |
| WHOQOL-BREF Social domain | 1.6 | 0.9–2.2 | 0.095 |
| WHOQOL-BREF Environmental domain | 1.4 | 1.0–1.9 | 0.068 |
| Charlson Comorbidity Index (CCI > 2) | 2.0 | 1.1–3.6 | 0.024 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanda, I.-I.; Hosin, S.; Vermesan, D.; Deleanu, B.; Pop, D.; Crisan, D.; Al-Qatawneh, M.; Mioc, M.; Prejbeanu, R.; Rosca, O. Impact of Syndesmotic Screw Removal on Quality of Life, Mobility, and Daily Living Activities in Patients Post Distal Tibiofibular Diastasis Repair. Medicina 2023, 59, 2048. https://doi.org/10.3390/medicina59122048
Sanda I-I, Hosin S, Vermesan D, Deleanu B, Pop D, Crisan D, Al-Qatawneh M, Mioc M, Prejbeanu R, Rosca O. Impact of Syndesmotic Screw Removal on Quality of Life, Mobility, and Daily Living Activities in Patients Post Distal Tibiofibular Diastasis Repair. Medicina. 2023; 59(12):2048. https://doi.org/10.3390/medicina59122048
Chicago/Turabian StyleSanda, Isabella-Ionela, Samer Hosin, Dinu Vermesan, Bogdan Deleanu, Daniel Pop, Dan Crisan, Musab Al-Qatawneh, Mihai Mioc, Radu Prejbeanu, and Ovidiu Rosca. 2023. "Impact of Syndesmotic Screw Removal on Quality of Life, Mobility, and Daily Living Activities in Patients Post Distal Tibiofibular Diastasis Repair" Medicina 59, no. 12: 2048. https://doi.org/10.3390/medicina59122048