
The Use of Nano-Hydroxyapatite (NH) for Socket Preservation: Communication of an Upcoming Multicenter Study with the Presentation of a Pilot Case Report

 , , ,
, , ,  and
and 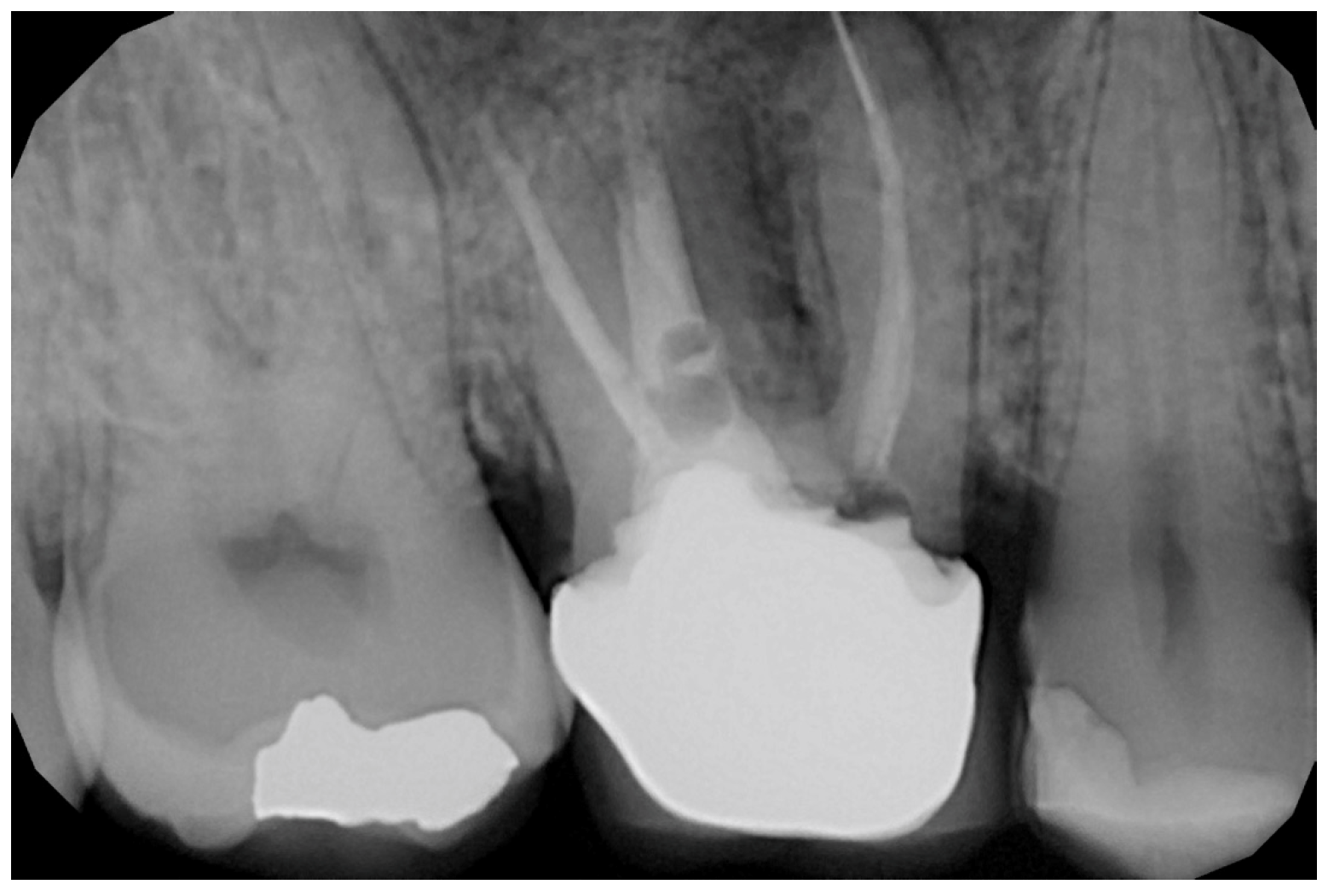{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives of Multicenter Study
- To evaluate and compare two postextraction sites treated with nano-HA in the posterior regions (test) and the control sites, thus involving 4 or 5 sites of the jaws, after 24 weeks of healing;
- To determine the bone values of these sites in an evaluation during implant site preparation;
- To determine whether the addition of nano-HA increases the amount of bone using a site evaluation;
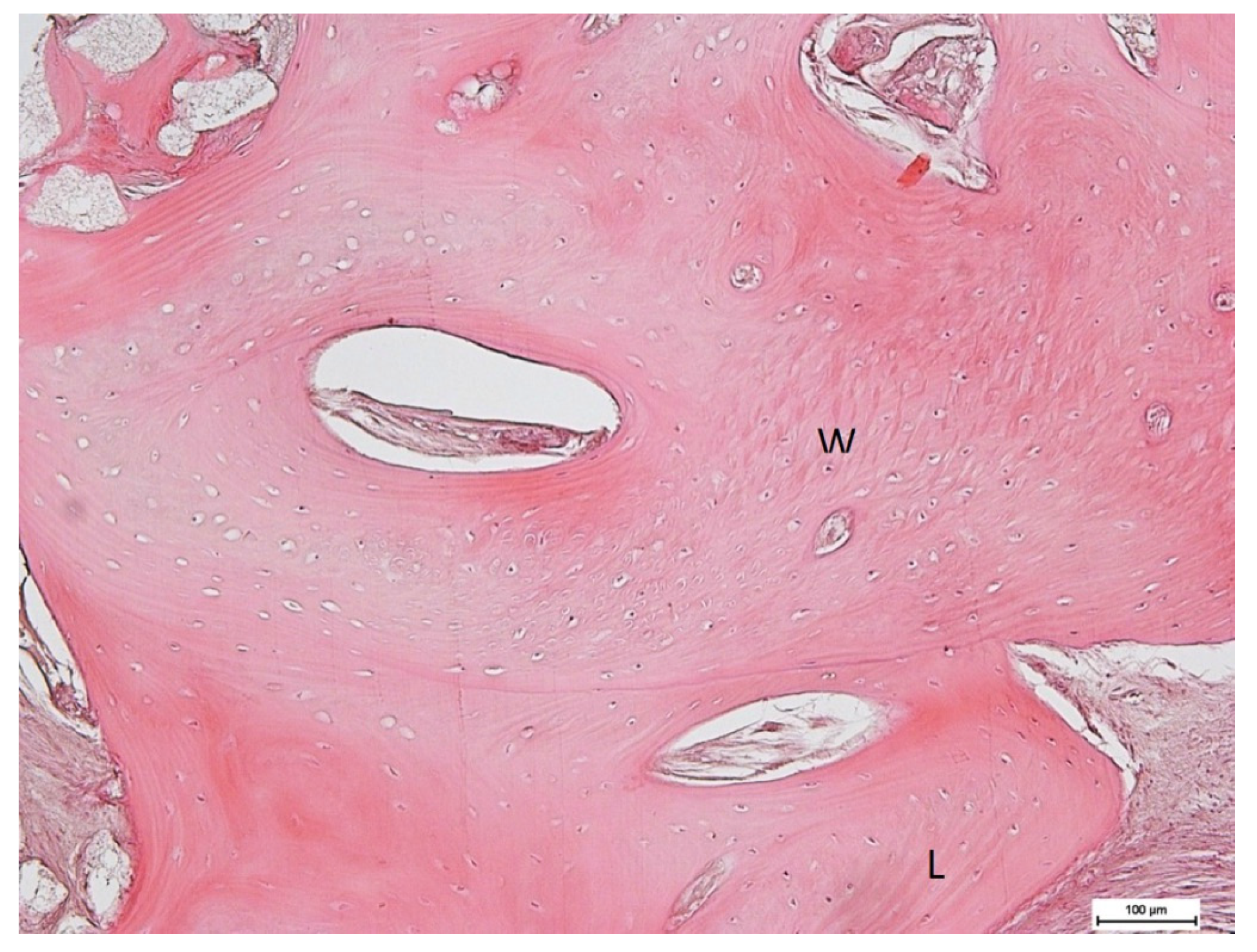
- To determine the bone quality of the sites based on a histological evaluation.
2.2. Study Population of Preliminary Study
2.3. Study Population of Multicentric Study
- Age >18 years old;
- General good health (ASA I-II);
- Adequate oral hygiene (Full Mouth Plaque Score ≤ 20%, Full Mouth Bleeding Score ≤ 20%);
- Two adjacent teeth to be extracted in the same quadrant in 4 and 5 sites.
- Pregnant or within lactating period;
- Untreated periodontitis;
- Osteometabolic disease;
- Intravenous bisphosphonates therapy;
- History of chemotherapy or radiation therapy applied to the neck and head area;
- Frequent smoking habits (>15 cigarettes/per day);
- Absence of buccal bone plate;
- Patients with active local infection.
2.4. The Nano-Ha:NuvaBone
2.5. Surgical Technique
2.6. Case Presentation. Nano-HA Applied to Socket Preservation Procedures
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Weber, F.E. Reconsidering Osteoconduction in the Era of Additive Manufacturing. Tissue Eng. Part B Rev. 2019, 25, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Jordana, F.; Le Visage, C.; Weiss, P. Substituts osseux. Med. Sci. 2017, 33, 60–65. [Google Scholar] [CrossRef]
- Kao, S.T.; Scott, D.D. A Review of Bone Substitutes. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Zizzari, V.L.; Zara, S.; Tetè, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biologic and clinical aspects of integration of different bone substitutes in oral surgery: A literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 392–402. [Google Scholar] [CrossRef]
- Aludden, H.C.; Mordenfeld, A.; Hallman, M.; Dahlin, C.; Jensen, T. Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autogenous bone graft: A systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhou, W.; Li, P.; Luo, Q.; Li, A.; Zhang, X. Comparison of the osteogenic effectiveness of an autogenous demineralised dentin matrix and Bio-Oss® in bone augmentation: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2022, 60, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Keil, C.; Gollmer, B.; Zeidler-Rentzsch, I.; Gredes, T.; Heinemann, F. Histological evaluation of extraction sites grafted with Bio-Oss Collagen: Randomized controlled trial. Ann. Anat.—Anat. Anz. 2021, 237, 151722. [Google Scholar] [CrossRef]
- Palachur, D.; Rao, K.P.; Murthy, K.V.; Kishore, D.; Reddy, M.; Bhupathi, A. A comparative evaluation of bovine-derived xenograft (Bio-Oss Collagen) and type I collagen membrane (Bio-Gide) with bovine-derived xenograft (Bio-Oss Collagen) and fibrin fibronectin sealing system (TISSEEL) in the treatment of intrabony defects: A clinico-radiographic study. J. Indian Soc. Periodontol. 2014, 18, 336–343. [Google Scholar] [CrossRef]
- Tetè, S.; Zizzari, V.L.; Vinci, R.; Zara, S.; Di Tore, U.; Manica, M.; Cataldi, A.; Mortellaro, C.; Piattelli, A.; Gherlone, E. Equine and porcine bone substitutes in maxillary sinus augmentation: A histological and immunohistochemical analysis of VEGF expression. J. Craniofac. Surg. 2014, 25, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Pagliani, L.; Andersson, P.; Lanza, M.; Nappo, A.; Verrocchi, D.; Volpe, S.; Sennerby, L. A collagenated porcine bone substitute for augmentation at Neoss implant sites: A prospective 1-year multicenter case series study with histology. Clin. Implant. Dent. Relat. Res. 2012, 14, 746–758. [Google Scholar] [CrossRef] [PubMed]
- Green, D.W.; Ben-Nissan, B.; Yoon, K.S.; Milthorpe, B.; Jung, H.-S. Natural and Synthetic Coral Biomineralization for Human Bone Revitalization. Trends Biotechnol. 2017, 35, 43–54. [Google Scholar] [CrossRef]
- Ratnayake, J.T.B.; Mucalo, M.; Dias, G.J. Substituted hydroxyapatites for bone regeneration: A review of current trends. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 105, 1285–1299. [Google Scholar] [CrossRef]
- Khoshakhlagh, P.; Rabiee, S.M.; Kiaee, G.; Heidari, P.; Miri, A.K.; Moradi, R.; Moztarzadeh, F.; Ravarian, R. Development and characterization of a bioglass/chitosan composite as an injectable bone substitute. Carbohydr. Polym. 2017, 157, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Rizwan, M.; Hamdi, M.; Basirun, W.J. Bioglass® 45S5-based composites for bone tissue engineering and functional applications. J. Biomed. Mater. Res. Part A 2017, 105, 3197–3223. [Google Scholar] [CrossRef] [PubMed]
- Luvizuto, E.R.D.; Queiroz, T.P.D.; Margonar, R.D.; Panzarini, S.R.D.; Hochuli-Vieira, E.D.; Okamoto, T.D.; Okamoto, R.D. Osteoconductive Properties of β-Tricalcium Phosphate Matrix, Polylactic and Polyglycolic Acid Gel, and Calcium Phosphate Cement in Bone Defects. J. Craniofacial Surg. 2012, 23, e430–e433. [Google Scholar] [CrossRef] [PubMed]
- Lanao, R.P.F.; Jonker, A.M.; Wolke, J.G.; Jansen, J.A.; van Hest, J.C.; Leeuwenburgh, S.C.; Gkioni, K.; Douglas, T.E.; Mikos, A.G.; Sariibrahimoglu, K.; et al. Physicochemical properties and applications of poly(lactic-co-glycolic acid) for use in bone regeneration. Tissue Eng. Part B Rev. 2013, 19, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef]
- Wei, G.; Ma, P.X. Structure and properties of nano-hydroxyapatite/polymer composite scaffolds for bone tissue engineering. Biomaterials 2004, 25, 4749–4757. [Google Scholar] [CrossRef]
- Kalita, S.J.; Bhardwaj, A.; Bhatt, H.A. Nanocrystalline calcium phosphate ceramics in biomedical engineering. Mater. Sci. Eng. C 2007, 27, 441–449. [Google Scholar] [CrossRef]
- Mostafa, N.Y.; Brown, P.W. Computer simulation of stoichiometric hydroxyapatite: Structure and substitutions. J. Phys. Chem. Solids 2007, 68, 431–437. [Google Scholar] [CrossRef]
- Teixeira, S.; Rodriguez, M.; Pena, P.; De Aza, A.; De Aza, S.; Ferraz, M.; Monteiro, F. Physical characterization of hydroxyapatite porous scaffolds for tissue engineering. Mater. Sci. Eng. C 2009, 29, 1510–1514. [Google Scholar] [CrossRef]
- Guo, L.; Huang, M.; Zhang, X. Effects of sintering temperature on structure of hydroxyapatite studied with Rietveld method. J. Mater. Sci. Mater. Med. 2003, 14, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Kavasi, R.-M.; Coelho, C.C.; Platania, V.; Quadros, P.A.; Chatzinikolaidou, M. In vitro biocompatibility assessment of nano-hydroxyapatite. Nanomaterials 2021, 11, 1152. [Google Scholar] [CrossRef]
- Maddalone, M.; Mirabelli, L.; Scavia, S.; Roncucci, R.; Bianco, E.; Bader, A. Vertical Bone Augmentation with GBR Pocket Technique: Surgical Procedure and Preliminary Results. J. Contemp. Dent. Pr. 2021, 22, 1370–1376. [Google Scholar] [CrossRef]
- Alkindi, M.; Ramalingam, S.; Alghamdi, O.; Alomran, O.M.; Binsalah, M.A.; Badwelan, M. Guided bone regeneration with osteoconductive grafts and PDGF: A tissue engineering option for segmental bone defect reconstruction. J. Appl. Biomater. Funct. Mater. 2021, 19, 2280800020987405. [Google Scholar] [CrossRef]
- Quirino, L.C.; Carvalho, P.H.d.A.; Neto, R.T.A.; Comachio, C.A.; Monteiro, N.G.; Ervolino-Silva, A.C.; Okamoto, R.; Pereira-Filho, V.A. Polydioxanone Membrane Compared with Collagen Membrane for Bone Regeneration. Polymers 2023, 15, 868. [Google Scholar] [CrossRef]
- Lee, J.-H.; An, H.-W.; Im, J.-S.; Kim, W.-J.; Lee, D.-W.; Yun, J.-H. Evaluation of the clinical and radiographic effectiveness of treating peri-implant bone defects with a new biphasic calcium phosphate bone graft: A prospective, multicenter randomized controlled trial. J. Periodontal Implant. Sci. 2023, 53, 306–317. [Google Scholar] [CrossRef]
- Zych, Ł.; Osyczka, A.M.; Łacz, A.; Różycka, A.; Niemiec, W.; Rapacz-Kmita, A.; Dzierzkowska, E.; Stodolak-Zych, E. How Surface Properties of Silica Nanoparticles Influence Structural, Microstructural and Biological Properties of Polymer Nanocomposites. Materials 2021, 14, 843. [Google Scholar] [CrossRef]
- Pistilli, R.; Simion, M.; Barausse, C.; Gasparro, R.; Pistilli, V.; Bellini, P.; Felice, P. Guided Bone Regeneration with Nonresorbable Membranes in the Rehabilitation of Partially Edentulous Atrophic Arches: A Retrospective Study on 122 Implants with a 3- to 7-Year Follow-up. Int. J. Periodontics Restor. Dent. 2020, 40, 685–692. [Google Scholar] [CrossRef]
- Tamburaci, S.; Tihminlioglu, F. Development of Si doped nano hydroxyapatite reinforced bilayer chitosan nanocomposite barrier membranes for guided bone regeneration. Mater. Sci. Eng. C 2021, 128, 112298. [Google Scholar] [CrossRef]
- Memè, L.; Santarelli, A.; Marzo, G.; Lo Muzio, L.; Bambini, F. Novel hydroxyapatite biomaterial covalently linked to raloxifene. Int. J. Immunopathol. Pharmacol. 2014, 27, 437–444. [Google Scholar] [CrossRef]
- Lo Muzio, L.; Santarelli, A.; Orsini, G.; Putignano, A.; Bambini, F. MG63 and MC3T3-E1 osteoblastic cell lines response to raloxifene. Eur. J. Inflamm. 2013, 11, 797–804. [Google Scholar] [CrossRef]
- Santos, A.M.d.S.; Pereira, R.d.S.; Montemezzi, P.; Mello-Machado, R.C.; Okamoto, R.; Sacco, R.; Lisboa-Filho, P.N.; Messora, M.R.; Mourão, C.F.; Hochuli-Vieira, E. The Interplay of Raloxifene and Sonochemical Bio-Oss in Early Maxillary Sinus Bone Regeneration: A Histological and Immunohistochemical Analysis in Rabbits. Medicina 2023, 59, 1521. [Google Scholar] [CrossRef] [PubMed]
- Santarelli, A.; Mascitti, M.; Orsini, G.; Lo Muzio, L.; Bambini, F. Osteopontin, osteocalcin and OB-cadherin expression in synthetic nanohydroxyapatite vs. bovine hydroxyapatite cultured osteoblastic-like cells. J. Biol. Regul. Homeost. Agents 2014, 28, 523–529. [Google Scholar]
- Mummolo, S.; Nota, A.; Marchetti, E.; Marzo, G.; Campanella, V. Histologic and histomorphometric analysis of maxillary sinus augmentation with different biomaterials. A pilot split-mouth human study. ORAL Implantol. 2018, 11, 249–256. [Google Scholar]
- Nguyen, V.; von Krockow, N.; Pouchet, J.; Weigl, P. Periosteal Inhibition Technique for Alveolar Ridge Preservation as It Applies to Implant Therapy. Int. J. Periodontics Restor. Dent. 2019, 39, 737–744. [Google Scholar] [CrossRef]
- Grassi, A.; Memè, L.; Strappa, E.M.; Martini, E.; Bambini, F. Modified Periosteal Inhibition (MPI) Technique for Extraction Sockets: A Case Series Report. Appl. Sci. 2022, 12, 12292. [Google Scholar] [CrossRef]
- Memè, L.; Bambini, F.; Gallusi, G.; Strappa, E.M.; Mummolo, S. The Effect and the Potential Use of Magnetic–Dam Barrier in Guided Bone Regeneration: A Laboratory Study. Appl. Sci. 2023, 13, 1625. [Google Scholar] [CrossRef]
- Thurzo, A.; Gálfiová, P.; Nováková, Z.V.; Polák, Š.; Varga, I.; Strunga, M.; Urban, R.; Surovková, J.; Leško, L.; Hajdúchová, Z.; et al. Fabrication and In Vitro Characterization of Novel Hydroxyapatite Scaffolds 3D Printed Using Polyvinyl Alcohol as a Thermoplastic Binder. Int. J. Mol. Sci. 2022, 23, 14870. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, G.; Johnson, B.N.; Jia, X. Three-dimensional (3D) printed scaffold and material selection for bone repair. Acta Biomater. 2018, 84, 16–33. [Google Scholar] [CrossRef]
- Wang, T.; Guo, Y. The Host Response to Autogenous, Allogeneic, and Xenogeneic Treated Dentin Matrix/Demineralized Dentin Matrix-Oriented Tissue Regeneration. Tissue Eng. Part B Rev. 2023. [Google Scholar] [CrossRef]
- Memè, L.; Strappa, E.M.; Monterubbianesi, R.; Bambini, F.; Mummolo, S. SEM and FT-MIR Analysis of Human Demineralized Dentin Matrix: An In Vitro Study. Appl. Sci. 2022, 12, 1480. [Google Scholar] [CrossRef]
- Sultan, N.; Jayash, S.N. Evaluation of osteogenic potential of demineralized dentin matrix hydrogel for bone formation. BMC Oral Health 2023, 23, 247. [Google Scholar] [CrossRef] [PubMed]
- Dłucik, R.; Orzechowska-Wylęgała, B.; Dłucik, D.; Puzzolo, D.; Santoro, G.; Micali, A.; Testagrossa, B.; Acri, G. Comparison of clinical efficacy of three different dentin matrix biomaterials obtained from different devices. Expert Rev. Med. Devices 2023, 20, 313–327. [Google Scholar] [CrossRef]
- Bernardi, S.; Mummolo, S.; Tecco, S.; Continenza, M.A.; Marzo, G. Histological characterization of Sacco’s concentrated growth factors membrane|Caracterización Histológica de la Membrana de los Factores de Crecimiento Concentrados Sacco. Int. J. Morphol. 2017, 35, 114–119. [Google Scholar] [CrossRef]
- Jain, P.; Shetye, A.G.; Rathee, M.; Agarkar, V.; Kaushik, S.; Alam, M. Effect of advanced platelet-rich fibrin and concentrated growth factor on tissues around implants in maxillary anterior region. J. Indian Prosthodont. Soc. 2022, 22, 169–178. [Google Scholar] [CrossRef]
- Karthik, V.; Prabhu, K.; Bharath, N.; Shobana, P.; Indhu, K.; Abraham, S.; Arunalakshmi, K. Randomized controlled study on effect of concentrated growth factors on crestal bone levels and peri-implant bone density in dental implants. J. Pharm. Bioallied Sci. 2022, 14 (Suppl. 1), S68–S77. [Google Scholar] [CrossRef] [PubMed]
- Jalkh, E.B.B.; Tovar, N.; Arbex, L.; Kurgansky, G.; Torroni, A.; Gil, L.F.; Wall, B.; Kohanbash, K.; Bonfante, E.A.; Coelho, P.G.; et al. Effect of leukocyte-platelet-rich fibrin in bone healing around dental implants placed in conventional and wide osteotomy sites: A pre-clinical study. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 2705–2713. [Google Scholar] [CrossRef]
- Gheno, E.; Alves, G.G.; Ghiretti, R.; Mello-Machado, R.C.; Signore, A.; Lourenço, E.S.; Leite, P.E.C.; Mourão, C.F.d.A.B.; Sohn, D.-S.; Calasans-Maia, M.D. “Sticky Bone” Preparation Device: A Pilot Study on the Release of Cytokines and Growth Factors. Materials 2022, 15, 1474. [Google Scholar] [CrossRef]
- Gheno, E.; Carlos Fernando de Almeida Barros, C.; de Mello-Machado, R.C.; Lourenço, E.S.; Miron, R.J.; Catarino, K.F.F.; Alves, A.T.; Alves, G.G.; Calasans-Maia, M.D. In vivo evaluation of the biocompatibility and biodegradation of a new denatured plasma membrane combined with liquid PRF (Alb-PRF). Platelets 2020, 32, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Pinto, N.R.; Pereda, A.; Jiménez, P.; Del Corso, M.; Kang, B.-S.; Nally, M.; Lanata, N.; Wang, H.-L.; Quirynen, M. The impact of the centrifuge characteristics and centrifugation protocols on the cells, growth factors, and fibrin architecture of a leukocyte- and platelet-rich fibrin (L-PRF) clot and membrane. Platelets 2018, 29, 171–184. [Google Scholar] [CrossRef] [PubMed]


















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, R.; Carli, E.; Bambini, F.; Mummolo, S.; Licini, C.; Memè, L. The Use of Nano-Hydroxyapatite (NH) for Socket Preservation: Communication of an Upcoming Multicenter Study with the Presentation of a Pilot Case Report. Medicina 2023, 59, 1978. https://doi.org/10.3390/medicina59111978
Rossi R, Carli E, Bambini F, Mummolo S, Licini C, Memè L. The Use of Nano-Hydroxyapatite (NH) for Socket Preservation: Communication of an Upcoming Multicenter Study with the Presentation of a Pilot Case Report. Medicina. 2023; 59(11):1978. https://doi.org/10.3390/medicina59111978
Chicago/Turabian StyleRossi, Roberto, Elisabetta Carli, Fabrizio Bambini, Stefano Mummolo, Caterina Licini, and Lucia Memè. 2023. "The Use of Nano-Hydroxyapatite (NH) for Socket Preservation: Communication of an Upcoming Multicenter Study with the Presentation of a Pilot Case Report" Medicina 59, no. 11: 1978. https://doi.org/10.3390/medicina59111978