
Comparison of Efficacy of Lidocaine and Articaine as Inferior Alveolar Nerve Blocking Agents in Patients with Symptomatic Irreversible Pulpitis: Randomized Controlled Trial
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Trial Design
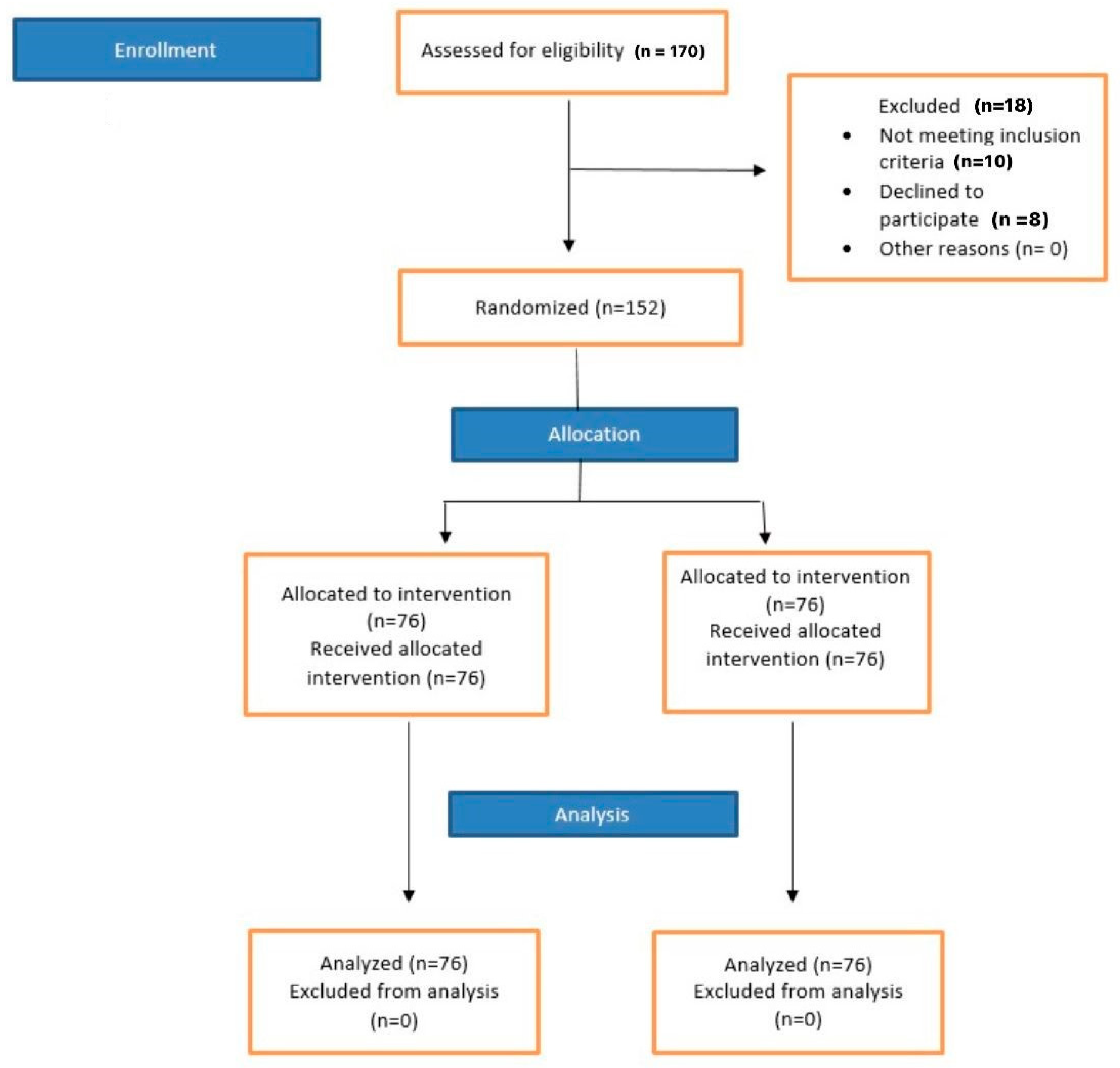
2.3. Sample Size Calculation
2.4. Eligibility Criteria
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
2.5. Randomization and Blinding
2.5.1. Random Allocation SEQUENCE Generation
2.5.2. Allocation Concealment
2.5.3. Implementation
2.6. Intervention
2.6.1. Control Group
2.6.2. Experimental Group
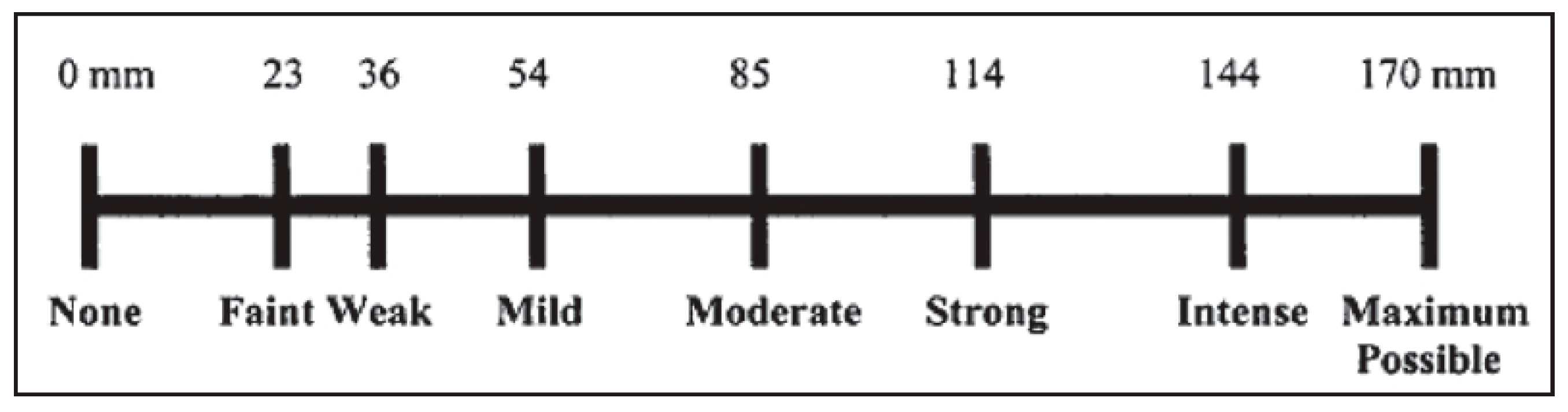
2.7. Outcome Assessment
- No pain: 0 mm.
- Mild pain: between 0 and 54 mm.
- Moderate pain: between 54 and 114 mm.
- Severe pain: ≥114 mm.
2.8. Statistical Analysis
3. Results
4. Discussion
4.1. Strengths of the Study
4.2. Limitations of the Study
5. Conclusions
6. Future Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, D. Triumph Over Pain: The Curiously Contentious History of Ether. In Proceedings of the 14th Annual History of Medicine Days, Calgary, AB, Canada, 18–19 March 2005. [Google Scholar]
- Malamed, S.F. Local anesthetics: Dentistry’s most important drugs, clinical update 2006. J. Calif. Dent. Assoc. 2006, 34, 971–976. [Google Scholar] [CrossRef]
- Ranjan, R.; Kumar, S.S.; Singh, M. Comparison of efficacy of 0.75% ropivacaine and 2% lidocaine with 1: 200,000 adrenaline in pain control in extraction of mandibular posterior teeth: A double-blind study. Indian J. Dent. Res. 2018, 29, 611. [Google Scholar] [PubMed]
- Minu, M.O.; Ajay, R.H.; Bhat, S.S.; Sargod, S.; Riyas, A.K.; Suvarna, R.M. Comparison of the Local Anaesthetic Effect of 4% Articaine and 2% Lidocaine Administered Using Inferior Alveolar Nerve Block Technique in Primary Mandibular Molar Extractions. J. Evol. Med. Dent. Sci. 2021, 10, 13–19. [Google Scholar]
- Ghadimi, S.; Shahrabi, M.; Khosravi, Z.; Behroozi, R. Efficacy of articaine infiltration versus lidocaine inferior alveolar nerve block for pulpotomy in mandibular primary second molars: A randomized clinical trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 97. [Google Scholar] [CrossRef] [PubMed]
- Malamed, S. Articaine 30 years later. Oral Health 2016, 106, 42–68. [Google Scholar]
- Isen, D. Articaine: Pharmacology and clinical use of a recently approved local anesthetic. Dent. Today 2000, 19, 72–77. [Google Scholar]
- Yapp, K.E.; Hopcraft, M.S.; Parashos, P. Dentists’ perceptions of a new local anaesthetic drug—Articaine. Aust. Dent. J. 2012, 57, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Corbett, I. Increasing popularity of articaine. Br. Dent. J. 2021, 230, 790–791. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Tang, H.; Liu, S.; Ma, C.; Ma, S.; Zhao, H. Anesthetic efficiency of articaine versus lidocaine in the extraction of lower third molars: A meta-analysis and systematic review. J. Oral Maxillofac. Surg. 2019, 77, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Ghazalgoo, A.; Saatchi, M.; Khazaei, S.; Shadmehr, E. The effect of using articaine versus lidocaine for inferior alveolar nerve block on pain after root canal treatment: A Prospective, Randomized clinical study. Dent. Hypotheses 2018, 9, 80. [Google Scholar]
- Costa, C.G.; Tortamano, I.P.; Rocha, R.G.; Francischone, C.E.; Tortamano, N. Onset and duration periods of articaine and lidocaine on maxillary infiltration. J. Prosthet. Dent. 2005, 94, 381. [Google Scholar] [CrossRef]
- Kanaa, M.D.; Whitworth, J.M.; Corbett, I.P.; Meechan, J.G. Articaine and lidocaine mandibular buccal infiltration anesthesia: A prospective randomized double-blind cross-over study. J. Endod. 2006, 32, 296–298. [Google Scholar] [CrossRef]
- Robertson, D.; Nusstein, J.; Reader, A.; Beck, M.; McCartney, M. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior teeth. J. Am. Dent. Assoc. 2007, 138, 1104–1112. [Google Scholar] [CrossRef]
- Petrovskaia, L.; IuM, M.; Grinin, V. Comparative efficiency of local anesthetics from the group of complex amides during therapeutic stomatological interventions. Stomatologiia 2002, 81, 38–41. [Google Scholar] [PubMed]
- Tong, H.J.; Alzahrani, F.S.; Sim, Y.F.; Tahmassebi, J.F.; Duggal, M. Anaesthetic efficacy of articaine versus lidocaine in children’s dentistry: A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2018, 28, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Mittal, J.; Kaur, G.; Mann, H.S.; Narang, S.; Kamra, M.; Kapoor, S.; Sindhi, M.; Kataria, R. Comparative Study of the Efficacy of 4% Articaine vs 2% Lidocaine in Surgical Removal of Bilaterally Impacted Mandibular Third Molars. J. Contemp. Dent. Pract. 2018, 19, 743–748. [Google Scholar]
- Sierra Rebolledo, A.; Delgado Molina, E.; Berini Aytés, L.; Gay Escoda, C. Comparative study of the anesthetic efficacy of 4% articaine versus 2% lidocaine in inferior alveolar nerve block during surgical extraction of impacted lower third molars. Med. Oral Patol. Oral Cirugía Bucal 2007, 12, 139–144. [Google Scholar]
- Rosenberg, P.A.; Amin, K.G.; Zibari, Y.; Lin, L.M. Comparison of 4% articaine with 1: 100,000 epinephrine and 2% lidocaine with 1: 100,000 epinephrine when used as a supplemental anesthetic. J. Endod. 2007, 33, 403–405. [Google Scholar] [CrossRef] [PubMed]
- Sherman, M.G.; Flax, M.; Namerow, K.; Murray, P.E. Anesthetic efficacy of the Gow-Gates injection and maxillary infiltration with articaine and lidocaine for irreversible pulpitis. J. Endod. 2008, 34, 656–659. [Google Scholar] [CrossRef]
- Srinivasan, N.; Kavitha, M.; Loganathan, C.S.; Padmini, G. Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.; Nusstein, J.; Drum, M.; Reader, A.; Beck, M. A prospective, randomized, double-blind comparison of articaine and lidocaine for maxillary infiltrations. J. Endod. 2008, 34, 389–393. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Duncan, H.; Bjørndal, L.; Kvist, T.; Priya, E.; Jayaraman, J.; Pulikkotil, M.; Pigg, D.K.; Rechenberg, M.; Væth, P.M.; et al. PRIRATE 2020 guidelines for reporting randomized trials in Endodontics: A consensus-based development. Int. Endod. J. 2020, 53, 764–773. [Google Scholar] [CrossRef]
- Cuschieri, S. The CONSORT statement. Saudi J. Anaesth. 2019, 13 (Suppl. 1), S27. [Google Scholar] [CrossRef] [PubMed]
- Lang, T.A.; Talerico, C.; Siontis, G.C. Documenting clinical and laboratory images in publications: The CLIP principles. Chest 2012, 141, 1626–1632. [Google Scholar] [CrossRef]
- Tortamano, I.P.; Siviero, M.; Costa, C.G.; Buscariolo, I.A.; Armonia, P.L. A comparison of the anesthetic efficacy of articaine and lidocaine in patients with irreversible pulpitis. J. Endod. 2009, 35, 165–168. [Google Scholar] [CrossRef]
- Shapiro, M.R.; McDonald, N.J.; Gardner, R.J.; Peters, M.C.; Botero, T.M. Efficacy of articaine versus lidocaine in supplemental infiltration for mandibular first versus second molars with irreversible pulpitis: A prospective, randomized, double-blind clinical trial. J. Endod. 2018, 44, 523–528. [Google Scholar] [CrossRef]
- Mikesell, P.; Nusstein, J.; Reader, A.; Beck, M.; Weaver, J. A comparison of articaine and lidocaine for inferior alveolar nerve blocks. J. Endod. 2005, 31, 265–270. [Google Scholar] [CrossRef]
- Haase, A.; Reader, A.; Nusstein, J.; Beck, M.; Drum, M. Comparing anesthetic efficacy of articaine versus lidocaine as a supplemental buccal infiltration of the mandibular first molar after an inferior alveolar nerve block. J. Am. Dent. Assoc. 2008, 139, 1228–1235. [Google Scholar] [CrossRef]
- Poorni, S.; Veniashok, B.; Senthilkumar, A.D.; Indira, R.; Ramachandran, S. Anesthetic efficacy of four percent articaine for pulpal anesthesia by using inferior alveolar nerve block and buccal infiltration techniques in patients with irreversible pulpitis: A prospective randomized double-blind clinical trial. J. Endod. 2011, 37, 1603–1607. [Google Scholar] [CrossRef]
- Simon, M.; Gielen, M.; Alberink, N.; Vree, T.; Van Egmond, J. Intravenous regional anesthesia with 0.5% articaine, 0.5% lidocaine, or 0.5% prilocaine: A double-blind randomized clinical study. Reg. Anesth. Pain Med. 1997, 22, 29–34. [Google Scholar] [CrossRef]
- Malamed, S.F.; Gagnon, S.; Leblanc, D. A comparison between articaine HCl and lidocaine HCl in pediatric dental patients. Pediatr. Dent. 2000, 22, 307–311. [Google Scholar]
- Aggarwal, V.; Singla, M.; Miglani, S. Comparative Evaluation of Anesthetic Efficacy of 2% Lidocaine, 4% Articaine, and 0.5% Bupivacaine on Inferior Alveolar Nerve Block in Patients with Symptomatic Irreversible Pulpitis: A Prospective, Randomized, Double-blind Clinical Trial. J. Oral Facial Pain Headache 2017, 31, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, P.C.; Ranali, J.; Bovi Ambrosano, G.M.; de Oliveira, P.C.; Groppo, F.C.; Meechan, J.G.; Volpato, M.C. Anesthetic efficacy of 3 volumes of lidocaine with epinephrine in maxillary infiltration anesthesia. Anesth. Prog. 2008, 55, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Mittal, M.; Sharma, S.; Kumar, A.; Chopra, R.; Srivastava, D. Comparison of Anesthetic Efficacy of Articaine and Lidocaine in Patients with Irreversible Pulpitis. Pak. J. Med. Health Sci. 2021, 15, 843–846. [Google Scholar]
- Khan, Q.; Noor, N.; Anayat, N.; Khan, T.S.; Ahmed, M. Comparison of Anaesthetic Efficacy Of Articaine And Lidocaine In Nonsurgical Endodontic Treatment Of Permanent Mandibular Molars With Symptomatic Irreversible Pulpitis. A Randomized Clinical Trial. J. Ayub Med. Coll. Abbottabad Pak. 2021, 33, 192–197. [Google Scholar]
- Nagendrababu, V.; Duncan, H.; Whitworth, J.; Nekoofar, M.; Pulikkotil, S.; Veettil, S.; Dummer, P.M.H. Is articaine more effective than lidocaine in patients with irreversible pulpitis? An umbrella review. Int. Endod. J. 2020, 53, 200–213. [Google Scholar] [CrossRef]
- Almaiman, S.; Bahkali, S.; Alabdulatif, N.; Bahkaly, A.; Al-Surimi, K.; Househ, M. Promoting oral health using social media platforms: Seeking Arabic online oral health related information (OHRI). Stud. Health Technol. Inform. 2016, 226, 283–286. [Google Scholar]
- St George, G.; Morgan, A.; Meechan, J.; Moles, D.R.; Needleman, I.; Ng, Y.L.; Petrie, A. Injectable Local Anaesthetic Agents for Dental Anaesthesia. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Lee, R.J.; Ratnayake, J. Demographics, Practising Arrangements, and Standards: Survey among New Zealand Dentists. Int. J. Dent. 2018, 2018, 7675917. [Google Scholar] [CrossRef]
- Toma, M.; Berghahn, M.; Loth, S.; Verrengia, B.; Visani, L.; Velotti, F. Articaine and Paresthesia in Dental Anesthesia: Neurotoxicity or Procedural Trauma; Oral Health Group: Toronto, ON, Canada, 2016. [Google Scholar]
- Aquilanti, L.; Mascitti, M.; Togni, L.; Contaldo, M.; Rappelli, G.; Santarelli, A. A Systematic Review on Nerve-Related Adverse Effects following Mandibular Nerve Block Anesthesia. Int. J. Environ. Res. Public Health 2022, 19, 1627. [Google Scholar] [CrossRef]
- Wright, C. Therapeutic Guidelines: Oral and Dental. Version 2. Aust. Prescr. 2012, 35, 182. [Google Scholar] [CrossRef]
- Piccinni, C.; Gissi, D.B.; Gabusi, A.; Montebugnoli, L.; Poluzzi, E. Paraesthesia after local anaesthetics: An analysis of reports to the FDA Adverse Event Reporting System. Basic Clin. Pharmacol. Toxicol. 2015, 117, 52–56. [Google Scholar] [CrossRef]
- Tan, Y.-Z.; Shi, R.-J.; Ke, B.-W.; Tang, Y.-L.; Liang, X.-H. Paresthesia in dentistry: The ignored neurotoxicity of local anesthetics. Heliyon 2023, 9, e18031. [Google Scholar] [CrossRef]
- Ahmad, M. The anatomical nature of dental paresthesia: A quick review. Open Dent. J. 2018, 12, 155. [Google Scholar] [CrossRef]
- Cornelius, C.; Roser, M.; Wiethölter, H.; Wolburg, H. Nerve injection injuries due to local anaesthetics. Experimental work. J. Craniomaxillofac Surg. 2000, 28 (Suppl. 3), 134–135. [Google Scholar]
- Cohen, H.P.; Cha, B.Y.; Spångberg, L.S. Endodontic anesthesia in mandibular molars: A clinical study. J. Endod. 1993, 19, 370–373. [Google Scholar] [CrossRef]
- Patel, R.; Bansal, N.; Dudulwar, G.; Gupta, D. Evaluation of post-obturation pain after single-visit versus multiple-visit non-surgical endodontic treatments. Int. J. Cur. Res. Rev. 2021, 13, S66–S69. [Google Scholar] [CrossRef]
- DiRenzo, A.; Gresla, T.; Johnson, B.R.; Rogers, M.; Tucker, D.; BeGole, E.A. Postoperative pain after 1-and 2-visit root canal therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.J.; Johnson, B.R.; Remeikis, N.A.; BeGole, E.A. Comparison of effect of intracanal use of ketorolac tromethamine and dexamethasone with oral ibuprofen on post treatment endodontic pain. J. Endod. 1999, 25, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Contributors Physiopedia Visual Analogue Scale: Physiopedia. 2023. Available online: https://www.physio-pedia.com/Visual_Analogue_Scale (accessed on 9 October 2023).
- González-Fernández, M.; Ghosh, N.; Ellison, T.; McLeod, J.C.; Pelletier, C.A.; Williams, K. Moving Beyond the Limitations of the Visual Analog Scale for Measuring Pain: Novel Use of the General Labeled Magnitude Scale in a Clinical Setting. Am. J. Phys. Med. Rehabil. 2014, 93, 75–81. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Effectiveness of Anesthetic Injection during * N(%) | |||
|---|---|---|---|
| Access Cavity Preparation | Initial Instrumentation | ||
| Control Group (Lidocaine) | Yes | 71(93) | 55(72) |
| No | 5(7) | 21(28) | |
| Experimental Group (Articaine) | Yes | 74(97) | 54(71) |
| No | 2(3) | 22(29) | |
| p-value | 0.246 | 0.857 | |
| Lidocaine n (%) | Articaine n (%) | p-Value * | sig/not sig | ||
| Tooth Type | 1st premolar | 1 (01) | 3 (04) | 0.334 | not sig |
| 2nd premolar | 15 (20) | 8 (11) | |||
| 1st molar | 44 (58) | 49 (64) | |||
| 2nd molar | 16 (21) | 16 (21) | |||
| 76 (100) | 76 (100) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, S.; Ahmed, A.; Saqib, W.; Abulhamael, A.M.; Habib, S.R.; Javed, M.Q. Comparison of Efficacy of Lidocaine and Articaine as Inferior Alveolar Nerve Blocking Agents in Patients with Symptomatic Irreversible Pulpitis: Randomized Controlled Trial. Medicina 2023, 59, 1840. https://doi.org/10.3390/medicina59101840
Hassan S, Ahmed A, Saqib W, Abulhamael AM, Habib SR, Javed MQ. Comparison of Efficacy of Lidocaine and Articaine as Inferior Alveolar Nerve Blocking Agents in Patients with Symptomatic Irreversible Pulpitis: Randomized Controlled Trial. Medicina. 2023; 59(10):1840. https://doi.org/10.3390/medicina59101840
Chicago/Turabian StyleHassan, Sobia, Alia Ahmed, Warda Saqib, Ayman M. Abulhamael, Syed Rashid Habib, and Muhammad Qasim Javed. 2023. "Comparison of Efficacy of Lidocaine and Articaine as Inferior Alveolar Nerve Blocking Agents in Patients with Symptomatic Irreversible Pulpitis: Randomized Controlled Trial" Medicina 59, no. 10: 1840. https://doi.org/10.3390/medicina59101840