
Sheep’s Head as an Anatomic Model for Basic Training in Endoscopic Sinus Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Acquisition for Anatomical Description and Anatomical Sectioning
2.2. Model Preparation for Surgery and Instrumentation
2.3. Participant Selection
2.4. Participant Assessment—Satisfaction Questionnaire
2.5. Statistical Analysis
3. Results
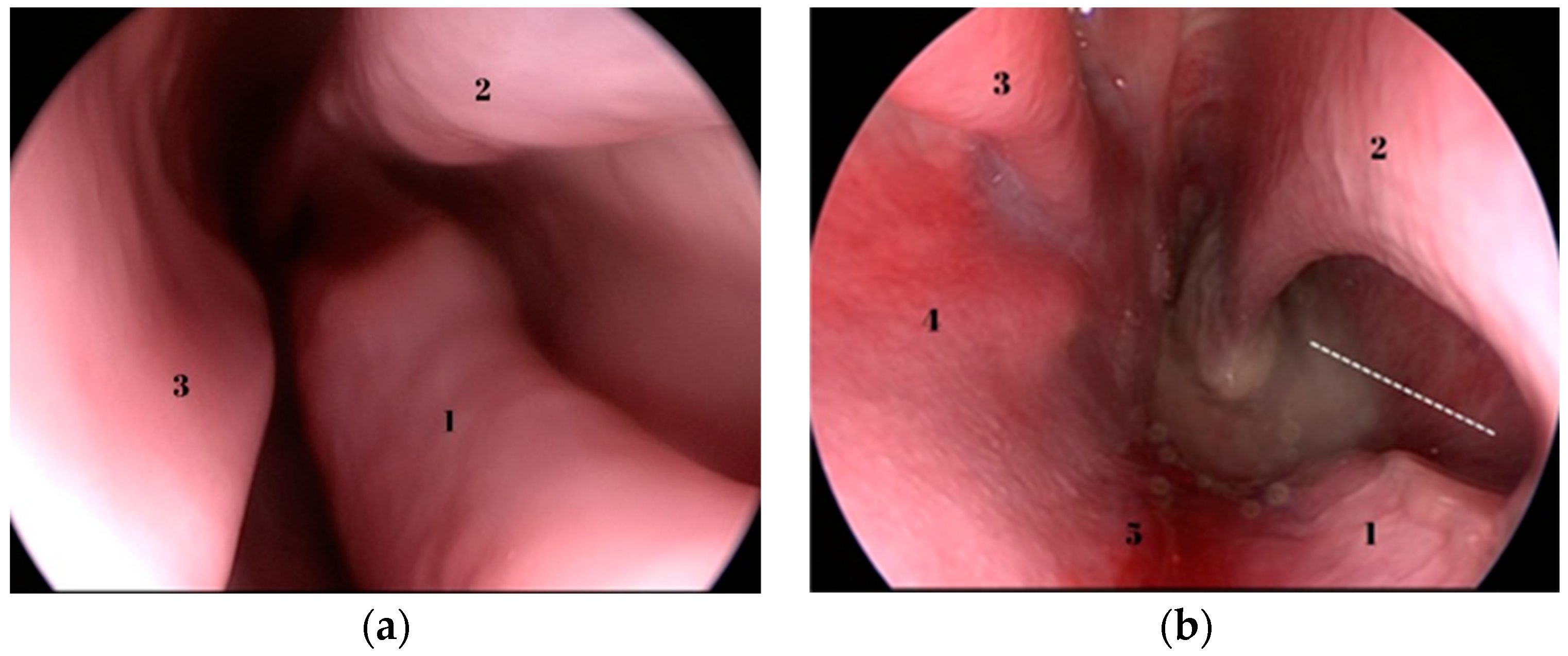
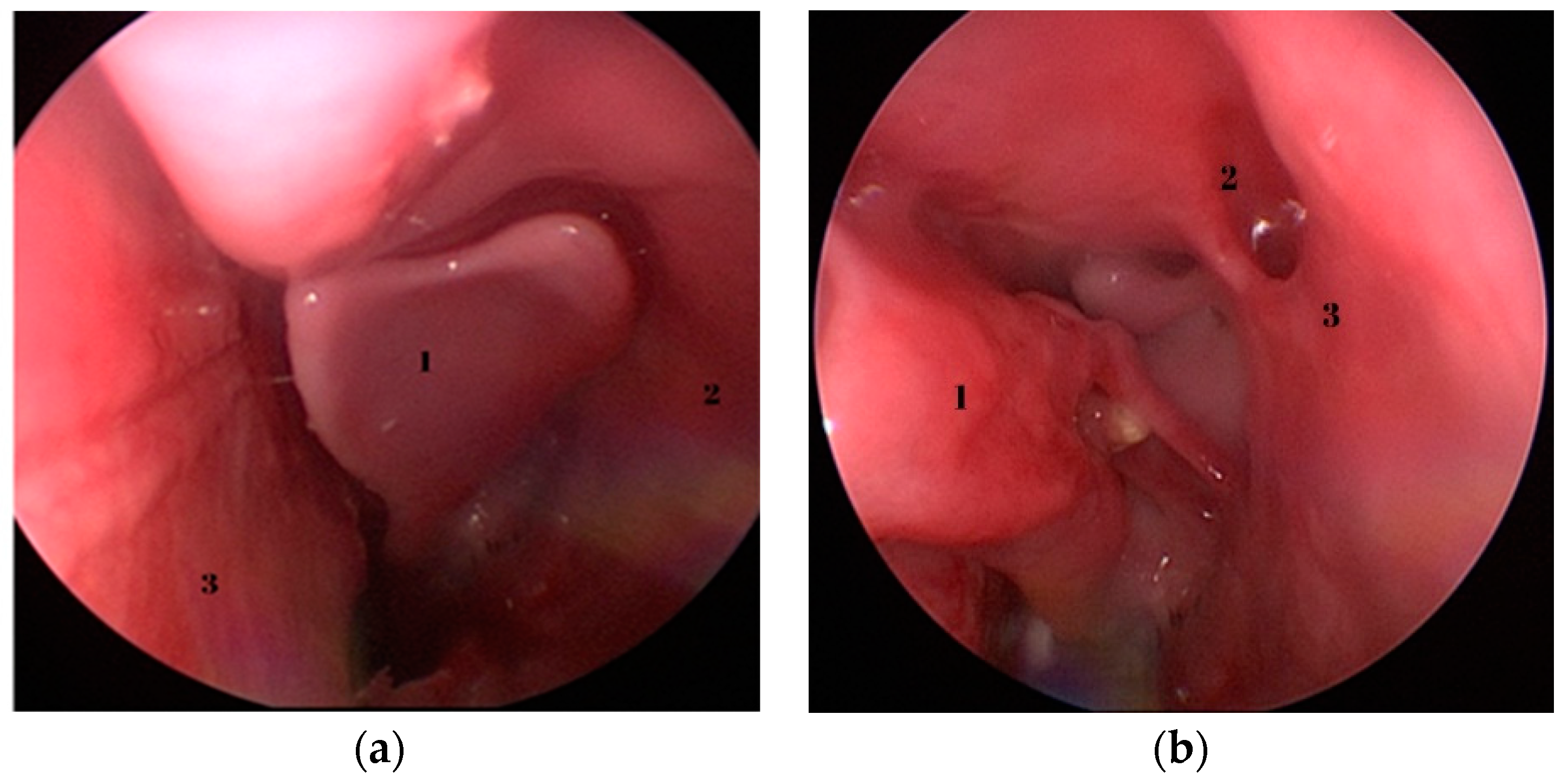
3.1. Basic Endoscopic Anatomy
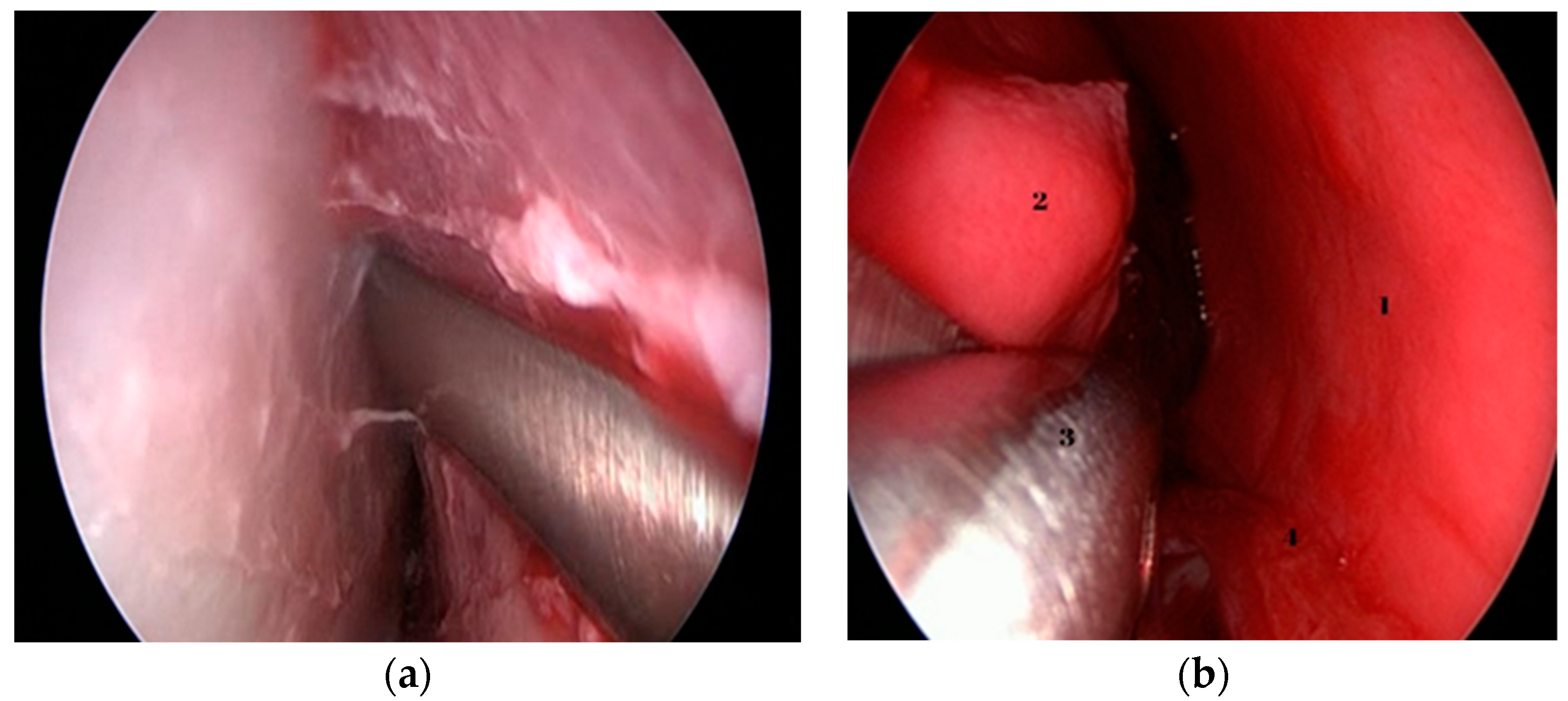
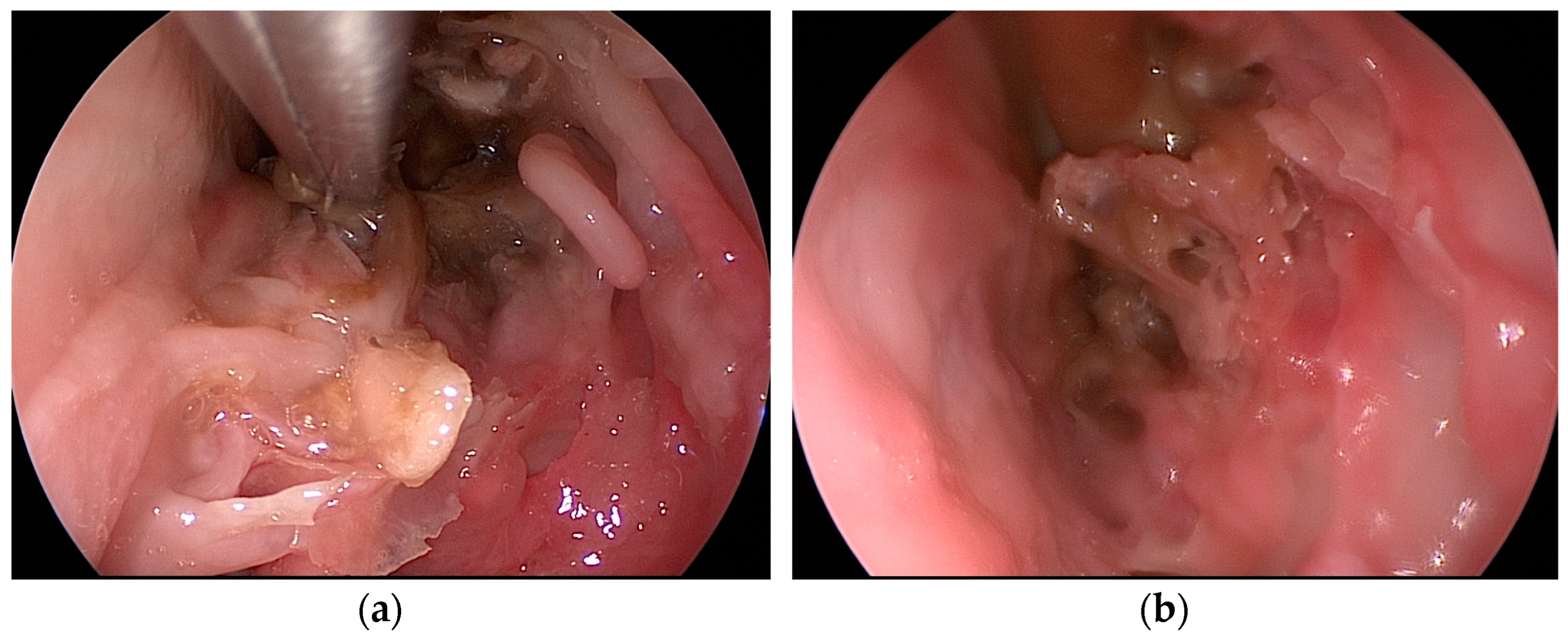
3.2. Procedures and Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mallmann, L.B.; Piltcher, O.B.; Isolan, G.R. The Lamb’s Head as a Model for Surgical Skills Development in Endonasal Surgery. J. Neurol. Surg. B Skull Base 2016, 77, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Stan, C.; Vesa, D.; Tănase, M.I.; Bulmaci, M.; Pop, S.; Rădeanu, D.G.; Cosgarea, M.; Maniu, A. Can Non-Virtual Reality Simulation Improve Surgical Training in Endoscopic Sinus Surgery? A Literature Review. Adv. Med. Educ. Pract. 2023, 14, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Stew, B.; Ooi, E. The role of simulation in endoscopic sinus surgery training. In Paranasal Sinuses; IntechOpen: London, UK, 2017. [Google Scholar] [CrossRef]
- Mills, R.; Lee, P. Surgical skills training in middle-ear surgery. J. Laryngol. Otol. 2003, 117, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Awad, Z.; Touska, P.; Arora, A.; Ziprin, P.; Darzi, A.; Tolley, N.S. Face and content validity of sheep heads in endoscopic rhinology training. Int. Forum. Allergy Rhinol. 2014, 4, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Awad, Z.; Taghi, A.; Sethukumar, P.; Tolley, N.S. Construct validity of the ovine model in endoscopic sinus surgery training. Laryngoscope 2015, 125, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Mladina, R. Endoscopic Surgical Anatomy of the Lamb’s Head; Storz Endo PressTM: Tuttlingen, Germany, 2011. [Google Scholar]
- Skitarelić, N.; Mladina, R. Lamb’s head: The model for novice education in endoscopic sinus surgery. World J. Methodol. 2015, 5, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, Q.; Oluwole, M.; Tan, L.; White, P.S. An animal model for training in endoscopic nasal and sinus surgery. J. Laryngol. Otol. 1996, 110, 425–428. [Google Scholar] [CrossRef]
- Mladina, R.; Vuković, K.; Štern Padovan, R.; Skitarelić, N. An animal model for endoscopic endonasal surgery and dacryocystorhinostomy training: Uses and limitations of the lamb’s head. J. Laryngol. Otol. 2011, 125, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Radeanu, D.; Stan, C.; Maniu, A.A. Utility of 3D Reconstructions for Preoperative Planning in Functional Endoscopic Sinus Surgery (FESS). In Proceedings of the 6th International Conference on Advancements of Medicine And Health Care through Technology, Meditech 2018, Cluj Napoca, Romania, 17–20 October 2018. [Google Scholar]
- Radeanu, D.; Marin, A.; Stan, C.; Maniu, A. FESS Role in Oral Surgery Rehabilitation. In Proceedings of the National Ent, Head and Neck Surgery Conference, Sibiu, Romania, 17–20 May 2017. [Google Scholar]
- Anschuetz, L.; Bonali, M.; Ghirelli, M.; Mattioli, F.; Villari, D.; Caversaccio, M.; Presutti, L. An Ovine Model for Exclusive Endoscopic Ear Surgery. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, S.; Yacoub, A.; Fernandez, I.J.; Niederhauser, L.; Fermi, M.; Caversaccio, M.; Marco, B.; Anschuetz, L. Exclusive Endoscopic Laser-Stapedotomy: Feasibility of an Ovine Training Model. Otol. Neurotol. 2021, 42, 994–1000. [Google Scholar] [CrossRef]
- Fernandez, I.J.; Bonali, M.; Yacoub, A.; Ghirelli, M.; Fermi, M.; Presutti, L.; Caversaccio, M.; Anschuetz, L. Training model for salvage procedures in endoscopic stapes surgery. Eur. Arch. Otorhinolaryngol. 2021, 278, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, G.; Wulc, A.E. Applicability of a sheep model for training in plastic surgery of eyelids and orbit. Ear Nose Throat J. 2022, 101 (Suppl. S2), 43S–49S. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.S.; Ianacone, D.C.; Isaacson, G.C. Ex vivo ovine model for teaching open laryngotracheal surgery. World J. Otorhinolaryngol. Head Neck Surg. 2018, 4, 140–144. [Google Scholar] [CrossRef]
- Valbonetti, L.; Berardinelli, P.; Scarano, A.; Piattelli, A.; Mattioli, M.; Barboni, B.; Vulpiani, M.P.; Muttini, A. Translational Value of Sheep as Animal Model to Study Sinus Augmentation. J. Craniofacial Surg. 2015, 26, 737–740. [Google Scholar] [CrossRef] [PubMed]
- Borner, U.; Caversaccio, M.; Wagner, F.; Marchal, F.; Anschuetz, L. First evaluation of an ovine training model for sialendoscopy. Laryngoscope Investig. Otolaryngol. 2023, 8, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Kamp, M.A.; Knipps, J.; Steiger, H.J.; Rapp, M.; Cornelius, J.F.; Folke-Sabel, S.; Sabel, M. Training for brain tumour resection: A realistic model with easy accessibility. Acta Neurochir. 2015, 157, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Korotkov, D.; Abramyan, A.; Wuo-Silva, R.; Chaddad-Neto, F. Cadaveric Sheep Head Model for Anterior Clinoidectomy in Neurosurgical Training. World Neurosurg. 2023, 175, e481–e491. [Google Scholar] [CrossRef] [PubMed]
- Altunrende, M.E.; Hamamcioglu, M.K.; Hıcdonmez, T.; Akcakaya, M.O.; Bırgılı, B.; Cobanoglu, S. Microsurgical training model for residents to approach to the orbit and the optic nerve in fresh cadaveric sheep cranium. J. Neurosci. Rural. Pract. 2014, 5, 151–154. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nr | Equipment (Germany—KARL STORZ SE & Co. KG, Tuttlingen) |
|---|---|
| 1. | Karl Storz TelePack X |
| 2. | Karl Storz rigid Hopkins telescopes 0° and 30° |
| 3. | Mladina head holder (Karl Storz®) |
| 4. | Blakesley nasal forceps (Karl Storz®) |
| 5. | Backbiter antrum punch (Karl Storz®) |
| 6. | Cottle dorsal scissors (Karl Storz®) |
| 7. | Freer elevator (Karl Storz®) |
| 8. | Sickle knife (Karl Storz®) |
| 9. | Straight and curved curette (Karl Storz®) |
| 10. | Frazier suction tube (Karl Storz®) |
| 11. | Scalpel handle with no. 11 blade (Karl Storz®) |
| Nr | Surgical Step |
|---|---|
| 1. | Foreign body removal (round plastic, popcorn) |
| 2. | Endoscopic septal resection |
| 3. | Endoscopic turbinoplasty |
| 4. | Maxillary anthrostomy |
| 5. | Ethmoidectomy |
| Questions | ENT Resident Mean (SD) | ENT Junior Mean (SD) | ENT Senior Mean (SD) | p Value 1 |
|---|---|---|---|---|
| The similarity of anatomical structures to humans | 3.1 (0.7) | 3.2 (0.6) | 3.0 (0) | 0.943 |
| Realistic perception of the mucosa | 4.7 (0.45) | 4.4 (0.8) | 4.33 (0.47) | 0.386 |
| Realistic perception of bone tissue | 4.4 (0.66) | 4.1 (0.83) | 4 (0) | 0.486 |
| Good depth perception | 4.2 (0.74) | 4.4 (0.48) | 5 (0) | 0.391 |
| Good applicability of the basic FESS instruments | 4.1 (0.94) | 4.4 (0.66) | 4 (0) | 0.475 |
| Useful to improve hand-eye coordination | 4.2 (0.6) | 4.4 (0.48) | 5 (0) | 0.660 |
| Useful to improve surgical technique | 4.1 (0.83) | 3.6 (0.66) | 4.33 (0.47) | 0.317 |
| Generally useful for basic endoscopic sinus surgery training | 4.1 (0.53) | 3.8 (0.6) | 4.33 (0.47) | 0.130 |
| Useful for endoscopic examination of the nasal cavities | 4.4 (0.48) | 4.5 (0.5) | 5 (0) | 0.340 |
| Useful for extraction of a foreign body | 4.8 (0.4) | 4.5 (0.5) | 4.66 (0.47) | 0.511 |
| Useful for the maxillary antrostomy | 3.6 (0.8) | 3.6 (0.48) | 3.66 (0.47) | 0.342 |
| Useful for the ethmoidectomy | 3 (0.73) | 2.6 (0.66) | 2.2 (0.4) | 0.191 |
| Useful for the septoplasty | 4.8 (0.4) | 4.2 (0.4) | 4.66 (0.47) | 0.582 |
| Useful for the lower turbinoplasty | 3.8 (0.4) | 4.4 (0.48) | 4.66 (0.47) | 0.088 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stan, C.; Ujvary, L.P.; Blebea, C.M.; Vesa, D.; Tănase, M.I.; Tănase, M.; Pop, S.S.; Rădeanu, D.G.; Maniu, A.A.; Cosgarea, M. Sheep’s Head as an Anatomic Model for Basic Training in Endoscopic Sinus Surgery. Medicina 2023, 59, 1792. https://doi.org/10.3390/medicina59101792
Stan C, Ujvary LP, Blebea CM, Vesa D, Tănase MI, Tănase M, Pop SS, Rădeanu DG, Maniu AA, Cosgarea M. Sheep’s Head as an Anatomic Model for Basic Training in Endoscopic Sinus Surgery. Medicina. 2023; 59(10):1792. https://doi.org/10.3390/medicina59101792
Chicago/Turabian StyleStan, Constantin, Laszlo Peter Ujvary, Cristina Maria Blebea, Doiniţa Vesa, Mihai Ionuţ Tănase, Mara Tănase, Septimiu Sever Pop, Doinel Gheorghe Rădeanu, Alma Aurelia Maniu, and Marcel Cosgarea. 2023. "Sheep’s Head as an Anatomic Model for Basic Training in Endoscopic Sinus Surgery" Medicina 59, no. 10: 1792. https://doi.org/10.3390/medicina59101792