
Breaking Barriers in Cranioplasty: 3D Printing in Low and Middle-Income Settings—Insights from Zenica, Bosnia and Herzegovina

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Evaluation
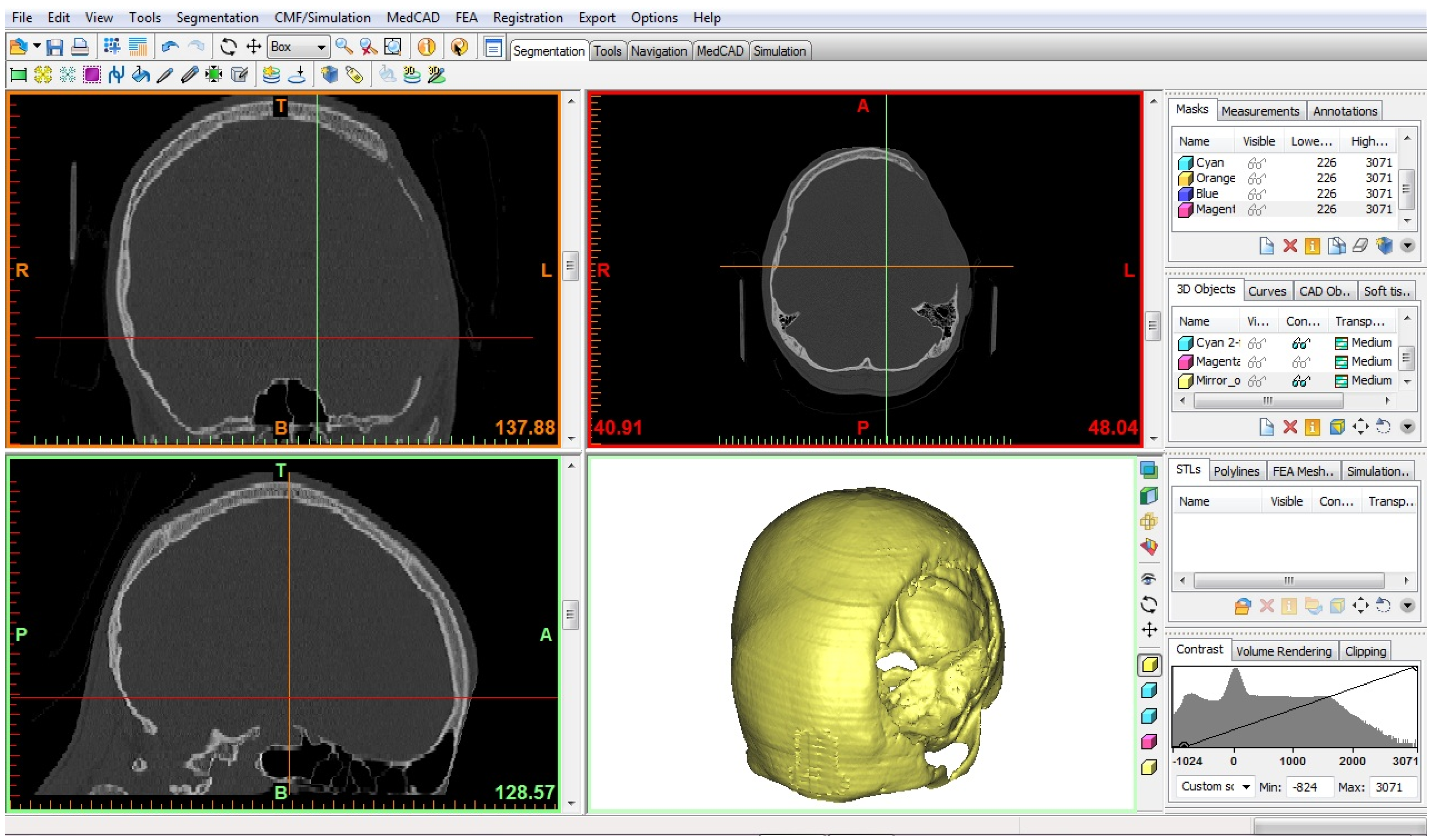
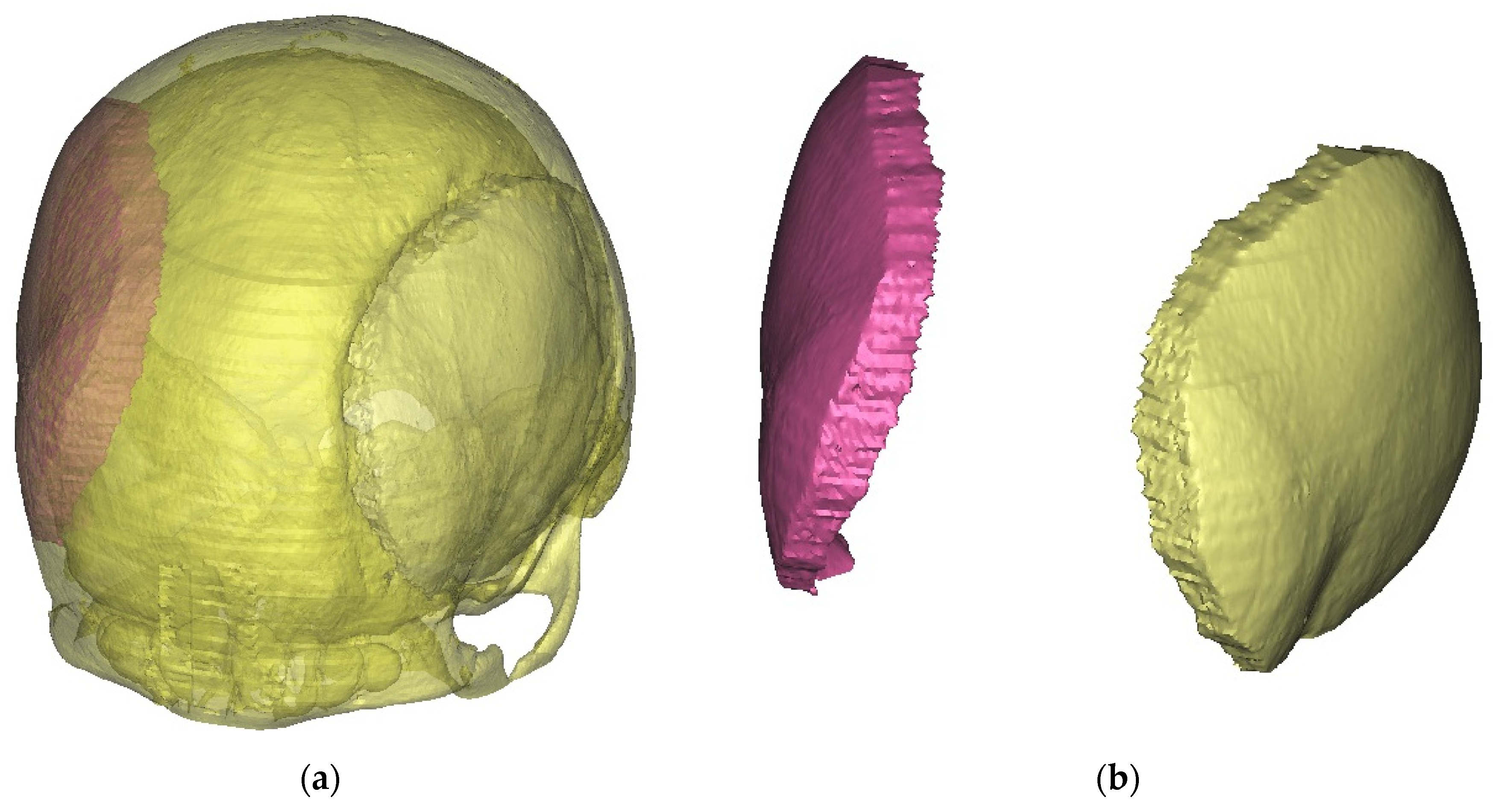
2.2. Technical Procedure
2.3. Surgical Procedure
2.4. Follow-Up Assesment
3. Results
3.1. Case Presentations
3.2. Radioogical Findings
3.3. Intraoperative Processing
3.4. Technological Process and Costs
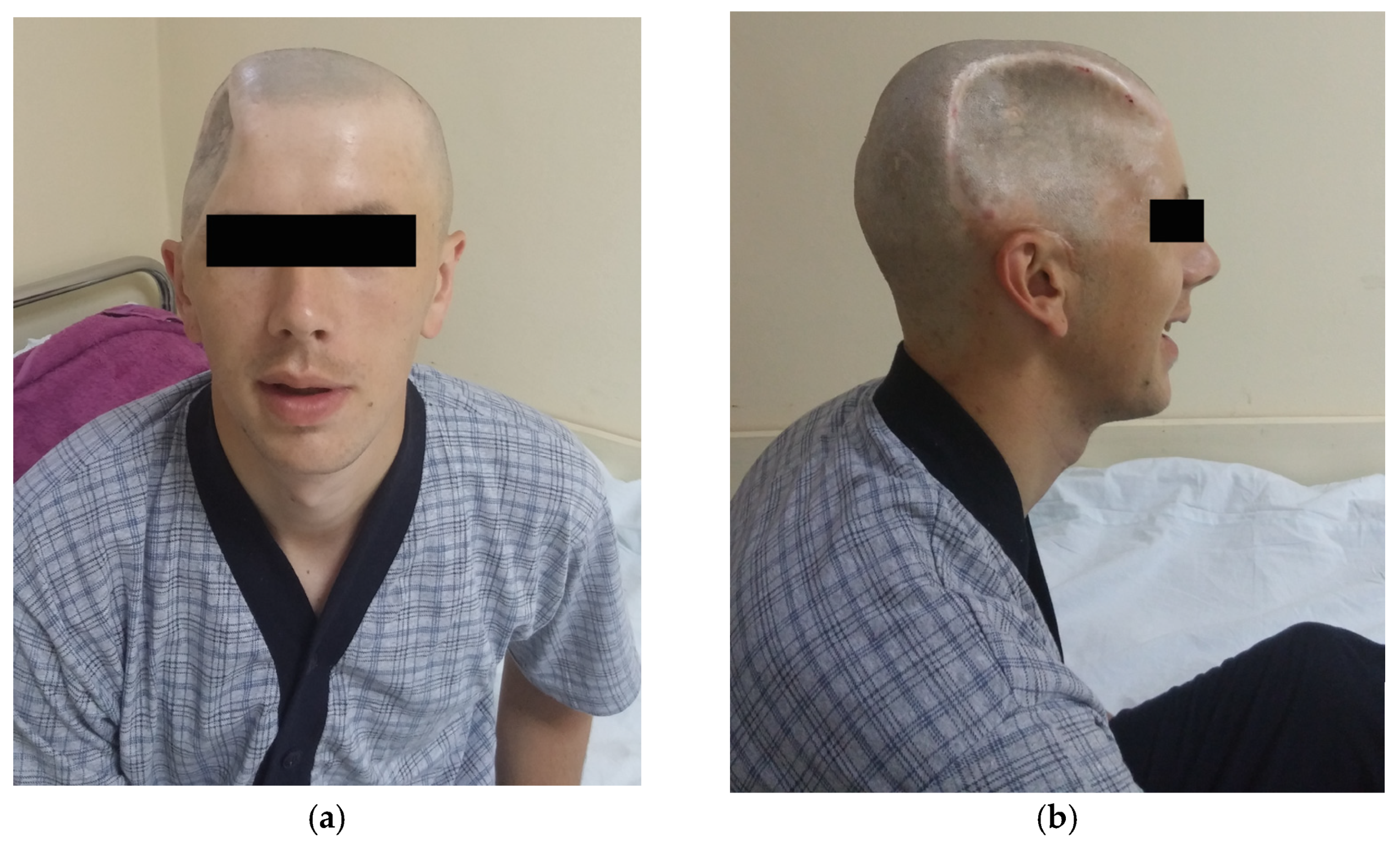
3.5. Outcome and Aestetic Satisfaction
4. Discussion
Overview of Implemented (Bosnian) Model for CP in LIMCs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aydin, S.; Kucukyuruk, B.; Abuzayed, B.; Aydin, S.; Sanus, G.Z. Cranioplasty: Review of materials and techniques. J. Neurosci. Rural Pract. 2011, 2, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Zanotti, B.; Zingaretti, N.; Verlicchi, A.; Robiony, M.; Alfieri, A.; Parodi, P.C. Cranioplasty: Review of Materials. J. Craniofac. Surg. 2016, 27, 2061–2072. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.S.; Luoma, A.M.; Wilson, S.R.; Kitchen, N. Titanium cranioplasty and the prediction of complications. Br. J. Neurosurg. 2012, 26, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Policicchio, D.; Casu, G.; Dipellegrini, G.; Doda, A.; Muggianu, G.; Boccaletti, R. Comparison of two different titanium cranioplasty methods: Custom-made titanium prostheses versus precurved titanium mesh. Surg. Neurol. Int. 2020, 11, 148. [Google Scholar] [CrossRef] [PubMed]
- Stoodley, M.A.; Abbott, J.R.; Simpson, D.A. Titanium cranioplasty using 3-D computer modelling of skull defects. J. Clin. Neurosci. 1996, 3, 149–155. [Google Scholar] [CrossRef]
- Omerhodzic, I.; Dzurlic, A.; Rovcanin, B.; Rotim, K.; Hadzimehmedagic, A.; Ahmetspahic, A.; Zvizdic, Z.; Granov, N.; Suljic, E. Hinge craniotomy as an alternative technique for patients with refractory intracranial hypertension. Brain Spine 2023, 3, 101758. [Google Scholar] [CrossRef]
- Schirmer, C.M.; Ackil, A.A., Jr.; Malek, A.M. Decompressive Craniectomy. Neurocrit. Care 2008, 8, 456–470. [Google Scholar] [CrossRef]
- Kolias, A.G.; Kirkpatrick, P.J.; Hutchinson, P.J. Decompressive craniectomy: Past, present and future. Nat. Rev. Neurol. 2013, 9, 405–415. [Google Scholar] [CrossRef]
- Belzberg, M.; Mitchell, K.A.; Ben-Shalom, N.; Asemota, A.O.; Wolff, A.Y.; Santiago, G.F.; Shay, T.; Huang, J.; Manson, P.N.; Brem, H.; et al. Cranioplasty Outcomes From 500 Consecutive Neuroplastic Surgery Patients. J. Craniofac. Surg. 2022, 33, 1648–1654. [Google Scholar] [CrossRef]
- Fallatah, M.A.; Aldahlawi, A.; Babateen, E.M.; Saif, S.; Alnejadi, W.; Bamsallm, M.; Lary, A. Outcomes of Cranioplasty: A Single-Center Experience. Cureus 2023, 15, e35213. [Google Scholar] [CrossRef]
- Posti, J.P.; Yli-Olli, M.; Heiskanen, L.; Aitasalo, K.M.J.; Rinne, J.; Vuorinen, V.; Serlo, W.; Tenovuo, O.; Vallittu, P.K.; Piitulainen, J.M. Cranioplasty After Severe Traumatic Brain Injury: Effects of Trauma and Patient Recovery on Cranioplasty Outcome. Front. Neurol. 2018, 9, 223. [Google Scholar] [CrossRef] [PubMed]
- Czyżewski, W.; Jachimczyk, J.; Hoffman, Z.; Szymoniuk, M.; Litak, J.; Maciejewski, M.; Kura, K.; Rola, R.; Torres, K. Low-Cost Cranioplasty-A Systematic Review of 3D Printing in Medicine. Materials 2022, 15, 4731. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Júnior, E.B.; de Aragão, A.H.; de Paula Loureiro, M.; Lobo, C.S.; Oliveti, A.F.; de Oliveira, R.M.; Ramina, R. Cranioplasty with three-dimensional customised mould for polymethylmethacrylate implant: A series of 16 consecutive patients with cost-effectiveness consideration. 3D Print. Med. 2021, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Spahić, D.; Beculić, H. An example of cranioplasty with the assistance of 3D printing technology. Mašinstvo 2019, 4, 207–211. [Google Scholar]
- Poukens, J.; Laeven, P.; Beerens, M.; Nijenhuis, G.; Sloten, J.V.; Stoelinga, P.; Kessler, P. A classification of cranial implants based on the degree of difficulty in computer design and manufacture. Int. J. Med. Robot. Comput. Assist. Surg. 2008, 4, 46–50. [Google Scholar] [CrossRef]
- Funk, W.; Podmelle, F.; Guiol, C.; Metelmann, H.R. Aesthetic satisfaction scoring—Introducing an aesthetic numeric analogue scale (ANA-scale). J. Craniomaxillofac. Surg. 2012, 40, 439–442. [Google Scholar] [CrossRef]
- De Bonis, P.; Frassanito, P.; Mangiola, A.; Nucci, C.G.; Anile, C.; Pompucci, A. Cranial repair: How complicated is filling a “hole”? J. Neurotrauma 2012, 29, 1071–1076. [Google Scholar] [CrossRef]
- Velin, L.; Lantz, A.; Ameh, E.A.; Roy, N.; Jumbam, D.T.; Williams, O.; Elobu, A.; Seyi-Olajide, J.; Hagander, L. Systematic review of low-income and middle-income country perceptions of visiting surgical teams from high-income countries. BMJ Glob. Health 2022, 7, e008791. [Google Scholar] [CrossRef]
- Rubagumya, F.; Hopman, W.M.; Gyawali, B.; Mukherji, D.; Hammad, N.; Pramesh, C.S.; Zubaryev, M.; Eniu, A.; Tsunoda, A.T.; Kutluk, T.; et al. Participation of Lower and Upper Middle-Income Countries in Clinical Trials Led by High-Income Countries. JAMA Netw. Open 2022, 5, e2227252. [Google Scholar] [CrossRef]
- Simunović, V.J. Health care in Bosnia and Herzegovina before, during, and after 1992–1995 war: A personal testimony. Confl. Health 2007, 1, 7. [Google Scholar] [CrossRef]
- Hodgetts, G.; Brown, G.; Batić-Mujanović, O.; Gavran, L.; Jatić, Z.; Račić, M.; Tešanović, G.; Zahilić, A.; Martin, M.; Birtwhistle, R. Twenty-five years on: Revisiting Bosnia and Herzegovina after implementation of a family medicine development program. BMC Fam. Pract. 2020, 21, 7. [Google Scholar] [CrossRef]
- Cubro, H.; Somun-Kapetanovic, R.; Thiery, G.; Talmor, D.; Gajic, O. Cost effectiveness of intensive care in a low resource setting: A prospective cohort of medical critically ill patients. World J. Crit. Care Med. 2016, 5, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Tokalić, R.; Viđak, M.; Kaknjo, M.M.; Marušić, A. Antifragility of healthcare systems in Croatia and Bosnia and Herzegovina: Learning from man-made and natural crises. Lancet Reg. Health-Eur. 2021, 9, 100216. [Google Scholar] [CrossRef] [PubMed]
- Masic, I. Medical Decision Making—An Overview. Acta Inform. Med. 2022, 30, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, C.; Kolias, A.; Adelson, P.D.; Rubiano, A.M.; Viaroli, E.; Buki, A.; Cinalli, G.; Fountas, K.; Khan, T.; Signoretti, S.; et al. Consensus statement from the international consensus meeting on post-traumatic cranioplasty. Acta Neurochir. 2021, 163, 423–440. [Google Scholar] [CrossRef]
- Karekezi, C. Editorial: Low-cost patient-specific cranial implants for cranioplasty. Acta Neurochir. 2023, 165, 2225–2226. [Google Scholar] [CrossRef]
- Maegele, M.; Lefering, R.; Sakowitz, O.; Kopp, M.A.; Schwab, J.M.; Steudel, W.I.; Unterberg, A.; Hoffmann, R.; Uhl, E.; Marzi, I. The Incidence and Management of Moderate to Severe Head Injury. Dtsch. Ärztebl. Int. 2019, 116, 167–173. [Google Scholar] [CrossRef]
- Zijlstra, I.A.; van der Steen, W.E.; Verbaan, D.; Majoie, C.B.; Marquering, H.A.; Coert, B.A.; Vandertop, W.P.; van den Berg, R. Ruptured middle cerebral artery aneurysms with a concomitant intraparenchymal hematoma: The role of hematoma volume. Neuroradiology 2018, 60, 335–342. [Google Scholar] [CrossRef]
- Johnson, W.C.; Ravindra, V.M.; Fielder, T.; Ishaque, M.; Patterson, T.T.; McGinity, M.J.; Lacci, J.V.; Grandhi, R. Surface Area of Decompressive Craniectomy Predicts Bone Flap Failure after Autologous Cranioplasty: A Radiographic Cohort Study. Neurotrauma Rep. 2021, 2, 391–398. [Google Scholar] [CrossRef]
- Quah, B.L.; Low, H.L.; Wilson, M.H.; Bimpis, A.; Nga, V.D.W.; Lwin, S.; Zainuddin, N.H.; Wahab, N.A.; Salek, M.A.A. Is There An Optimal Time for Performing CPs? Results from a Prospective Multinational Study. World Neurosurg. 2016, 94, 13–17. [Google Scholar] [CrossRef]
- Morton, R.P.; Abecassis, I.J.; Hanson, J.F.; Barber, J.K.; Chen, M.; Kelly, C.M.; Nerva, J.D.; Emerson, S.N.; Ene, C.I.; Levitt, M.R.; et al. Timing of cranioplasty: A 10.75-year single-center analysis of 754 patients. J. Neurosurg. 2018, 128, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- De Cola, M.C.; Corallo, F.; Pria, D.; Lo Buono, V.; Calabrò, R.S. Timing for cranioplasty to improve neurological outcome: A systematic review. Brain Behav. 2018, 8, e01106. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.F.; Lafuma, A.; Berdeaux, G.; Berto, P.; Brueggenjuergen, B.; Magaz, S.; Auffarth, G.K.; Brezin, A.; Caporossi, A.; Mendicute, J. Cost-effectiveness analysis of PMMA, silicone, or acrylic intra-ocular lenses in cataract surgery in four European countries. Ophthalmic Epidemiol. 2005, 12, 343–351. [Google Scholar] [CrossRef]
- Paulucci, B.P. PMMA Safety for Facial Filling: Review of Rates of Granuloma Occurrence and Treatment Methods. Aesthetic Plast. Surg. 2020, 44, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S. Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update. Polymers 2020, 12, 2299. [Google Scholar] [CrossRef]
- Mansouri, K.; Shaarawy, T.; Wedrich, A.; Mermoud, A. Comparing polymethylmethacrylate implant with collagen implant in deep sclerectomy: A randomized controlled trial. J. Glaucoma 2006, 15, 264–270. [Google Scholar] [CrossRef]
- Ashraf, M.; Choudhary, N.; Kamboh, U.A.; Raza, M.A.; Sultan, K.A.; Ghulam, N.; Hussain, S.S.; Ashraf, N. Early experience with patient-specific low-cost 3D-printed polymethylmethacrylate cranioplasty implants in a lower-middle-income-country: Technical note and economic analysis. Surg. Neurol. Int. 2022, 13, 270. [Google Scholar] [CrossRef]
- Loli Piccolomini, E.; Prato, M.; Scipione, M.; Sebastiani, A. CTprintNet: An Accurate and Stable Deep Unfolding Approach for Few-View CT Reconstruction. Algorithms 2023, 16, 270. [Google Scholar] [CrossRef]
- Bello, H.R.; Graves, J.A.; Rohatgi, S.; Vakil, M.; McCarty, J.; Van Hemert, R.L.; Geppert, S.; Peterson, R.B. Skull Base–related Lesions at Routine Head CT from the Emergency Department: Pearls, Pitfalls, and Lessons Learned. RadioGraphics 2019, 39, 1161–1182. [Google Scholar] [CrossRef]
- Bonne, N.X.; Dubrulle, F.; Risoud, M.; Vincent, C. How to perform 3D reconstruction of skull base tumours. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 117–120. [Google Scholar] [CrossRef]
- Shi, L.; Liu, B.; Yu, H.; Wei, C.; Wei, L.; Zeng, L.; Wang, G. Review of CT image reconstruction open source toolkits. J. Xray Sci. Technol. 2020, 28, 619–639. [Google Scholar] [CrossRef] [PubMed]
- Wettenhovi, V.V.; Vauhkonen, M.; Kolehmainen, V. OMEGA-open-source emission tomography software. Phys. Med. Biol. 2021, 66, 065010. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.M.; Noo, F.; Young, S.; Hsieh, S.S.; McNitt-Gray, M. Technical Note: FreeCT_ICD: An open-source implementation of a model-based iterative reconstruction method using coordinate descent optimization for CT imaging investigations. Med. Phys. 2018, 45, 3591–3603. [Google Scholar] [CrossRef]
- Yao, F.; Wang, J.; Yao, J.; Hang, F.; Lei, X.; Cao, Y. Three-dimensional image reconstruction with free open-source OsiriX software in video-assisted thoracoscopic lobectomy and segmentectomy. Int. J. Surg. 2017, 39, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Markovitz, M.A.; Lu, S.; Viswanadhan, N.A. Role of 3D Printing and Modeling to Aid in Neuroradiology Education for Medical Trainees. Fed. Pract. 2021, 38, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.L.; Lin, J.S.; Meng, H.; Su, N.; Yang, Y.; Fei, Q. A novel “three-dimensional-printed individual guide template-assisted percutaneous vertebroplasty” for osteoporotic vertebral compression fracture: A prospective, controlled study. J. Orthop. Surg. Res. 2021, 16, 326. [Google Scholar] [CrossRef] [PubMed]
- Uhl, J.F.; Sufianov, A.; Ruiz, C.; Iakimov, Y.; Mogorron, H.J.; Encarnacion Ramirez, M.; Prat, G.; Lorea, B.; Baldoncini, M.; Goncharov, E.; et al. The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education. Brain Sci. 2023, 13, 894. [Google Scholar] [CrossRef]
- Ostaș, D.; Almășan, O.; Ileșan, R.R.; Andrei, V.; Thieringer, F.M.; Hedeșiu, M.; Rotar, H. Point-of-Care Virtual Surgical Planning and 3D Printing in Oral and Cranio-Maxillofacial Surgery: A Narrative Review. J. Clin. Med. 2022, 11, 6625. [Google Scholar] [CrossRef]
- Chamo, D.; Msallem, B.; Sharma, N.; Aghlmandi, S.; Kunz, C.; Thieringer, F.M. Accuracy Assessment of Molded, Patient-Specific Polymethylmethacrylate Craniofacial Implants Compared to Their 3D Printed Originals. J. Clin. Med. 2020, 9, 832. [Google Scholar] [CrossRef]
- Mee, H.; Anwar, F.; Timofeev, I.; Owens, N.; Grieve, K.; Whiting, G.; Alexander, K.; Kendrick, K.; Helmy, A.; Hutchinson, P.; et al. Cranioplasty: A Multidisciplinary Approach. Front. Surg. 2022, 9, 864385. [Google Scholar] [CrossRef]
- Gordon, C.R.; Fisher, M.; Liauw, J.A.; Lina, I.A.; Puvanesarajah, V.; Susarla, S.M.; Coon, A.L.; Lim, M.; Quiñones-Hinojosa, A.; Weingart, J.D.; et al. Multidisciplinary Approach for Improved Outcomes in Secondary Cranial Reconstruction: Introducing the Pericranial-Onlay Cranioplasty Technique. Neurosurgery 2014, 10, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Ghani, W.M.A. Cranioplasty with polymethyl methacrylate implant: Solutions of pitfalls. Egypt. J. Neurosurg. 2018, 33, 7. [Google Scholar] [CrossRef]
- Primalani, N.K.; Chew, K.Y.; Ramachandran, S.; Ng, L.P.; Low, D.C.Y.; Seow, W.T.; Low, S.Y.Y. Paediatric cranioplasty—Experience from a Singapore children’s hospital. Interdiscip. Neurosurg. 2022, 30, 101606. [Google Scholar] [CrossRef]
- De la Torre-Díez, I.; López-Coronado, M.; Vaca, C.; Aguado, J.S.; de Castro, C. Cost-utility and cost-effectiveness studies of telemedicine, electronic, and mobile health systems in the literature: A systematic review. Telemed. J. E-Health 2015, 21, 81–85. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Vijayaraghavan, S.; Wherton, J.; Shaw, S.; Byrne, E.; Campbell-Richards, D.; Bhattacharya, S.; Hanson, P.; Ramoutar, S.; Gutteridge, C.; et al. Virtual online consultations: Advantages and limitations (VOCAL) study. BMJ Open 2016, 6, e009388. [Google Scholar] [CrossRef] [PubMed]
- Maricevich, J.; Cezar-Junior, A.B.; de Oliveira-Junior, E.X.; Veras, E.S.J.A.M.; da Silva, J.V.L.; Nunes, A.A.; Almeida, N.S.; Azevedo-Filho, H.R.C. Functional and aesthetic evaluation after cranial reconstruction with polymethyl methacrylate prostheses using low-cost 3D printing templates in patients with cranial defects secondary to decompressive craniectomies: A prospective study. Surg. Neurol. Int. 2019, 10, 1. [Google Scholar] [CrossRef]
- Fischer, C.M.; Burkhardt, J.K.; Sarnthein, J.; Bernays, R.L.; Bozinov, O. Aesthetic outcome in patients after polymethyl-methacrylate (PMMA) cranioplasty—A questionnaire-based single-centre study. Neurol. Res. 2012, 34, 281–285. [Google Scholar] [CrossRef]
- Huang, Y.-H.; Lee, T.-C.; Yang, K.-Y.; Liao, C.-C. Is timing of cranioplasty following posttraumatic craniectomy related to neurological outcome? Int. J. Surg. 2013, 11, 886–890. [Google Scholar] [CrossRef]
- Tomenson, J.A.; Bonner, S.M.; Edwards, J.C.; Pemberton, M.A.; Cummings, T.F.; Paddle, G.M. Study of two cohorts of workers exposed to methyl methacrylate in acrylic sheet production. Occup. Environ. Med. 2000, 57, 810. [Google Scholar] [CrossRef]
- Schabowsky, C. Medical Device Material Performance Study: Polymethyl Methacrylate Safety Profile; Food and Drug Administration: Silver Spring, MD, USA, 2021.
- Kuroda, A.; Sakai, K.; Yahagi, S.; Mukawa, T.; Sato, N.; Nakamura, N.; Maezawa, D.; Masaki, H.; Banno, T.; Asakura, K. Surface Structures of Cosmetic Standard Poly Methyl Methacrylate UV Evaluation Plates and their Influence on the in vitro Evaluation of UV Protection Abilities of Cosmetic Sunscreens. J. Oleo Sci. 2019, 68, 175–182. [Google Scholar] [CrossRef]
- Frazer, R.Q.; Byron, R.T.; Osborne, P.B.; West, K.P. PMMA: An essential material in medicine and dentistry. J. Long-Term Eff. Med. Implant. 2005, 15, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Gozum, N.; Unal, E.S.; Altan-Yaycioglu, R.; Gucukoglu, A.; Ozgun, C. Visual performance of acrylic and PMMA intraocular lenses. Eye 2003, 17, 238–242. [Google Scholar] [CrossRef]
- Auffarth, G.U.; Brezin, A.; Caporossi, A.; Lafuma, A.; Mendicute, J.; Berdeaux, G.; Smith, A.F. Comparison of Nd: YAG capsulotomy rates following phacoemulsification with implantation of PMMA, silicone, or acrylic intra-ocular lenses in four European countries. Ophthalmic Epidemiol. 2004, 11, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.H.; Bhat, S.N.; Mamatha, H. Outcome analysis of antibiotic-loaded poly methyl methacrylate (PMMA) beads in musculoskeletal infections. J. Taibah Univ. Med. Sci. 2021, 16, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, T.A.G.; Arts, J.J.; Geurts, J.A.P. Antibiotic-Loaded Polymethylmethacrylate Beads and Spacers in Treatment of Orthopedic Infections and the Role of Biofilm Formation. Front. Microbiol. 2019, 10, 1626. [Google Scholar] [CrossRef]
- Von Hertzberg-Boelch, S.P.; Luedemann, M.; Rudert, M.; Steinert, A.F. PMMA Bone Cement: Antibiotic Elution and Mechanical Properties in the Context of Clinical Use. Biomedicines 2022, 10, 1830. [Google Scholar] [CrossRef]
- Lunz, A.; Knappe, K.; Omlor, G.W.; Schonhoff, M.; Renkawitz, T.; Jaeger, S. Mechanical strength of antibiotic-loaded PMMA spacers in two-stage revision surgery. BMC Musculoskelet. Disord. 2022, 23, 945. [Google Scholar] [CrossRef]
- Wall, V.; Nguyen, T.-H.; Nguyen, N.; Tran, P.A. Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement. Biomedicines 2021, 9, 26. [Google Scholar] [CrossRef]
- Cyphert, E.L.; Zhang, N.; Marques, D.W.; Learn, G.D.; Zhang, F.; von Recum, H.A. Poly(methyl methacrylate) Bone Cement Composite Can Be Refilled with Antibiotics after Implantation in Femur or Soft Tissue. J. Funct. Biomater. 2021, 12, 8. [Google Scholar] [CrossRef]
- Zore, A.; Abram, A.; Učakar, A.; Godina, I.; Rojko, F.; Štukelj, R.; Škapin, A.S.; Vidrih, R.; Dolic, O.; Veselinovic, V.; et al. Antibacterial Effect of Polymethyl Methacrylate Resin Base Containing TiO2 Nanoparticles. Coatings 2022, 12, 1757. [Google Scholar] [CrossRef]
- Glazkova, E.; Bakina, O.; Rodkevich, N.; Mosunov, A.; Evstigneev, M.; Evstigneev, V.; Klimenko, V.; Lerner, M. Antibacterial Properties of PMMA Functionalized with CuFe2O4/Cu2O/CuO Nanoparticles. Coatings 2022, 12, 957. [Google Scholar] [CrossRef]
- Anderson, G.M.; Osorio, C.; Berns, E.M.; Masood, U.; Alsoof, D.; McDonald, C.L.; Zhang, A.S.; Younghein, J.A.; Kuris, E.O.; Telfeian, A.; et al. Antibiotic Cement Utilization for the Prophylaxis and Treatment of Infections in Spine Surgery: Basic Science Principles and Rationale for Clinical Use. J. Clin. Med. 2022, 11, 3481. [Google Scholar] [CrossRef] [PubMed]
- Balato, M.; Petrarca, C.; Quercia, A.; Riccio, A.; Sellitto, A.; Campi, J.; Borriello, A.; Zarrelli, M.; Balato, G. A Customized Knee Antibiotic-Loaded PMMA Spacer: A Preliminary Design Analysis. Polymers 2021, 13, 4065. [Google Scholar] [CrossRef] [PubMed]
- Unterhofer, C.; Wipplinger, C.; Verius, M.; Recheis, W.; Thomé, C.; Ortler, M. Reconstruction of large cranial defects with poly-methyl-methacrylate (PMMA) using a rapid prototyping model and a new technique for intraoperative implant modeling. Neurol. Neurochir. Pol. 2017, 51, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Andrabi, S.M.; Sarmast, A.H.; Kirmani, A.R.; Bhat, A.R. Cranioplasty: Indications, procedures, and outcome—An institutional experience. Surg. Neurol. Int. 2017, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-M.; Park, T.; Lee, S.-P.; Baek, J.-W.; Ryou, K.-S.; Kim, S.-H. Optimal Timing and Complications of Cranioplasty: A Single-Center Retrospective Review of 109 Cases. J. Neurointensive Care 2020, 3, 48–57. [Google Scholar] [CrossRef]
- Sobani, Z.A.; Shamim, M.S.; Zafar, S.N.; Qadeer, M.; Bilal, N.; Murtaza, S.G.; Enam, S.A.; Bari, M.E. Cranioplasty after decompressive craniectomy: An institutional audit and analysis of factors related to complications. Surg. Neurol. Int. 2011, 2, 123. [Google Scholar] [CrossRef]
- Jung, Y.T.; Lee, S.P.; Cho, J.I. An Improved One-Stage Operation of Cranioplasty and Ventriculoperitoneal Shunt in Patient with Hydrocephalus and Large Cranial Defect. Korean J. Neurotrauma 2015, 11, 93–99. [Google Scholar] [CrossRef]
- Bot, G.M.; Ismail, N.J.; Usman, B.; Shilong, D.J.; Obande, J.O.; Aliu, S.; Sale, D.; Shehu, B.B. Using the head as a mould for cranioplasty with methylmethacrylate. J. Neurosci. Rural Pract. 2013, 4, 471–474. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | 1 | 2 | 3 |
|---|---|---|---|
| Age | 19 | 24 | 49 |
| Years | Male | Male | Female |
| Cause | SDH, TBI caused by falling from a height of 7 m | TBI caused by falling from the roof of a house from a height of 4–5 m | Cranial decompression due to surgery of ACM aneurysm |
| Anamnestic data | Treated surgically 3 years b.c. in another facility due to previously explained injury | Treated surgically two years ago in our facility, epidural empyema without isolating the pathogen a year ago | Treated three years b.c. in another facility (and state) due to MCA aneurysm, present hemiparesis of the left side, as well as paresis of the right oculomotor and facial nerve |
| Defect size | 119.8 mm × 52.8 mm (63.3 cm2) | 121.0 mm × 89.5 mm (108.3 cm2) | 102.2 mm × 68.1 mm (69.6 cm2) |
| Side | Left | Right | Left |
| Localisation | Frontal, parietal and temporal bone included | Frontal, parietal and temporal bone included | Frontal and temporal bone included |
| Poukens et al. [15] classification | II | III | II |
| Time to CP (months) | 36 | 12 | 36 |
| Operation time | 120 | 140 | 145 |
| Hospitalisation days | 5 | 11 | 31 |
| Comorbidities | None | None | Status after MCA occlusion |
| Outcome | Functional and aesthetic improvement | Functional and aesthetic improvement | Functional and aesthetic improvement |
| Case | 1 | 2 | 3 |
|---|---|---|---|
| Material costs | USD 99 | USD 90 | USD 90 |
| Technical processing costs 1 | USD 395 | USD 395 | USD 400 |
| Total costs material and processing costs | USD 494 | USD 485 | USD 490 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bečulić, H.; Spahić, D.; Begagić, E.; Pugonja, R.; Skomorac, R.; Jusić, A.; Selimović, E.; Mašović, A.; Pojskić, M. Breaking Barriers in Cranioplasty: 3D Printing in Low and Middle-Income Settings—Insights from Zenica, Bosnia and Herzegovina. Medicina 2023, 59, 1732. https://doi.org/10.3390/medicina59101732
Bečulić H, Spahić D, Begagić E, Pugonja R, Skomorac R, Jusić A, Selimović E, Mašović A, Pojskić M. Breaking Barriers in Cranioplasty: 3D Printing in Low and Middle-Income Settings—Insights from Zenica, Bosnia and Herzegovina. Medicina. 2023; 59(10):1732. https://doi.org/10.3390/medicina59101732
Chicago/Turabian StyleBečulić, Hakija, Denis Spahić, Emir Begagić, Ragib Pugonja, Rasim Skomorac, Aldin Jusić, Edin Selimović, Anes Mašović, and Mirza Pojskić. 2023. "Breaking Barriers in Cranioplasty: 3D Printing in Low and Middle-Income Settings—Insights from Zenica, Bosnia and Herzegovina" Medicina 59, no. 10: 1732. https://doi.org/10.3390/medicina59101732