
Effect of C-Clamp Application on Hemodynamic Instability in Polytrauma Victims with Pelvic Fracture
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Assessment of Hemodynamic Stabilization
2.3. Statistical Analysis
3. Results
3.1. Patients
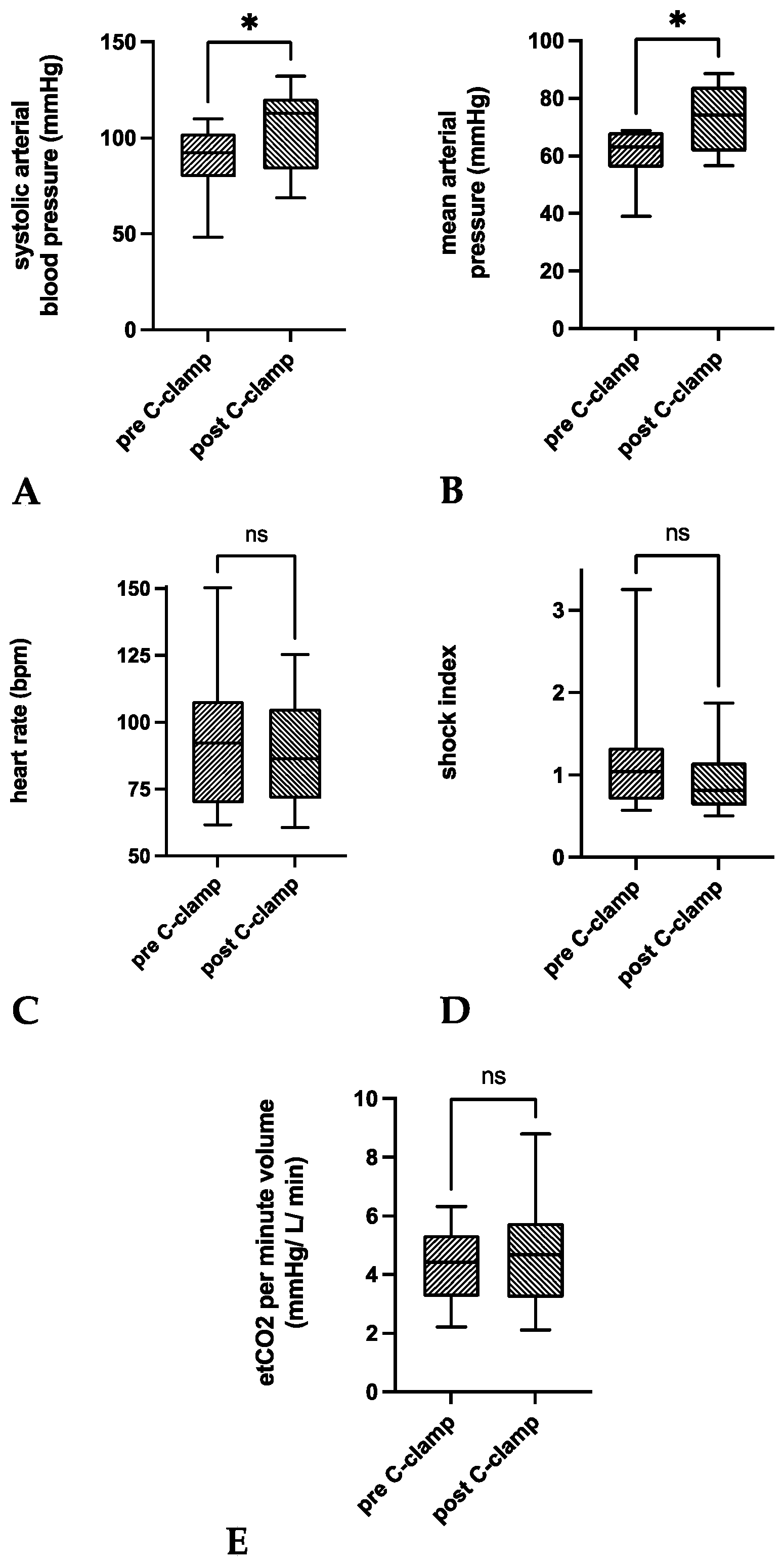
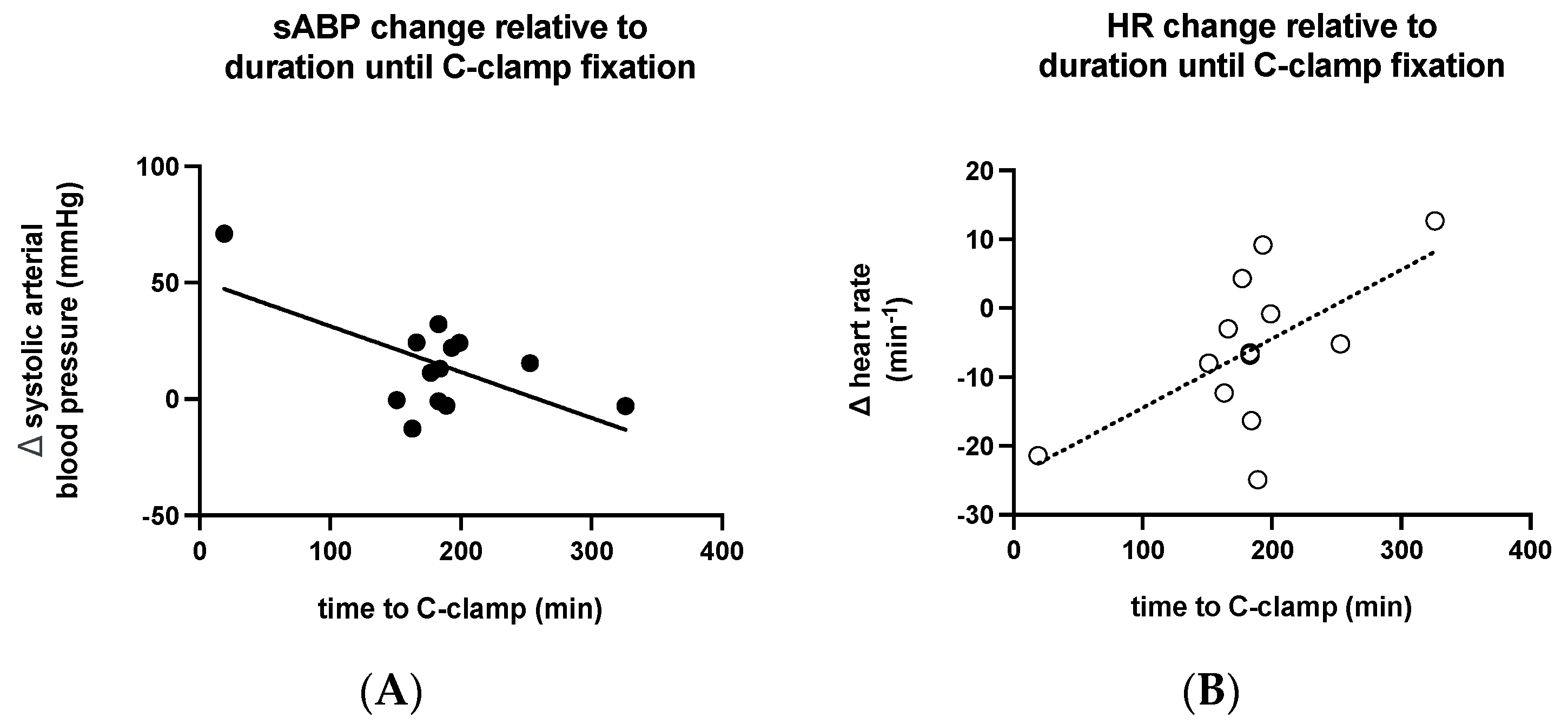
3.2. Vital Parameters
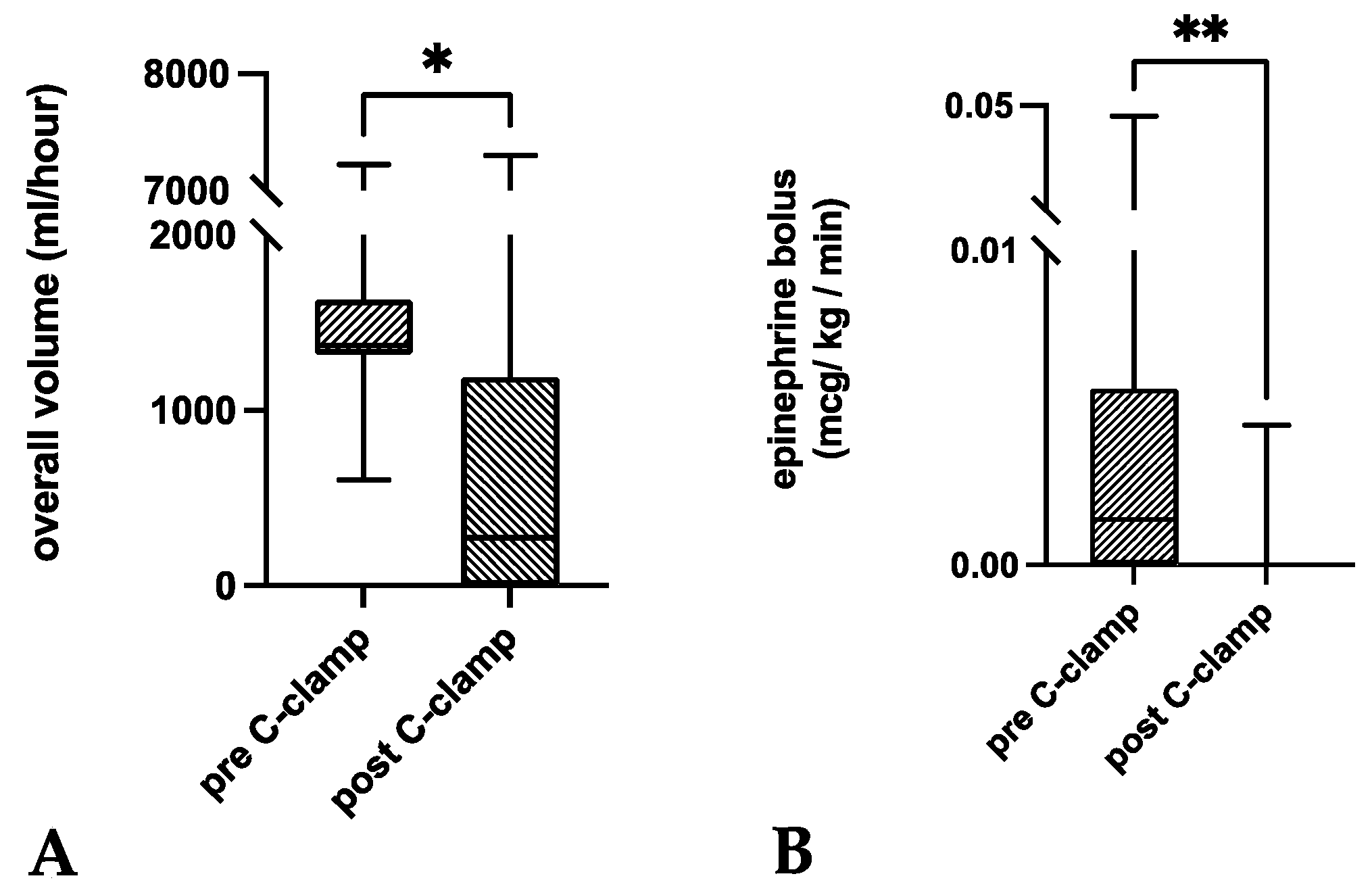
3.3. Metabolic Indices and Volume Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ganz, R.; Krushell, R.J.; Jakob, R.P.; Küffer, J. The antishock pelvic clamp. Clin. Orthop. Relat. Res. 1991, 267, 71–78. [Google Scholar] [CrossRef]
- Pohlemann, T.; Culemann, U.; Gänsslen, A.; Tscherne, H. Severe pelvic injury with pelvic mass hemorrhage: Determining severity of hemorrhage and clinical experience with emergency stabilization. Unfallchirurg 1996, 99, 734–743. [Google Scholar] [CrossRef] [PubMed]
- Heini, P.F.; Witt, J.; Ganz, R. The pelvic C-clamp for the emergency treatment of unstable pelvic ring injuries. A report on clinical experience of 30 cases. Injury 1996, 27 (Suppl. 1), 38–45. [Google Scholar] [CrossRef]
- Tscherne, H.; Pohlemann, T.; Gänsslen, A.; Hüfner, T.; Pape, H.C. Crush injuries of the pelvis. Eur. J. Surg. 2000, 166, 276–282. [Google Scholar] [CrossRef]
- Hauschild, O.; Strohm, P.C.; Culemann, U.; Pohlemann, T.; Suedkamp, N.P.; Koestler, W.; Schmal, H. Mortality in patients with pelvic fractures: Results from the German pelvic injury register. J. Trauma Acute Care Surg. 2008, 64, 449–455. [Google Scholar] [CrossRef]
- Schmal, H.; Larsen, M.S.; Stuby, F.; Strohm, P.C.; Reising, K.; Goodwin Burri, K. Effectiveness and complications of primary C-clamp stabilization or external fixation for unstable pelvic fractures. Injury 2019, 50, 1959–1965. [Google Scholar] [CrossRef]
- Höch, A.; Zeidler, S.; Pieroh, P.; Josten, C.; Stuby, F.M.; Herath, S.C. Trends and efficacy of external emergency stabilization of pelvic ring fractures: Results from the German Pelvic Trauma Registry. Eur. J. Trauma Emerg. Surg. 2021, 47, 523–531. [Google Scholar] [CrossRef]
- Gewiess, J.; Albers, C.E.; Pape, H.C.; Bangerter, H.; Zech, W.D.; Keel, M.J.B.; Bastian, J.D. Characteristics of Prehospital Death in Trauma Victims. J. Clin. Med. 2021, 10, 4765. [Google Scholar] [CrossRef]
- Hak, D.J.; Smith, W.R.; Suzuki, T. Management of hemorrhage in life-threatening pelvic fracture. J. Am. Acad. Orthop. Surg. 2009, 17, 447–457. [Google Scholar] [CrossRef]
- Starr, A.J.; Griffin, D.R.; Reinert, C.M.; Frawley, W.H.; Walker, J.; Whitlock, S.N.; Borer, D.S.; Rao, A.V.; Jones, A.L. Pelvic ring disruptions: Prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J. Orthop. Trauma 2002, 16, 553–561. [Google Scholar] [CrossRef]
- Gänsslen, A.; Hildebrand, F.; Pohlemann, T. Management of hemodynamic unstable patients “in extremis” with pelvic ring fractures. Acta Chir. Orthop. Traumatol. Cech. 2012, 79, 193–202. [Google Scholar] [PubMed]
- Gilliland, M.D.; Ward, R.E.; Barton, R.M.; Miller, P.W.; Duke, J.H. Factors affecting mortality in pelvic fractures. J. Trauma 1982, 22, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Collicott, P.E.; Hughes, I. Training in Advanced Trauma Life Support. JAMA 1980, 243, 1156–1159. [Google Scholar] [CrossRef] [PubMed]
- Lustenberger, T.; Meier, C.; Benninger, E.; Lenzlinger, P.M.; Keel, M.J.B. C-clamp and pelvic packing for control of hemorrhage in patients with pelvic ring disruption. J. Emerg. Trauma Shock 2011, 4, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Tiemann, A.H.; Schmidt, C.; Gonschorek, O.; Josten, C. Use of the “c-clamp” in the emergency treatment of unstable pelvic fractures. Zentralbl Chir. 2004, 129, 245–251. [Google Scholar] [CrossRef]
- Thannheimer, A.; Woltmann, A.; Vastmans, J.; Bühren, V. The unstable patient with pelvic fracture. Zentralbl Chir. 2004, 129, 37–42. [Google Scholar] [CrossRef]
- Gupta, B.; Garg, N.; Ramachandran, R. Vasopressors: Do they have any role in hemorrhagic shock? J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 3–8. [Google Scholar] [CrossRef]
- Bangash, M.N.; Kong, M.L.; Pearse, R.M. Use of inotropes and vasopressor agents in critically ill patients. Br. J. Pharmacol. 2012, 165, 2015–2033. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008, 36, 296–327. [Google Scholar] [CrossRef]
- Ertel, W.; Keel, M.; Eid, K.; Platz, A.; Trentz, O. Control of severe hemorrhage using C-clamp and pelvic packing in multiply injured patients with pelvic ring disruption. J. Orthop. Trauma 2001, 15, 468–474. [Google Scholar] [CrossRef]
- Witschger, P.; Heini, P.; Ganz, R. Pelvic clamps for controlling shock in posterior pelvic ring injuries. Application, biomechanical aspects and initial clinical results. Orthopade 1992, 21, 393–399. [Google Scholar] [PubMed]
- Pohlemann, T.; Krettek, C.; Hoffmann, R.; Culemann, U.; Gänsslen, A. Biomechanical comparison of various emergency stabilization measures of the pelvic ring. Unfallchirurg 1994, 97, 503–510. [Google Scholar]
- Ghanayem, A.J.; Stover, M.D.; Goldstein, J.A.; Bellon, E.; Wilber, J.H. Emergent treatment of pelvic fractures. Comparison of methods for stabilization. Clin. Orthop. Relat. Res. 1995, 318, 75–80. [Google Scholar]
- Kellam, J.F. The role of external fixation in pelvic disruptions. Clin. Orthop. Relat. Res. 1989, 241, 66–82. [Google Scholar] [CrossRef]
- Richard, M.J.; Tornetta, P., 3rd. Emergent management of APC-2 pelvic ring injuries with an anteriorly placed C-clamp. J. Orthop. Trauma 2009, 23, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Horer, T.M.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R.; et al. Pelvic trauma: WSES classification and guidelines. World J. Emerg. Surg. 2017, 12, 5. [Google Scholar] [CrossRef]
- Loggers, S.A.I.; Koedam, T.W.A.; Giannakopoulos, G.F.; Vandewalle, E.; Erwteman, M.; Zuidema, W.P. Definition of hemodynamic stability in blunt trauma patients: A systematic review and assessment amongst Dutch trauma team members. Eur. J. Trauma Emerg. Surg. 2017, 43, 823–833. [Google Scholar] [CrossRef]
- Abt, R.; Lustenberger, T.; Stover, J.F.; Benninger, E.; Lenzlinger, P.M.; Stocker, R.; Keel, M. Base excess determined within one hour of admission predicts mortality in patients with severe pelvic fractures and severe hemorrhagic shock. Eur. J. Trauma Emerg. Surg. 2009, 35, 429. [Google Scholar] [CrossRef]
- Saito, S.; Kadoi, Y.; Nihishara, F.; Aso, C.; Goto, F. End-tidal carbon dioxide monitoring stabilized hemodynamic changes during ECT. J. ECT 2003, 19, 26–30. [Google Scholar] [CrossRef]
- von Planta, M.; Weil, M.H.; Gazmuri, R.J. Noninvasive assessment of hemodynamics during resuscitation using capnography. Schweiz. Med. Wochenschr. 1989, 119, 371–375. [Google Scholar]
- Paladino, L.; Sinert, R.; Wallace, D.; Anderson, T.; Yadav, K.; Zehtabchi, S. The utility of base deficit and arterial lactate in differentiating major from minor injury in trauma patients with normal vital signs. Resuscitation 2008, 77, 363–368. [Google Scholar] [CrossRef]
- Barmparas, G.; Dhillon, N.K.; Smith, E.J.; Mason, R.; Melo, N.; Thomsen, G.M.; Margulies, D.R.; Ley, E.J. Patterns of vasopressor utilization during the resuscitation of massively transfused trauma patients. Injury 2018, 49, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Uchida, K.; Nishimura, T.; Hagawa, N.; Kaga, S.; Noda, T.; Shinyama, N.; Yamamoto, H.; Mizobata, Y. The impact of early administration of vasopressor agents for the resuscitation of severe hemorrhagic shock following blunt trauma. BMC Emerg. Med. 2020, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Schütz, M.; Stöckle, U.; Hoffmann, R.; Südkamp, N.; Haas, N. Clinical experience with two types of pelvic C-clamps for unstable pelvic ring injuries. Injury 1996, 27 (Suppl. 1), 46–50. [Google Scholar] [CrossRef]
- Sadri, H.; Nguyen-Tang, T.; Stern, R.; Hoffmeyer, P.; Peter, R. Control of severe hemorrhage using C-clamp and arterial embolization in hemodynamically unstable patients with pelvic ring disruption. Arch. Orthop. Trauma Surg. 2005, 125, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Esmer, E.; Esmer, E.; Derst, P.; Schulz, M.; Siekmann, H.; Delank, K.S. Influence of external pelvic stabilization on hemodynamically unstable pelvic fractures. Unfallchirurg 2017, 120, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Audretsch, C.K.; Mader, D.; Bahrs, C.; Trulson, A.; Höch, A.; Herath, S.C.; Küper, M.A. Comparison of pelvic C-clamp and pelvic binder for emergency stabilization and bleeding control in type-C pelvic ring fractures. Sci. Rep. 2021, 11, 2338. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Hofmann, A.; Hessmann, M.H. Management of Acute Hemorrhage in Pelvic Trauma: An Overview. Eur. J. Trauma Emerg. Surg. 2010, 36, 91–99. [Google Scholar] [CrossRef]
- Gänsslen, A.; Giannoudis, P.; Pape, H.C. Hemorrhage in pelvic fracture: Who needs angiography? Curr. Opin. Crit. Care 2003, 9, 515–523. [Google Scholar] [CrossRef]
- Marzi, I.; Lustenberger, T. Management of Bleeding Pelvic Fractures. Scand. J. Surg. 2014, 103, 104–111. [Google Scholar] [CrossRef]
- Tosounidis, T.I.; Giannoudis, P.V. Pelvic fractures presenting with haemodynamic instability: Treatment options and outcomes. Surgeon 2013, 11, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Sellei, R.M.; Schandelmaier, P.; Kobbe, P.; Knobe, M.; Pape, H.C. Can a modified anterior external fixator provide posterior compression of AP compression type III pelvic injuries? Clin. Orthop. Relat. Res. 2013, 471, 2862–2868. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, A.J.; Davies, K.; Ramesh, B.; O’Kelly, A.; Rajagopal, R. Haemorrhage control in pelvic fractures--a survey of surgical capabilities. Injury 2011, 42, 1008–1011. [Google Scholar] [CrossRef]
- Koller, H.; Keil, P.; Seibert, F. Individual and team training with first time users of the Pelvic C-Clamp: Do they remember or will we need refresher trainings? Arch. Orthop. Trauma Surg. 2013, 133, 343–349. [Google Scholar] [CrossRef]
- Schweigkofler, U.; Wincheringer, D.; Holstein, J.; Fritz, T.; Hoffmann, R.; Pohlemann, T.; Herath, S.C. How effective are different models of pelvic binders: Results of a study using a Pelvic Emergency Simulator. Eur. J. Trauma Emerg. Surg. 2022, 48, 847–855. [Google Scholar] [CrossRef]
- Abominal and Pelvic Trauma, in Advanced Trauma Life Support® Student Course Manual; American College of Surgeons: Chicago, IL, USA, 2018; pp. 82–101.
- Hsu, S.D.; Chen, C.J.; Chou, Y.C.; Wang, S.H.; Chan, D.C. Effect of Early Pelvic Binder Use in the Emergency Management of Suspected Pelvic Trauma: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1217. [Google Scholar] [CrossRef]
- Jowett, A.J.; Bowyer, G.W. Pressure characteristics of pelv.vic binders. Injury 2007, 38, 118–121. [Google Scholar] [CrossRef]
- Kuner, V.; van Veelen, N.; Studer, S.; Van de Wall, B.; Fornaro, J.; Stickel, M.; Knobe, M.; Babst, R.; Beeres, F.J.P.; Link, B.C. Application of Pelvic Circumferential Compression Devices in Pelvic Ring Fractures-Are Guidelines Followed in Daily Practice? J. Clin. Med. 2021, 10, 1297. [Google Scholar] [CrossRef]
- Marmor, M.; El Naga, A.N.; Barker, J.; Matz, J.; Stergiadou, S.; Miclau, T. Management of Pelvic Ring Injury Patients with Hemodynamic Instability. Front. Surg. 2020, 7, 588845. [Google Scholar] [CrossRef]
- Özkurtul, O.; Staab, H.; Osterhoff, G.; Ondruschka, B.; Höch, A.; Josten, C.; Fakler, J.K.M. Technical limitations of REBOA in a patient with exsanguinating pelvic crush trauma: A case report. Patient Saf. Surg. 2019, 13, 25. [Google Scholar] [CrossRef]
- Abrassart, S.; Stern, R.; Peter, R. Unstable pelvic ring injury with hemodynamic instability: What seems the best procedure choice and sequence in the initial management? Orthop. Traumatol. Surg. Res. 2013, 99, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, J.; Höll, S.; Kälicke, T.; Muhr, G.; Kutscha-Lissberg, F. Die offene Beckenfraktur. Unfallchirurg 2004, 107, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Dilogo, I.H.; Prabowo, I. The role of angioembolization and C-clamp fixation: Damaged control orthopaedic in haemodynamically unstable pelvic fracture. Ann. Med. Surg. 2021, 63, 102157. [Google Scholar] [CrossRef] [PubMed]
- Pizanis, A.; Pohlemann, T.; Burkhardt, M.; Aghayev, E.; Holstein, J.H. Emergency stabilization of the pelvic ring: Clinical comparison between three different techniques. Injury 2013, 44, 1760–1764. [Google Scholar] [CrossRef] [PubMed]
- Buitenwerf, E.; Boekel, M.F.; van der Velde, M.I.; Voogd, M.F.; Kerstens, M.N.; Wietasch, G.J.K.G.; Scheeren, T.W.L. The haemodynamic instability score: Development and internal validation of a new rating method of intra-operative haemodynamic instability. Eur. J. Anaesthesiol. 2019, 36, 290–296. [Google Scholar] [CrossRef]
- Mucha, P., Jr.; Welch, T.J. Hemorrhage in major pelvic fractures. Surg. Clin. N. Am. 1988, 68, 757–773. [Google Scholar] [CrossRef]
- Hooper, N.; Armstrong, T.J. Hemorrhagic Shock; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tiemann, A.H.; Böhme, J.; Josten, C. Emergency Treatment of Multiply Injured Patients with Unstable Disruption of the Posterior Pelvic Ring by Using the “C–Clamp”. Eur. J. Trauma 2005, 31, 244–251. [Google Scholar] [CrossRef]
- Sandroni, C.; De Santis, P.; D’Arrigo, S. Capnography during cardiac arrest. Resuscitation 2018, 132, 73–77. [Google Scholar] [CrossRef]
- Bruns, B.; Lindsey, M.; Rowe, K.; Brown, S.; Minei, J.P.; Gentilello, L.M.; Shafi, S. Hemoglobin drops within minutes of injuries and predicts need for an intervention to stop hemorrhage. J. Trauma 2007, 63, 312–315. [Google Scholar] [CrossRef]
- Maegele, M.; Lefering, R.; Yucel, N.; Tjardes, T.; Rixen, D.; Paffrath, T.; Simanski, C.; Neugebauer, E.; Bouillon, B. Early coagulopathy in multiple injury: An analysis from the German Trauma Registry on 8724 patients. Injury 2007, 38, 298–304. [Google Scholar] [CrossRef]
- Richards, J.E.; Harris, T.; Dünser, M.W.; Bouzat, P.; Gauss, T. Vasopressors in Trauma: A Never Event? Anesth. Analg. 2021, 133, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Beloncle, F.; Meziani, F.; Lerolle, N.; Radermacher, P.; Asfar, P. Does vasopressor therapy have an indication in hemorrhagic shock? Ann. Intensive Care 2013, 3, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age | Gender | ISS | Trauma Mechanism | Young/Burgess Type |
|---|---|---|---|---|---|
| 1 | 31 | m | 54 | fall from height | VC |
| 2 | 51 | f | 38 | MVA | VC |
| 3 | 27 | m | 38 | fall from height | VC |
| 4 | 28 | m | 50 | fall from height | VC |
| 5 | 53 | m | 33 | fall from height | VC |
| 6 | 39 | f | 29 | MVA | APCIII |
| 7 | 42 | m | 45 | other | LCIII |
| 8 † | 69 | m | 38 | fall from height | VC |
| 9 | 60 | f | 43 | MVA | LCIII |
| 10 † | 64 | m | 75 | MVA | APCIII |
| 11 | 40 | m | 50 | fall from height | VC |
| 12 | 74 | m | 66 | MVA | VC |
| 13 † | 74 | f | 29 | MVA | APCII |
| mean ± SD | 50.2 ± 17 | 45.2 ± 13.8 |
| ID | ΔsABP (mmHg) | ΔMAP (mmHg) | ΔHR (min−1) | ΔSI | ΔetCO2/RMV (mmHg/L/min) |
|---|---|---|---|---|---|
| 1 | −13 | −11 | −12 | 0.0 | −0.2 |
| 2 | 32 | 34 | −7 | −0.4 | 0.0 |
| 3 | 71 | 44 | −21 | −2.2 | 3.0 |
| 4 | 24 | 15 | −3 | −0.4 | −0.5 |
| 5 | 11 | 8 | 4 | 0.0 | 3.5 |
| 6 | −1 | 0 | −8 | −0.1 | 2.0 |
| 7 | 13 | 19 | −16 | −0.2 | −1.0 |
| 8 † | 22 | 17 | 9 | 0.0 | −0.6 |
| 9 | −1 | −2 | −7 | 0.0 | −0.1 |
| 10 † | −3 | −2 | −25 | −0.2 | −0.2 |
| 11 | 15 | 12 | −5 | −0.2 | 0.3 |
| 12 | −3 | 1 | 13 | 0.2 | −0.1 |
| 13 † | 24 | 23 | −1 | −0.2 | −0.5 |
| ID | Initial BE (mmol/L) | Time until Normalization (hh:mm) | Initial Hemoglobine (g/L) | Time until Normalization (hh:mm) | Initial Lactate (mmol/L) | Time until Normalization (hh:mm) | VS before C-Clamp (mL/h) | VS after C-Clamp (mL/h) |
|---|---|---|---|---|---|---|---|---|
| 1 | −5.7 | >12 h | 70 | >12 | 4.6 | 06:15 | 1690 | 1275 |
| 2 | −7.6 | >12 | 113 | >12 | 2.7 | >12 | 1450 | 0 |
| 3 | −20.5 | >12 | 91 | >12 | 12.3 | 11:59 | 846 | 5150 |
| 4 | −8.6 | 03:37 | 114 | >12 | 5.3 | >12 | 1317 | 250 |
| 5 | −5.7 | 00:01 | 130 | >12 | 4.4 | 00:01 | 1371 | 0 |
| 6 | −1.8 | 08:35 | 127 | >12 | 2.5 | >12 | 1757 | 0 |
| 7 | −3.4 | >12 | 136 | >12 | 1.1 | n.a. | 604 | 0 |
| 8 † | −11.4 | >12 | 117 | 01:52 | 7.2 | 01:52 | 1321 | 750 |
| 9 | −1.9 | >12 | 126 | >12 | 1.8 | n.a. | 1513 | 275 |
| 10 † | −20.4 | >12 | 106 | >12 | 13.4 | >12 | 7224 | 7300 |
| 11 | −10.5 | 00:14 | 99 | >12 | 5.8 | 00:14 | 1340 | 1100 |
| 12 | −7.6 | >12 | 107 | >12 | 8.1 | >12 | 1368 | 300 |
| 13 † | −9.2 | >12 | 109 | >12 | 1.8 | 00:59 | 1573 | 0 |
| mean ± SD | −8.8 ± 6 | 111.2 ± 17.8 | 5.5 ± 3.9 | 1798 ± 1595 | 1262 ± 2287 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gewiess, J.; Luedi, M.M.; Schnüriger, B.; Tosounidis, T.H.; Keel, M.J.B.; Bastian, J.D. Effect of C-Clamp Application on Hemodynamic Instability in Polytrauma Victims with Pelvic Fracture. Medicina 2022, 58, 1291. https://doi.org/10.3390/medicina58091291
Gewiess J, Luedi MM, Schnüriger B, Tosounidis TH, Keel MJB, Bastian JD. Effect of C-Clamp Application on Hemodynamic Instability in Polytrauma Victims with Pelvic Fracture. Medicina. 2022; 58(9):1291. https://doi.org/10.3390/medicina58091291
Chicago/Turabian StyleGewiess, Jan, Markus Martin Luedi, Beat Schnüriger, Theodoros Hercules Tosounidis, Marius Johann Baptist Keel, and Johannes Dominik Bastian. 2022. "Effect of C-Clamp Application on Hemodynamic Instability in Polytrauma Victims with Pelvic Fracture" Medicina 58, no. 9: 1291. https://doi.org/10.3390/medicina58091291