
The Prognostic Value of Optic Nerve Sheath Diameter/Eyeball Transverse Diameter Ratio in the Neurological Outcomes of Out-of-Hospital Cardiac Arrest Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
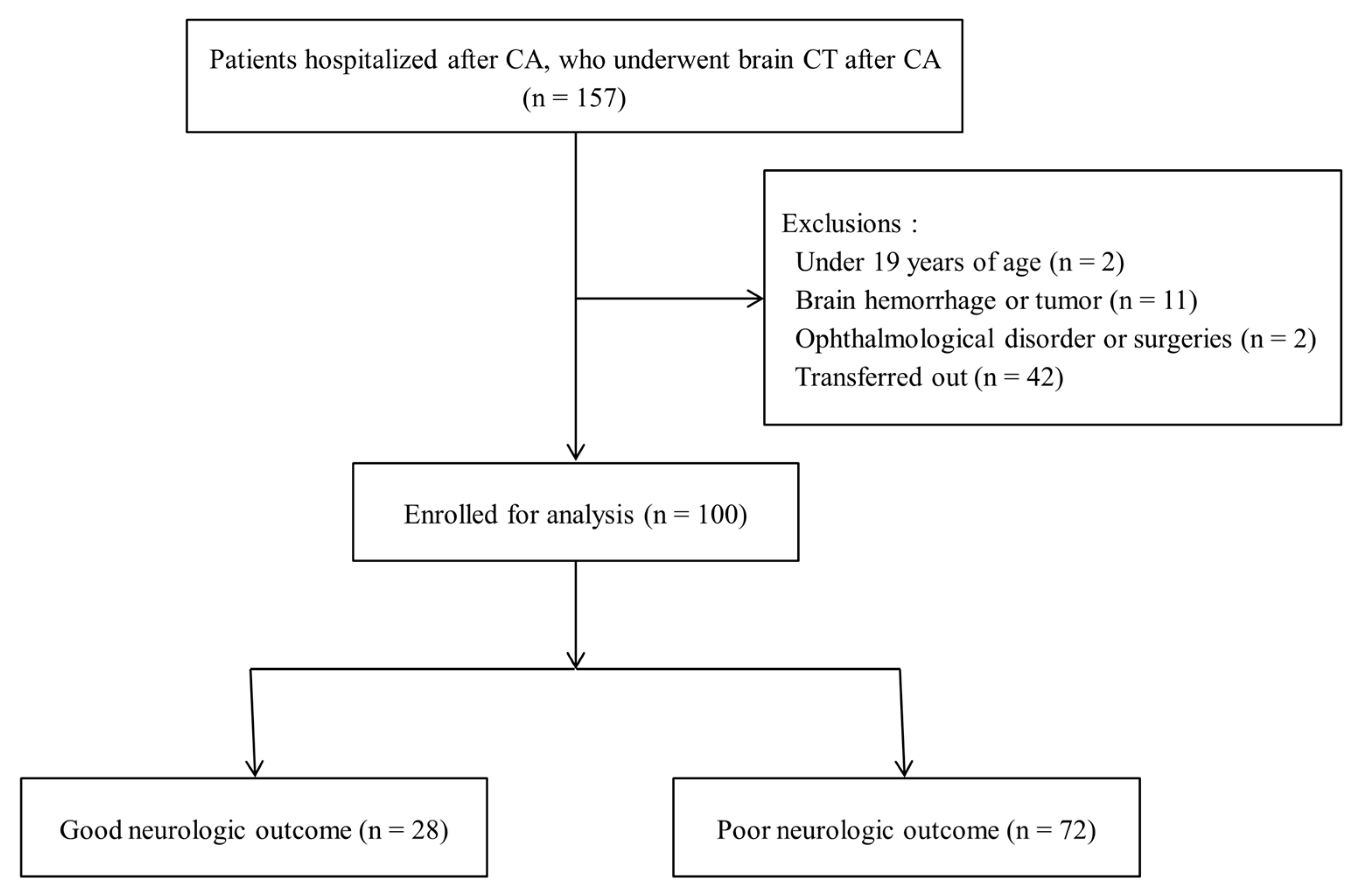
2.2. Participants
2.3. Data Collection
2.4. ONSD/ETD Ratio Measurements
2.5. Study Size
2.6. Statistical Methods
3. Results
3.1. Participants
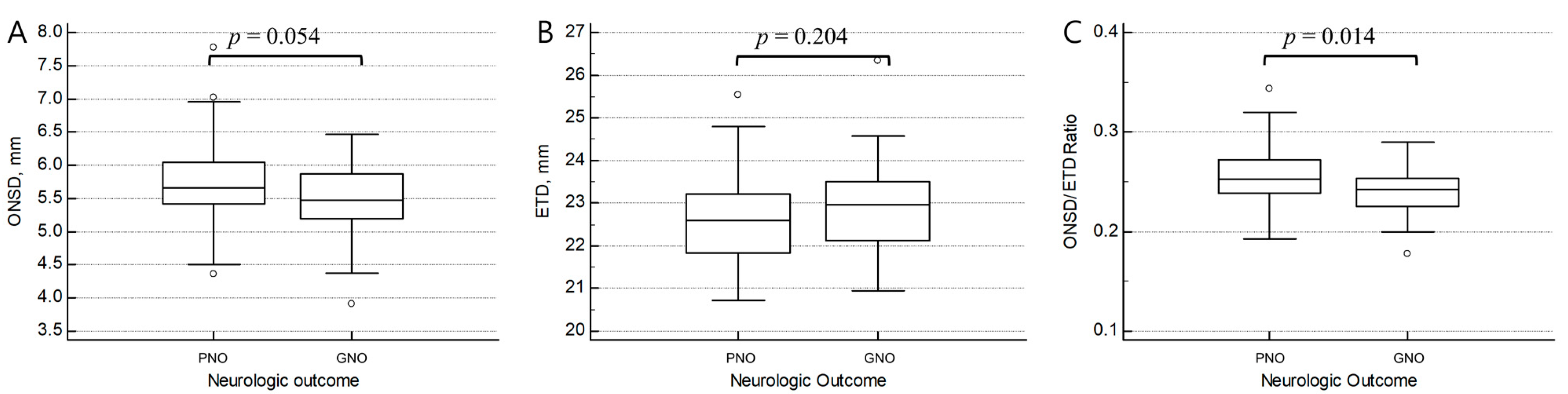
3.2. Comparison of the ONSD/ETD Ratio between GNO and PNO
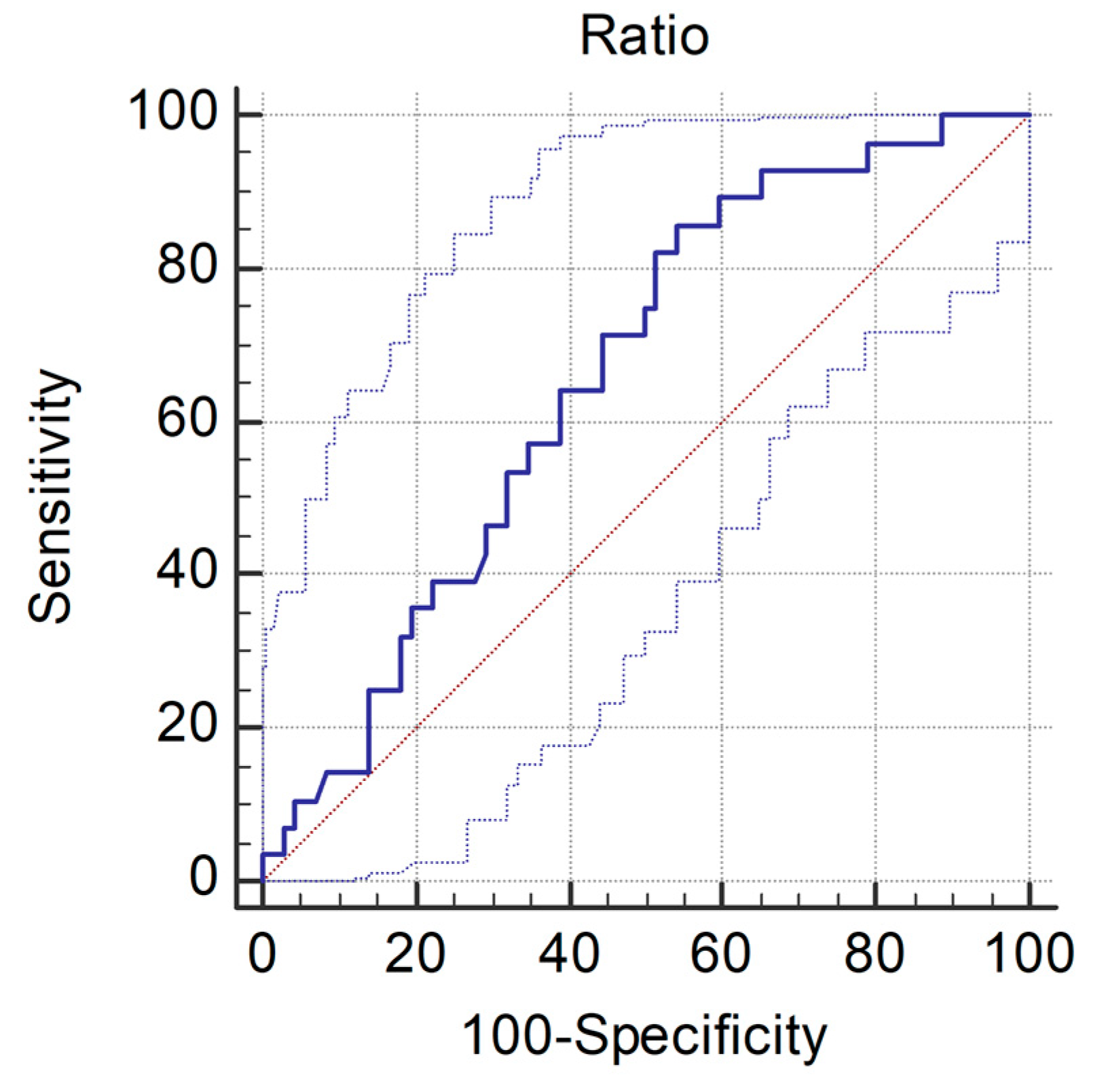
3.3. Diagnostic Value of the ONSD/ETD Ratio for Predicting the Neurologic Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gueugniaud, P.Y.; Garcia-Darennes, F.; Gaussorgues, P.; Bancalari, G.; Petit, P.; Robert, D. Prognostic Significance of Early Intracranial and Cerebral Perfusion Pressures in Post-Cardiac Arrest Anoxic Coma. Intensive Care Med. 1991, 17, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.K.; Ko, E.; Lee, J.H.; Lee, T.R.; Yoon, H.; Hwang, S.Y.; Cha, W.C.; Shin, T.G.; Sim, M.S.; Jo, I.J.; et al. Better Prognostic Value with Combined Optic Nerve Sheath Diameter and Grey-to-White Matter Ratio on Initial Brain Computed Tomography in Post-Cardiac Arrest Patients. Resuscitation 2016, 104, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Cho, Y.; You, Y.; Min, J.H.; Jeong, W.; Ahn, H.J.; Kang, C.; Yoo, I.; Ryu, S.; Lee, J.; et al. Optimal Timing to Measure Optic Nerve Sheath Diameter as a Prognostic Predictor in Post-Cardiac Arrest Patients Treated with Targeted Temperature Management. Resuscitation 2019, 143, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.; Min, J.H.; Park, J.S.; You, Y.; Yoo, I.; Cho, Y.C.; Jeong, W.; Ahn, H.J.; Ryu, S.; Lee, J.; et al. Relationship between Optic Nerve Sheath Diameter Measured by Magnetic Resonance Imaging, Intracranial Pressure, and Neurological Outcome in Cardiac Arrest Survivors Who Underwent Targeted Temperature Management. Resuscitation 2019, 145, 43–49. [Google Scholar] [CrossRef]
- Kim, J.-G.; Kim, W.; Shin, H.; Lim, T.-H.; Jang, B.-H.; Cho, Y.; Choi, K.-S.; Na, M.-K.; Ahn, C.; Lee, J. Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 500. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.; Shin, H.; Kim, C.; Choi, H.J.; Kang, B.S. Predictive Utility of Changes in Optic Nerve Sheath Diameter after Cardiac Arrest for Neurologic Outcomes. Int. J. Environ. Res. Public Health 2021, 18, 6567. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Jun, J.S.; Kim, R. Ultrasonographic Measurement of the Optic Nerve Sheath Diameter and Its Association with Eyeball Transverse Diameter in 585 Healthy Volunteers. Sci. Rep. 2017, 7, 15906. [Google Scholar] [CrossRef]
- Bekerman, I.; Sigal, T.; Kimiagar, I.; Ben Ely, A.; Vaiman, M. The Quantitative Evaluation of Intracranial Pressure by Optic Nerve Sheath Diameter/Eye Diameter CT Measurement. Am. J. Emerg. Med. 2016, 34, 2336–2342. [Google Scholar] [CrossRef]
- Dubourg, J.; Javouhey, E.; Geeraerts, T.; Messerer, M.; Kassai, B. Ultrasonography of Optic Nerve Sheath Diameter for Detection of Raised Intracranial Pressure: A Systematic Review and Meta-Analysis. Intensive Care Med. 2011, 37, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Santori, G.; Czosnyka, M.; Corradi, F.; Bragazzi, N.; Padayachy, L.; Taccone, F.S.; Citerio, G. Optic Nerve Sheath Diameter Measured Sonographically as Non-Invasive Estimator of Intracranial Pressure: A Systematic Review and Meta-Analysis. Intensive Care Med. 2018, 44, 1284–1294. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.C.E.; Kan, P.; Klimo, P.; Brockmeyer, D.L.; Walker, M.L.; Kestle, J.R.W. Complications of Intracranial Pressure Monitoring in Children with Head Trauma. J. Neurosurg. 2004, 101, 53–58. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Griesdale, D.E.; Robba, C.; McGlashan, N.; Needham, E.; Walland, K.; Shook, A.C.; Smielewski, P.; Czosnyka, M.; Gupta, A.K.; et al. Optic Nerve Sheath Diameter on Computed Tomography Is Correlated with Simultaneously Measured Intracranial Pressure in Patients with Severe Traumatic Brain Injury. Intensive Care Med. 2014, 40, 1267–1274. [Google Scholar] [CrossRef]
- Lee, S.H.; Jong Yun, S. Diagnostic Performance of Optic Nerve Sheath Diameter for Predicting Neurologic Outcome in Post-Cardiac Arrest Patients: A Systematic Review and Meta-Analysis. Resuscitation 2019, 138, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.W.; Zhang, S.; Gao, H.; Li, C.; Zhang, M.X. Prognostic Role of Optic Nerve Sheath Diameter for Neurological Outcomes in Post-Cardiac Arrest Patients: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2020, 2020, 5219367. [Google Scholar] [CrossRef]
- Kim, Y.H.; Lee, J.H.; Hong, C.K.; Cho, K.W.; Yeo, J.H.; Kang, M.J.; Kim, Y.W.; Lee, K.Y.; Kim, J.J.; Hwang, S.Y. Feasibility of Optic Nerve Sheath Diameter Measured on Initial Brain Computed Tomography as an Early Neurologic Outcome Predictor after Cardiac Arrest. Acad. Emerg. Med. 2014, 21, 1121–1128. [Google Scholar] [CrossRef]
- Chelly, J.; Deye, N.; Guichard, J.P.; Vodovar, D.; Vong, L.; Jochmans, S.; Thieulot-Rolin, N.; Sy, O.; Serbource-Goguel, J.; Vinsonneau, C.; et al. The Optic Nerve Sheath Diameter as a Useful Tool for Early Prediction of Outcome after Cardiac Arrest: A Prospective Pilot Study. Resuscitation 2016, 103, 7–13. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, S.H.; Oh, J.H.; Cho, I.S.; Lee, Y.H.; Han, C.; Choi, W.J.; Sohn, Y.D. Optic Nerve Sheath Diameter Measured Using Early Unenhanced Brain Computed Tomography Shows No Correlation with Neurological Outcomes in Patients Undergoing Targeted Temperature Management after Cardiac Arrest. Resuscitation 2018, 128, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Rush, B.; Wormsbecker, A.; Berger, L.; Wiskar, K.; Sekhon, M.S.; Griesdale, D.E. Optic Nerve Sheath Diameter on Computed Tomography Not Predictive of Neurological Status Post-Cardiac Arrest. Can. J. Emerg. Med. 2017, 19, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Goeres, P.; Zeiler, F.A.; Unger, B.; Karakitsos, D.; Gillman, L.M. Ultrasound Assessment of Optic Nerve Sheath Diameter in Healthy Volunteers. J. Crit. Care 2016, 31, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Jun, J.S.; Kim, R. Measurement of the Optic Nerve Sheath Diameter with Magnetic Resonance Imaging and Its Association with Eyeball Diameter in Healthy Adults. J. Clin. Neurol. 2018, 14, 345–350. [Google Scholar] [CrossRef]
- Zhu, S.; Cheng, C.; Zhao, D.; Zhao, Y.; Liu, X.; Zhang, J. The Clinical and Prognostic Values of Optic Nerve Sheath Diameter and Optic Nerve Sheath Diameter/Eyeball Transverse Diameter Ratio in Comatose Patients with Supratentorial Lesions. BMC Neurol. 2021, 21, 259. [Google Scholar] [CrossRef]
- Du, J.; Deng, Y.; Li, H.; Qiao, S.; Yu, M.; Xu, Q.; Wang, C. Ratio of Optic Nerve Sheath Diameter to Eyeball Transverse Diameter by Ultrasound Can Predict Intracranial Hypertension in Traumatic Brain Injury Patients: A Prospective Study. Neurocrit. Care 2020, 32, 478–485. [Google Scholar] [CrossRef]
- Park, J.S.; You, Y.; Min, J.H.; Yoo, I.; Jeong, W.; Cho, Y.; Ryu, S.; Lee, J.; Kim, S.W.; Cho, S.U.; et al. Study on the Timing of Severe Blood-Brain Barrier Disruption Using Cerebrospinal Fluid-Serum Albumin Quotient in Post Cardiac Arrest Patients Treated with Targeted Temperature Management. Resuscitation 2019, 135, 118–123. [Google Scholar] [CrossRef]
- You, Y.; Park, J.; Min, J.; Yoo, I.; Jeong, W.; Cho, Y.; Ryu, S.; Lee, J.; Kim, S.; Cho, S.; et al. Relationship between Time Related Serum Albumin Concentration, Optic Nerve Sheath Diameter, Cerebrospinal Fluid Pressure, and Neurological Prognosis in Cardiac Arrest Survivors. Resuscitation 2018, 131, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Geocadin, R.G.; Callaway, C.W.; Fink, E.L.; Golan, E.; Greer, D.M.; Ko, N.U.; Lang, E.; Licht, D.J.; Marino, B.S.; McNair, N.D.; et al. Standards for Studies of Neurological Prognostication in Comatose Survivors of Cardiac Arrest: A Scientific Statement from the American Heart Association. Circulation 2019, 140, E517–E542. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 100) | GNO (n = 28) | PNO (n = 72) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 66 (56–77) | 56 (52–65) | 74 (60–79) | <0.001 |
| Sex, male | 65 (65.0) | 22 (78.6) | 43 (59.7) | 0.076 |
| Comorbidities | ||||
| HTN | 49 (49.0) | 14 (50.0) | 35 (48.6) | 0.901 |
| DM | 30 (30.0) | 4 (14.3) | 26 (36.1) | 0.032 |
| MI | 12 (12.0) | 2 (7.1) | 10 (13.9) | 0.501 |
| Etiology | ||||
| Cardiac | 31 (31.0) | 22 (78.6) | 9 (12.5) | <0.001 |
| Respiratory | 31 (31.0) | 2 (7.1) | 29 (40.3) | 0.001 |
| Others | 38 (38.0) | 4 (14.3) | 34 (47.2) | 0.002 |
| Resuscitation | ||||
| Witnessed | 66 (66.0) | 19 (67.9) | 47 (65.3) | 0.807 |
| Bystander CPR | 62 (62.0) | 22 (78.6) | 40 (55.6) | 0.033 |
| Shockable rhythm | 22 (22.0) | 18 (64.3) | 4 (5.6) | <0.001 |
| Pre-hospital ROSC | 47 (47.0) | 23 (82.1) | 24 (33.3) | <0.001 |
| No-flow time, min | 10 (1–21) | 2 (0–9) | 12 (5–26) | <0.001 |
| Low-flow time, min | 12 (8–23) | 10 (6–16) | 14 (9–25) | 0.024 |
| ROSC to CT interval *, min | 97 (47–137) | 58 (31–87) | 113 (62–154) | <0.001 |
| TTM | 37 (37.0) | 11 (39.3) | 26 (36.1) | 0.812 |
| Total (n = 100) | GNO (n = 28) | PNO (n = 72) | p-Value | |
|---|---|---|---|---|
| Optic nerve sheath diameter, mm | ||||
| ONSD, Rt. | 5.74 (5.31–6.15) | 5.48 (5.19–5.96) | 5.79 (5.43–6.19) | 0.089 |
| ONSD, Lt. | 5.68 (5.22–5.90) | 5.48 (5.16–5.79) | 5.71 (5.24–6.06) | 0.078 |
| ONSD, average | 5.64 (5.34–6.02) | 5.48 (5.21–5.87) | 5.66 (5.43–6.05) | 0.054 |
| Eyeball transverse diameter, mm | ||||
| ETD, Rt. | 22.68 (21.92–23.32) | 23.08 (22.21–23.60) | 22.58 (21.83–23.28) | 0.162 |
| ETD, Lt. | 22.66 (22.01–23.29) | 22.80 (22.20–23.44) | 22.61 (21.96–23.11) | 0.286 |
| ETD, average | 22.65 (21.94–23.30) | 22.98 (22.13–23.52) | 22.61 (21.83–23.22) | 0.204 |
| ONSD/ETD ratio | ||||
| ONSD/ETD ratio, Rt. | 0.2531 (0.2354–0.2721) | 0.2407 (0.2263–0.2557) | 0.2578 (0.2404–0.2768) | 0.013 |
| ONSD/ETD ratio, Lt. | 0.2480 (0.2293–0.2671) | 0.2377 (0.2252–0.2503) | 0.2521 (0.2335–0.2723) | 0.021 |
| ONSD/ETD ratio, average | 0.2506 (0.2346–0.2676) | 0.2392 (0.2252–0.2532) | 0.2550 (0.2386–0.2721) | 0.014 |
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Unadjusted OR (95% CI) | p-Value | Adjusted OR (95% CI) | p-Value | |
| Age, year | 0.928 (0.892–0.965) | <0.001 | 0.916 (0.840–0.997) | 0.043 |
| Sex, male | 0.404 (0.146–1.119) | 0.081 | 0.289 (0.020–4.252) | 0.365 |
| DM | 0.295 (0.092–0.943) | 0.040 | 0.881 (0.065–11.994) | 0.924 |
| Etiology, cardiac | 25.667 (8.192–80.361) | <0.001 | 10.111 (0.423–241.721) | 0.153 |
| Etiology, respiratory | 0.114 (0.025–0.518) | 0.005 | 0.503 (0.021–12.129) | 0.672 |
| Bystander CPR | 2.933 (1.063–8.097) | 0.038 | 0.307 (0.020–4.662) | 0.395 |
| Shockable rhythm | 30.600 (8.588–109.027) | <0.001 | 5.351 (0.349–81.932) | 0.228 |
| Pre-hospital ROSC | 9.200 (3.111–27.204) | <0.001 | 1.569 (0.204–12.059) | 0.665 |
| No-flow time, min | 0.902 (0.850–0.958) | 0.001 | 0.924 (0.803–1.063) | 0.270 |
| Low-flow time, min | 0.950 (0.905–0.998) | 0.041 | 0.894 (0.814–0.982) | 0.019 |
| ROSC to CT interval *, min | 0.987 (0.977–0.996) | 0.006 | 0.988 (0.968–1.009) | 0.259 |
| ONSD/ETD ratio | 0.000 (0.000–0.009) | 0.014 | 0.000 (0.000–126,344,779.7) | 0.173 |
| Cut-Off | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|
| ONSD/ETD ratio for predicting PNO | >0.290 | 0.111 | 1.000 | 1.000 | 0.304 |
| ONSD/ETD ratio for predicting GNO | ≤0.257 | 0.857 | 0.458 | 0.381 | 0.892 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, B.-I.; Lee, H.; Shin, H.; Kim, C.; Choi, H.-J.; Kang, B.-S. The Prognostic Value of Optic Nerve Sheath Diameter/Eyeball Transverse Diameter Ratio in the Neurological Outcomes of Out-of-Hospital Cardiac Arrest Patients. Medicina 2022, 58, 1233. https://doi.org/10.3390/medicina58091233
Cho B-I, Lee H, Shin H, Kim C, Choi H-J, Kang B-S. The Prognostic Value of Optic Nerve Sheath Diameter/Eyeball Transverse Diameter Ratio in the Neurological Outcomes of Out-of-Hospital Cardiac Arrest Patients. Medicina. 2022; 58(9):1233. https://doi.org/10.3390/medicina58091233
Chicago/Turabian StyleCho, Byeong-In, Heekyung Lee, Hyungoo Shin, Changsun Kim, Hyuk-Joong Choi, and Bo-Seoung Kang. 2022. "The Prognostic Value of Optic Nerve Sheath Diameter/Eyeball Transverse Diameter Ratio in the Neurological Outcomes of Out-of-Hospital Cardiac Arrest Patients" Medicina 58, no. 9: 1233. https://doi.org/10.3390/medicina58091233