
Long-Term Results of Endovascular Treatment with Nitinol Stents for Femoropopliteal TASC II C and D Lesions

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
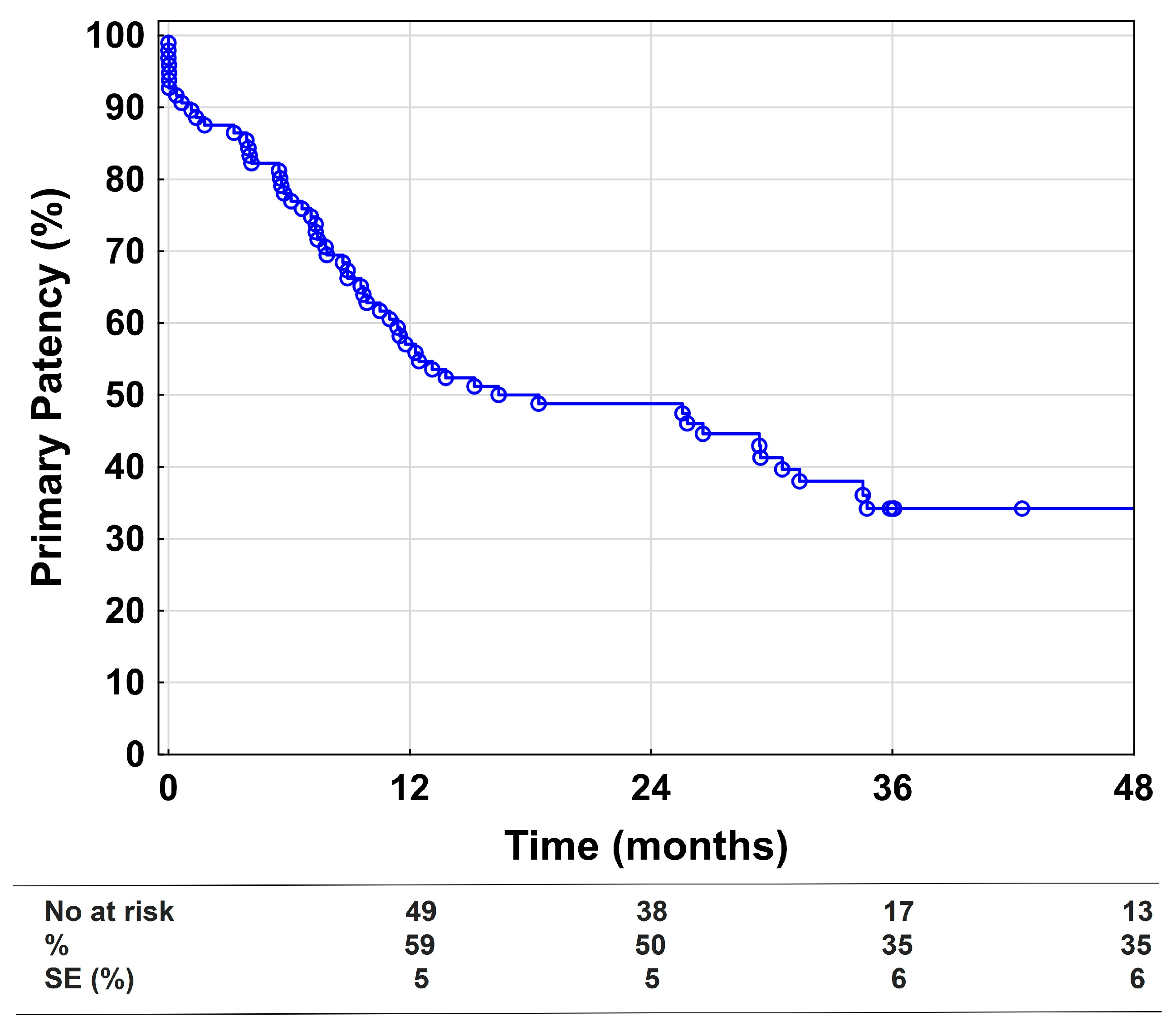
3.2. Primary Endpoint
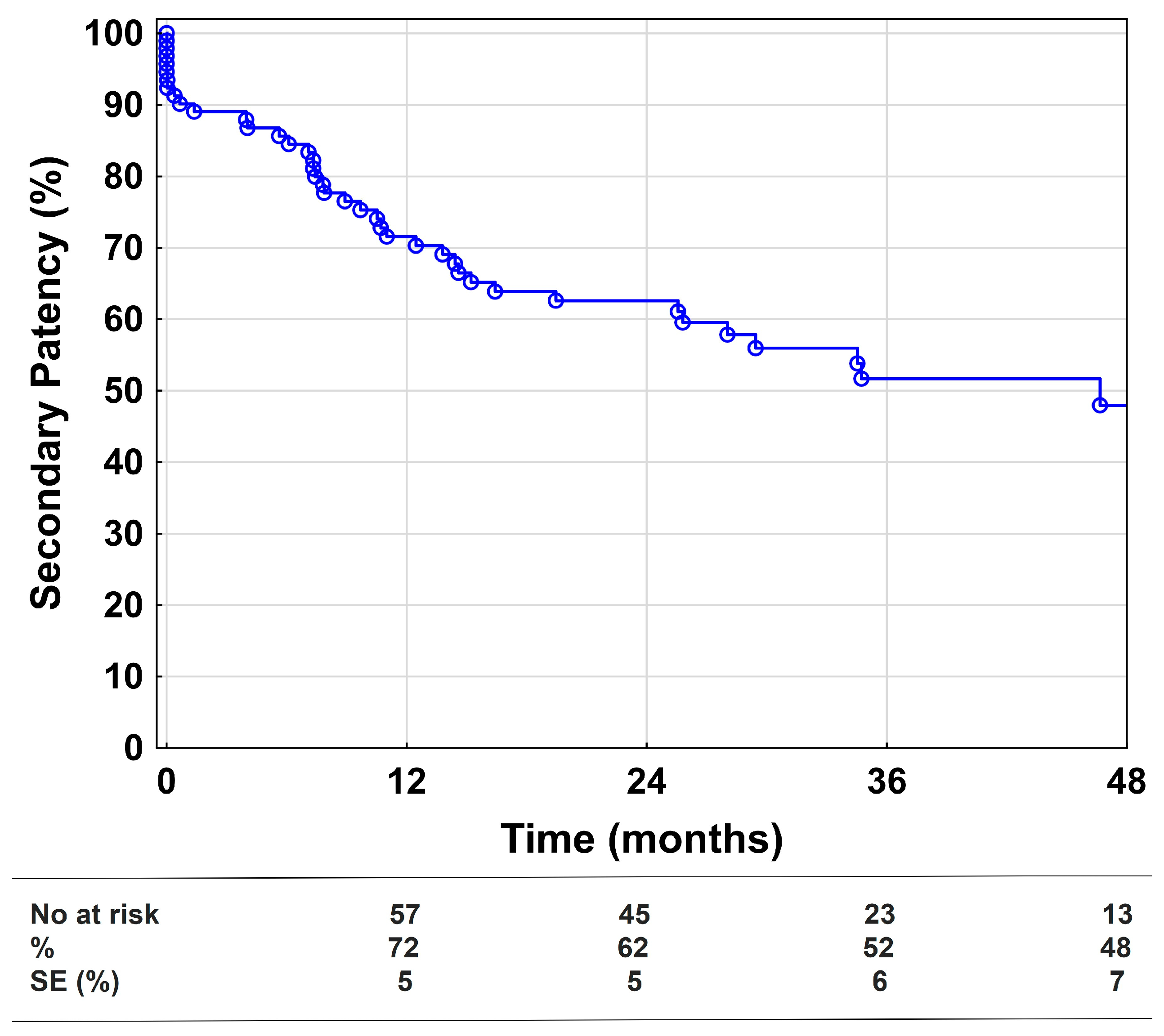
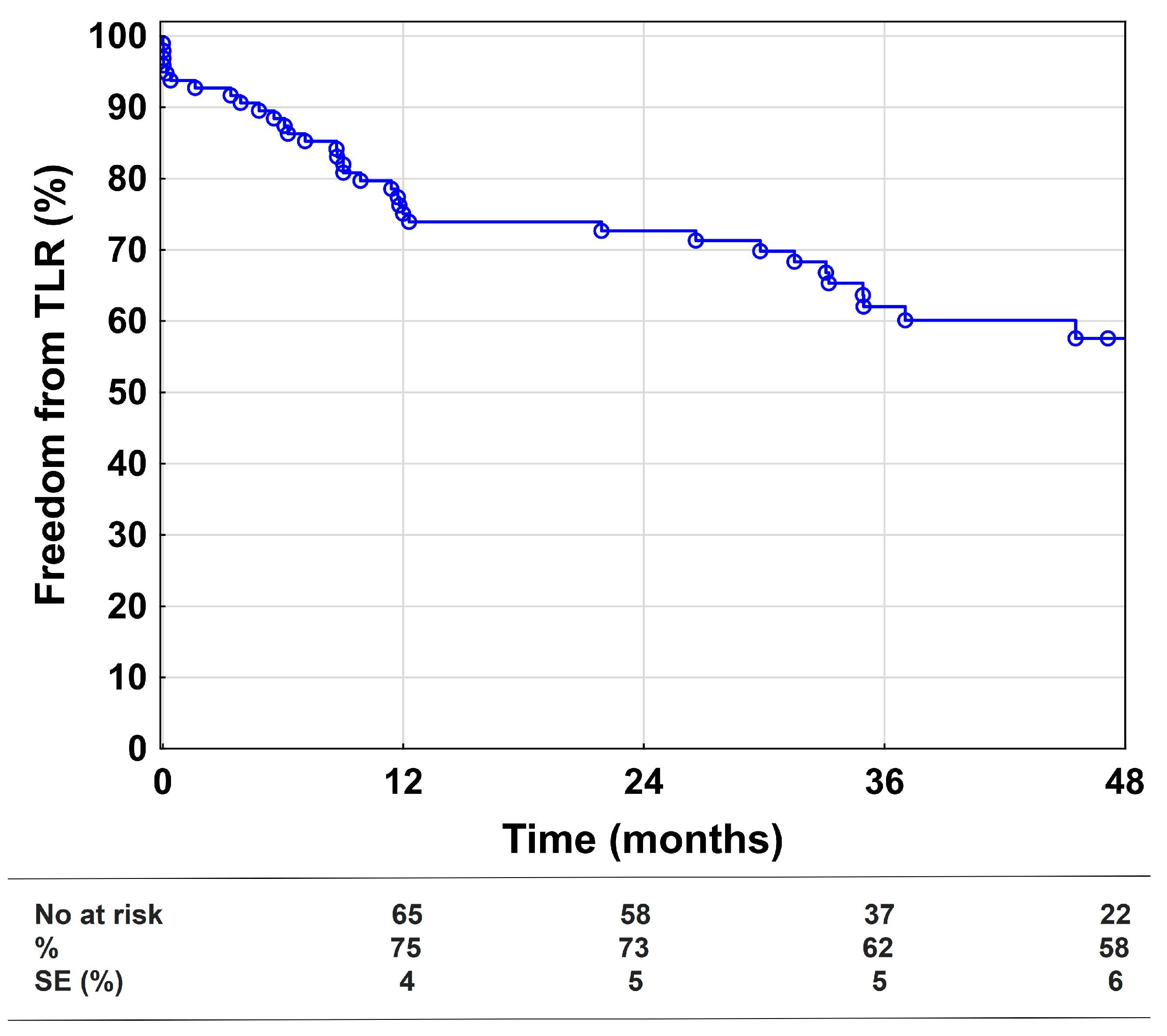
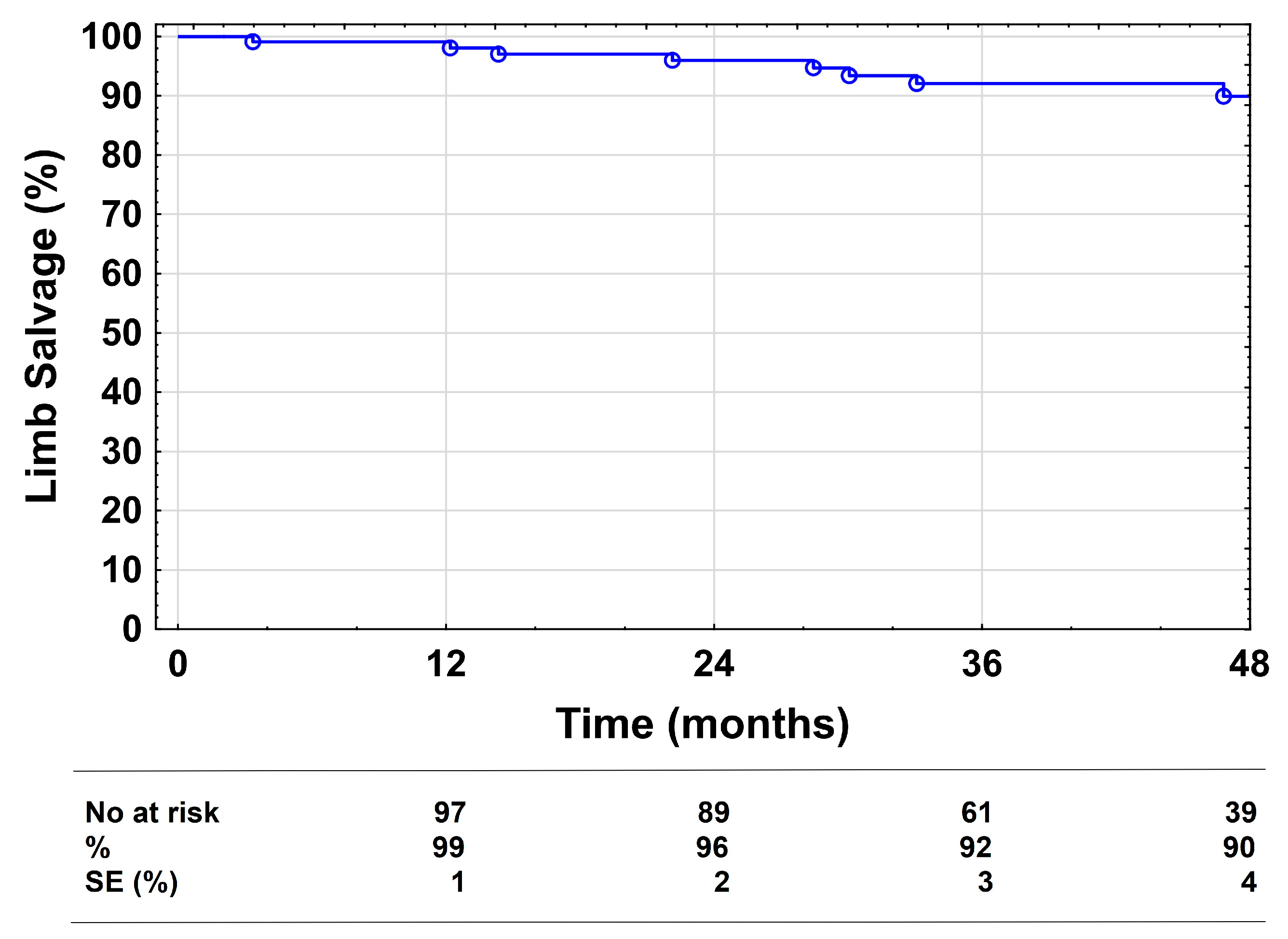
3.3. Secondary Endpoints
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef] [PubMed]
- Fowkes, F.G.; Murray, G.D.; Butcher, I.; Heald, C.L.; Lee, R.J.; Chambless, L.E.; Folsom, A.R.; Hirsch, A.T.; Dramaix, M.; de Backer, G.; et al. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: A meta-analysis. JAMA 2008, 300, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Jakubiak, G.K.; Pawlas, N.; Cieslar, G.; Stanek, A. Chronic Lower Extremity Ischemia and Its Association with the Frailty Syndrome in Patients with Diabetes. Int. J. Environ. Res. Public Health 2020, 17, 9339. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cieslar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 1970. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T. Current state of endovascular treatment of femoro-popliteal artery disease. Vasc. Med. 2007, 12, 223–234. [Google Scholar] [CrossRef]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.; Bell, K.; Caporusso, J.; Durand-Zaleski, I.; Komori, K.; et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J. Vasc. Endovasc. Surg. 2007, 33 (Suppl. S1), S1–S75. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. Editor’s Choice—2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 305–368. [Google Scholar] [CrossRef] [PubMed]
- Adam, D.J.; Beard, J.D.; Cleveland, T.; Bell, J.; Bradbury, A.W.; Forbes, J.F.; Fowkes, F.G.; Gillepsie, I.; Ruckley, C.V.; Raab, G.; et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): Multicentre, randomised controlled trial. Lancet 2005, 366, 1925–1934. [Google Scholar] [CrossRef]
- Laird, J.R.; Katzen, B.T.; Scheinert, D.; Lammer, J.; Carpenter, J.; Buchbinder, M.; Dave, R.; Ansel, G.; Lansky, A.; Cristea, E.; et al. Nitinol stent implantation vs. balloon angioplasty for lesions in the superficial femoral and proximal popliteal arteries of patients with claudication: Three-year follow-up from the RESILIENT randomized trial. J. Endovasc. Ther. 2012, 19, 1–9. [Google Scholar] [CrossRef]
- Rosenfield, K.; Jaff, M.R.; White, C.J.; Rocha-Singh, K.; Mena-Hurtado, C.; Metzger, D.C.; Brodmann, M.; Pilger, E.; Zeller, T.; Krishnan, P.; et al. Trial of a Paclitaxel-Coated Balloon for Femoropopliteal Artery Disease. N. Engl. J. Med. 2015, 373, 145–153. [Google Scholar] [CrossRef]
- Dake, M.D.; Ansel, G.M.; Jaff, M.R.; Ohki, T.; Saxon, R.R.; Smouse, H.B.; Machan, L.S.; Snyder, S.A.; O’Leary, E.E.; Ragheb, A.O.; et al. Durable Clinical Effectiveness With Paclitaxel-Eluting Stents in the Femoropopliteal Artery: 5-Year Results of the Zilver PTX Randomized Trial. Circulation 2016, 133, 1472–1483, discussion 1483. [Google Scholar] [CrossRef] [PubMed]
- Katsanos, K.; Spiliopoulos, S.; Kitrou, P.; Krokidis, M.; Karnabatidis, D. Risk of Death Following Application of Paclitaxel-Coated Balloons and Stents in the Femoropopliteal Artery of the Leg: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2018, 7, e011245. [Google Scholar] [CrossRef]
- Laird, J.R.; Zeller, T.; Loewe, C.; Chamberlin, J.; Begg, R.; Schneider, P.A.; Nanjundappa, A.; Bunch, F.; Schultz, S.; Harlin, S.; et al. Novel Nitinol Stent for Lesions up to 24 cm in the Superficial Femoral and Proximal Popliteal Arteries: 24-Month Results From the TIGRIS Randomized Trial. J. Endovasc. Ther. 2018, 25, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Nasr, B.; Gouailler, F.; Marret, O.; Guillou, M.; Chaillou, P.; Guyomarc’h, B.; Maurel, B.; Goueffic, Y. Treatment of Long Femoropopliteal Lesions With Self-Expanding Interwoven Nitinol Stent: 24 Month Outcomes of the STELLA-SUPERA Trial. J. Endovasc. Ther. 2022, 15266028221075227. [Google Scholar] [CrossRef]
- Vent, P.A.; Kaladji, A.; Davaine, J.M.; Guyomarch, B.; Chaillou, P.; Costargent, A.; Quillard, T.; Goueffic, Y. Bare Metal Versus Paclitaxel-Eluting Stents for Long Femoropopliteal Lesions: Prospective Cohorts Comparison Using a Propensity Score-Matched Analysis. Ann. Vasc. Surg. 2017, 43, 166–175. [Google Scholar] [CrossRef]
- Bohme, T.; Noory, E.; Brechtel, K.; Scheinert, D.; Bosiers, M.; Beschorner, U.; Zeller, T. Heparin-Bonded Stent-Graft for the Treatment of TASC II C and D Femoropopliteal Lesions: 36-Month Results of the Viabahn 25 cm Trial. J. Endovasc. Ther. 2021, 28, 222–228. [Google Scholar] [CrossRef]
- Enzmann, F.K.; Nierlich, P.; Holzenbein, T.; Aspalter, M.; Kluckner, M.; Hitzl, W.; Opperer, M.; Linni, K. Vein Bypass versus Nitinol Stent in Long Femoropopliteal Lesions: 4-Year Results of a Randomized Controlled Trial. Ann. Surg. 2022. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Baker, J.D.; Ernst, C.; Johnston, K.W.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended standards for reports dealing with lower extremity ischemia: Revised version. J. Vasc Surg 1997, 26, 517–538. [Google Scholar]
- Enzmann, F.K.; Nierlich, P.; Aspalter, M.; Hitzl, W.; Dabernig, W.; Holzenbein, T.; Ugurluoglu, A.; Seitelberger, R.; Linni, K. Nitinol Stent Versus Bypass in Long Femoropopliteal Lesions: 2-Year Results of a Randomized Controlled Trial. JACC Cardiovasc. Interv. 2019, 12, 2541–2549. [Google Scholar] [CrossRef]
- Jaff, M.R.; White, C.J.; Hiatt, W.R.; Fowkes, G.R.; Dormandy, J.; Razavi, M.; Reekers, J.; Norgren, L. An Update on Methods for Revascularization and Expansion of the TASC Lesion Classification to Include Below-the-Knee Arteries: A Supplement to the Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Endovasc. Ther. 2015, 22, 663–677. [Google Scholar] [CrossRef]
- Reijnen, M.; van Walraven, L.A.; Fritschy, W.M.; Lensvelt, M.M.A.; Zeebregts, C.J.; Lemson, M.S.; Wikkeling, O.R.M.; Smeets, L.; Holewijn, S. 1-Year Results of a Multicenter Randomized Controlled Trial Comparing Heparin-Bonded Endoluminal to Femoropopliteal Bypass. JACC Cardiovasc. Interv. 2017, 10, 2320–2331. [Google Scholar] [CrossRef] [PubMed]
- Bjorkman, P.; Auvinen, T.; Hakovirta, H.; Romsi, P.; Turtiainen, J.; Manninen, H.; Venermo, M. Drug-Eluting Stent Shows Similar Patency Results as Prosthetic Bypass in Patients with Femoropopliteal Occlusion in a Randomized Trial. Ann. Vasc. Surg. 2018, 53, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Bosiers, M.; Setacci, C.; De Donato, G.; Torsello, G.; Silveira, P.G.; Deloose, K.; Scheinert, D.; Veroux, P.; Hendriks, J.; Maene, L.; et al. ZILVERPASS Study: ZILVER PTX Stent vs Bypass Surgery in Femoropopliteal Lesions. J. Endovasc. Ther. 2020, 27, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Lammer, J.; Zeller, T.; Hausegger, K.A.; Schaefer, P.J.; Gschwendtner, M.; Mueller-Huelsbeck, S.; Rand, T.; Funovics, M.; Wolf, F.; Rastan, A.; et al. Sustained benefit at 2 years for covered stents versus bare-metal stents in long SFA lesions: The VIASTAR trial. Cardiovasc. Interv. Radiol. 2015, 38, 25–32. [Google Scholar] [CrossRef]
- Davaine, J.M.; Querat, J.; Kaladji, A.; Guyomarch, B.; Chaillou, P.; Costargent, A.; Quillard, T.; Goueffic, Y. Treatment of TASC C and D Femoropoliteal Lesions with Paclitaxel eluting Stents: 12 month Results of the STELLA-PTX Registry. Eur J. Vasc Endovasc. Surg. 2015, 50, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Torres-Blanco, A.; Edo-Fleta, G.; Gomez-Palones, F.; Molina-Nacher, V.; Ortiz-Monzon, E. Mid-Term Outcomes of Endovascular Treatment for TASC-II D Femoropopliteal Occlusive Disease with Critical Limb Ischemia. Cardiovasc. Interv. Radiol. 2016, 39, 344–352. [Google Scholar] [CrossRef]
- Micari, A.; Nerla, R.; Vadala, G.; Castriota, F.; Grattoni, C.; Liso, A.; Russo, P.; Pantaleo, P.; Roscitano, G.; Cremonesi, A. 2-Year Results of Paclitaxel-Coated Balloons for Long Femoropopliteal Artery Disease: Evidence From the SFA-Long Study. JACC Cardiovasc. Interv. 2017, 10, 728–734. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, X.; Zhang, J.; Zhuang, B.; Fu, W.; Wu, D.; Wang, F.; Zhao, Y.; Guo, P.; Bi, W.; et al. Drug-Coated Balloon Angioplasty Compared With Uncoated Balloons in the Treatment of 200 Chinese Patients With Severe Femoropopliteal Lesions: 24-Month Results of AcoArt I. JACC Cardiovasc. Interv. 2018, 11, 2347–2353. [Google Scholar] [CrossRef]
- Bisdas, T.; Beropoulis, E.; Argyriou, A.; Torsello, G.; Stavroulakis, K. 1-Year All-Comers Analysis of the Eluvia Drug-Eluting Stent for Long Femoropopliteal Lesions After Suboptimal Angioplasty. JACC Cardiovasc. Interv. 2018, 11, 957–966. [Google Scholar] [CrossRef]
- Roh, J.W.; Ko, Y.G.; Ahn, C.M.; Hong, S.J.; Shin, D.H.; Kim, J.S.; Kim, B.K.; Choi, D.; Hong, M.K.; Jang, Y. Risk Factors for Restenosis after Drug-coated Balloon Angioplasty for Complex Femoropopliteal Arterial Occlusive Disease. Ann. Vasc. Surg. 2019, 55, 45–54. [Google Scholar] [CrossRef]
- Davaine, J.M.; Querat, J.; Guyomarch, B.; Costargent, A.; Chaillou, P.; Patra, P.; Goueffic, Y. Primary stenting of TASC C and D femoropopliteal lesions: Results of the STELLA register at 30 months. Ann. Vasc. Surg. 2014, 28, 1686–1696. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. J. Vasc. Surg. 2019, 69, 3S–125S.e140. [Google Scholar] [CrossRef]
- Hossain, S.; Leblanc, D.; Farber, A.; Power, A.H.; DeRose, G.; Duncan, A.; Dubois, L. Editor’s Choice—Infrainguinal Bypass Following Failed Endovascular Intervention Compared With Primary Bypass: A Systematic Review and Meta-Analysis. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Nolan, B.W.; De Martino, R.R.; Stone, D.H.; Schanzer, A.; Goodney, P.P.; Walsh, D.W.; Cronenwett, J.L. Prior failed ipsilateral percutaneous endovascular intervention in patients with critical limb ischemia predicts poor outcome after lower extremity bypass. J. Vasc. Surg. 2011, 54, 730–735, discussion 735–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 103 | |
|---|---|
| Age (years) | 69.3 ± 7.0 |
| Male | 69 (67%) |
| Body mass index, kg/m2 | 26.5 ± 4.5 |
| Smoker | 36 (35%) |
| Hypertension | 89 (86%) |
| Dyslipidemia | 63 (61%) |
| Diabetes mellitus | 36 (35%) |
| Coronary artery disease | 48 (47%) |
| Previous stroke | 12 (12%) |
| Atrial fibrillation | 15 (15%) |
| Hemodialysis | 3 (3%) |
| ASA I | 1 (1%) |
| ASA II | 25 (24%) |
| ASA III | 77 (75%) |
| ABI | 0.51 ± 0.21 |
| Rutherford category | |
| 3 | 51 (47%) |
| 4 | 17 (15%) |
| 5 | 39 (36%) |
| 6 | 2 (2%) |
| N = 103, 109 Lesions | |
|---|---|
| Lesion length (mm) | 264 ± 58 |
| TASC II C | 48 (44%) |
| TASC II D | 61 (56%) |
| Chronic total occlusion | 87 (80%) |
| Recurrent lesion | 31 (28%) |
| Reference vessel diameter (mm) | 5.0 ± 0.7 |
| Severe calcification | 30 (28%) |
| Stenosis-free outflow vessels | |
| 1 | 26 (24%) |
| 2 | 53 (49%) |
| 3 | 30 (27%) |
| Procedural length (min) | 72 ± 30 |
| Contrast agent (ml) | 171 ± 80 |
| Number of stents | 4 ± 1.6 |
| Stent diameter (mm) | 6.5 ± 0.5 |
| Stented lesion length (mm) | 248 ± 98 |
| CFA angioplasty | 4 (4%) |
| Popliteal stenting | 30 (28%) |
| Re-entry device used | 11 (10%) |
| Trans-popliteal access | 24 (22%) |
| Loss of Primary Patency | Unadjusted HR (95% CI) | p-Value | Adjusted * HR (95% CI) | p-Value |
|---|---|---|---|---|
| TASC II D lesion | 0.61 (0.36–1.03) | 0.07 | ||
| Chronic total occlusion | 1.00 (0.53–1.89) | 0.99 | ||
| Lesion length > 25 cm | 0.91 (0.54–1.55) | 0.74 | ||
| Lesion length > 30 cm | 0.88 (0.43–1.80) | 0.73 | ||
| Previous intervention | 1.28 (0.71–2.28) | 0.41 | ||
| Reference vessel diameter < 5 mm | 0.85 (0.50–1.47) | 0.57 | ||
| Severe calcification | 0.95 (0.51–1.77) | 0.88 | ||
| Stenosis-free outflow vessels >1 | 1.17 (0.56–2.43) | 0.67 | ||
| Rutherford cat. 5 or 6 | 2.26 (1.19–4.28) | 0.01 | 2.46 (1.24–4.85) | 0.01 |
| No. of stents > 4 | 1.13 (0.67–1.90) | 0.66 | ||
| Stent diameter > 6 mm | 0.87 (0.51–1.50) | 0.62 | ||
| Stent oversizing > 1 mm | 1.02 (0.59–1.77) | 0.95 | ||
| Popliteal stenting | 1.05 (0.59–1.88) | 0.87 | ||
| Re-entry device used | 0.90 (0.39–2.10) | 0.80 | ||
| Trans-popliteal access | 0.89 (0.48–1.67) | 0.72 | ||
| Distal embolization | 3.83 (1.51–9.68) | 0.01 | 6.22 (2.31–16.79) | <0.001 |
| >1 local complication | 2.41 (0.86–6.75) | 0.09 |
| Target Lesion Revascularization | Unadjusted HR (95% CI) | p-Value | Adjusted * HR (95% CI) | p-Value |
|---|---|---|---|---|
| TASC II D lesion | 0.88 (0.44–1.71) | 0.68 | ||
| Chronic total occlusion | 1.86 (0.89–3.92) | 0.10 | ||
| Lesion length > 25 cm | 1.12 (0.57–2.21) | 0.73 | ||
| Lesion length > 30 cm | 1.69 (0.76–3.75) | 0.20 | ||
| Previous intervention | 1.78 (0.88–3.59) | 0.11 | ||
| Reference vessel diameter < 5 mm | 1.12 (0.56–2.24) | 0.75 | ||
| Severe calcification | 1.00 (0.45–2.20) | 0.99 | ||
| Stenosis-free outflow vessels > 1 | 1.02 (0.52–2.00) | 0.96 | ||
| Rutherford cat. 5 or 6 | 0.75 (0.35–1.62) | 0.47 | ||
| No. of stents > 4 | 1.87 (0.94–3.74) | 0.08 | ||
| Stent diameter > 6 mm | 0.67 (0.33–1.34) | 0.26 | ||
| Stent oversizing > 1 mm | 0.90 (0.45–1.80) | 0.77 | ||
| Popliteal stenting | 2.18 (1.09–4.35) | 0.03 | ||
| Re-entry device used | 1.08 (0.38–3.05) | 0.89 | ||
| Trans-popliteal access | 0.79 (0.36–1.77) | 0.57 | ||
| Distal embolization | 6.37 (2.43–16.70) | <0.001 | 6.50 (2.17–19.44) | 0.001 |
| >1 local complication | 2.88 (0.88–9.50) | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kluckner, M.; Nierlich, P.; Hitzl, W.; Aschacher, T.; Gratl, A.; Wipper, S.; Aspalter, M.; Moussalli, H.; Linni, K.; Enzmann, F.K. Long-Term Results of Endovascular Treatment with Nitinol Stents for Femoropopliteal TASC II C and D Lesions. Medicina 2022, 58, 1225. https://doi.org/10.3390/medicina58091225
Kluckner M, Nierlich P, Hitzl W, Aschacher T, Gratl A, Wipper S, Aspalter M, Moussalli H, Linni K, Enzmann FK. Long-Term Results of Endovascular Treatment with Nitinol Stents for Femoropopliteal TASC II C and D Lesions. Medicina. 2022; 58(9):1225. https://doi.org/10.3390/medicina58091225
Chicago/Turabian StyleKluckner, Michaela, Patrick Nierlich, Wolfgang Hitzl, Thomas Aschacher, Alexandra Gratl, Sabine Wipper, Manuela Aspalter, Herve Moussalli, Klaus Linni, and Florian K. Enzmann. 2022. "Long-Term Results of Endovascular Treatment with Nitinol Stents for Femoropopliteal TASC II C and D Lesions" Medicina 58, no. 9: 1225. https://doi.org/10.3390/medicina58091225