
Assessment of Sexual Dysfunction in Cervical Cancer Patients after Different Treatment Modality: A Systematic Review
 ,
,  , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
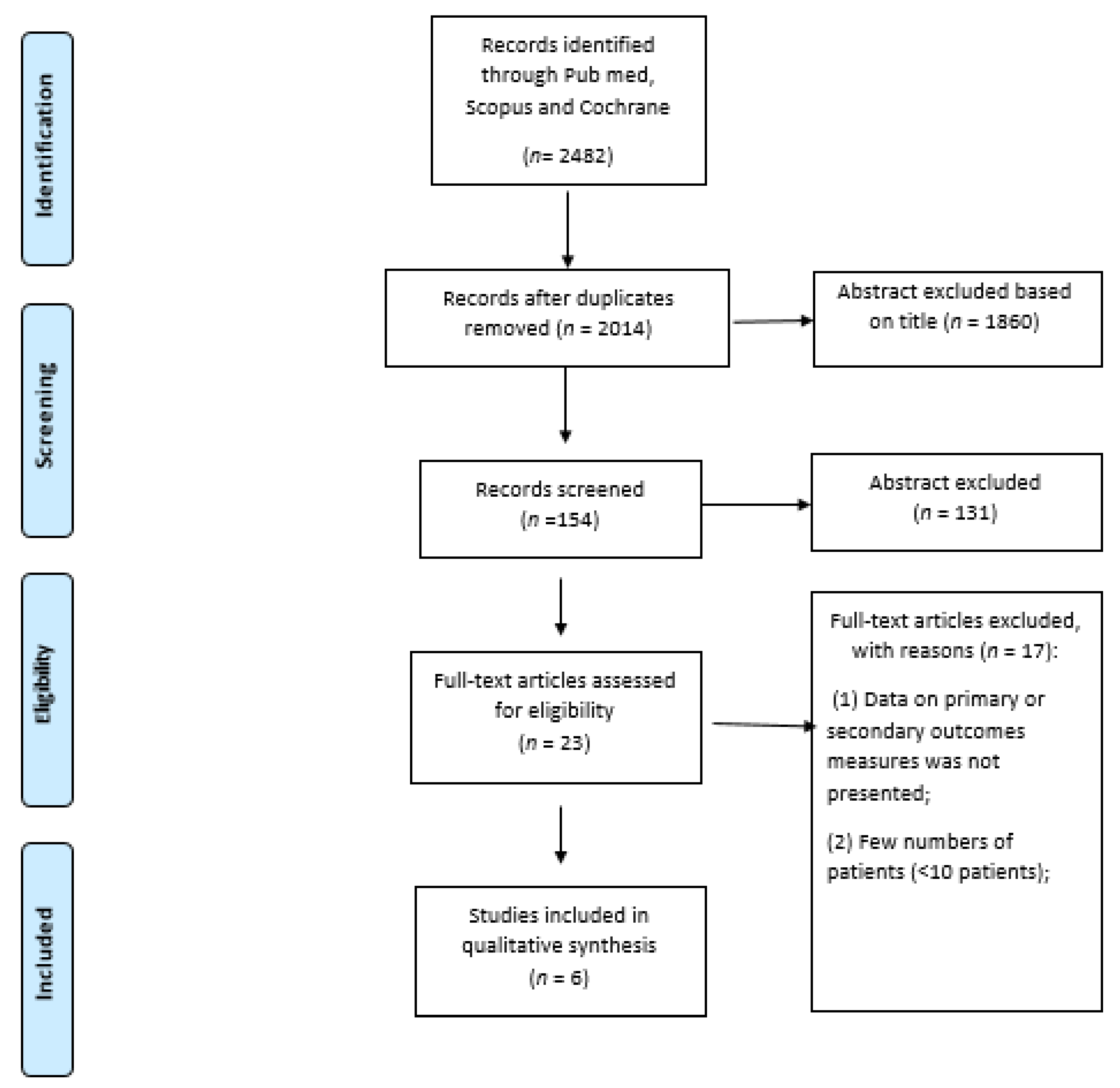
2. Materials and Methods
Search Strategy and Selection of Evidence
3. Results
3.1. Studies Characteristics
3.2. Studies Description
3.3. Outcomes
3.4. Evidence to Decision Framework
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, Second Edition: Use of mRNA Tests for Human Papillomavirus (HPV). 2021. Available online: https://www.who.int/publications/i/item/9789240040434 (accessed on 5 May 2022).
- NCCN: National Comprensive Cancer Network Cervical Cancer Versione 1. 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 5 May 2022).
- Sturdza, A.; Potter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Šegedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.; Mahantshetty, U.; Engineer, R.; Chopra, S.; Hawaldar, R.; Hande, V.; Kerkar, R.A.; Maheshwari, A.; Shylasree, T.S.; Ghosh, J.; et al. Cisplatin chemoradiotherapy vs radiotherapy in FIGO stage IIIB squamous cell carcinoma of the uterine cervix: A randomized clinical trial. JAMA Oncol. 2018, 4, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Maheshwari, A.; Parab, P.; Mahantshetty, U.; Hawaldar, R.; Sastri, S.; Kerkar, R.; Engineer, R.; Tongaonkar, H.; Ghosh, J.; et al. Neoadjuvant chemotherapy followed by radical surgery versus concomitant chemotherapy and radiotherapy in patients with stage IB2, IIA, or IIB squamous cervical cancer: A randomized controlled trial. J. Clin. Oncol. 2018, 36, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.L.; Gerber, R.; Han, K.; Jiang, H.; Xie, J.; Beiki-Ardakani, A.; Fyles, A.; Milosevic, M.; Williamson, D.; Croke, J. Patient-reported sexual adjustament after definitive chemoradiation and MR-guided brachytherapy for cervical cancer. Brachyterapy 2019, 18, 133–140. [Google Scholar] [CrossRef]
- Kirchheiner, K.; Smet, S.; Jürgenliemk-Schulz, I.M.; Haie-Meder, C.; Chargari, C.; Lindegaard, J.C.; Fokdal, L.U.; Spampinato, S.; Schmid, M.P.; Sturdza, A.; et al. Impact of vaginal symptoms and hormonal replacement therapy on sexual outcomes in locally advanced cervical cancer patients after definitive chemoradiotherapy—Results from the EMBRACE-I study. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 400–413. [Google Scholar] [CrossRef]
- Jensen, P.T.; Groenvold, M.; Klee, M.C.; Thranov, I.; Petersen, M.A.; Machin, D. Longitudinal study of sexual function and vaginal changes after radiotherapy for cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 937–949. [Google Scholar] [CrossRef]
- Hofsjö, A.; Bohm-Starke, N.; Blomgren, B.; Jahren, H.; Steineck, G.; Bergmark, K. Radiotherapy-induced vaginal fibrosis in cervical cancer survivors. Acta Oncol. 2017, 56, 661–666. [Google Scholar] [CrossRef]
- Ye, S.; Yang, J.; Cao, D.; Lang, J.; Shen, K. A systematic review of quality of life and sexual function of patients with cervical cancer after treatment. Int. J. Gynecol. Cancer 2014, 24, 1146–1157. [Google Scholar] [CrossRef]
- Bae, H.; Park, H. Sexual function, depression, and quality of life in patients with cervical cancer. Supportive Care Cancer 2016, 24, 1277–1283. [Google Scholar] [CrossRef]
- Correia, R.A.; Bomfim, C.V.; Feitosa, K.M.A.; Furtado, B.M.A.S.M.; Ferreira, D.K.S.; Santos, S.L. Sexual dysfunction after cervical cancer treatment. Rev. Esc. Enferm. USP 2020, 54, 03636. [Google Scholar] [CrossRef]
- Fakunle, I.E.; Maree, J.E. Sexual function in South African women treated for cervical cancer. Int. J. Afr. Nurs. Sci. 2019, 10, 124–130. [Google Scholar] [CrossRef]
- Frumovitz, M.; Sun, C.C.; Schover, L.R.; Munsell, M.F.; Jhingran, A.; Wharton, J.T.; Eifel, P.; Bevers, T.B.; Levenback, C.F.; Gershenson, D.M.; et al. Quality of Life and Sexual Functioning in Cervical Cancer Survivors. J. Clin. Oncol. 2005, 23, 7428–7436. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Yang, X.; Dai, Y.; Wu, Q.; He, G.; Yin, G. Survey of cervical cancer survivors regarding quality of life and sexual function. J. Cancer Res. Ther. 2016, 12, 938–944. [Google Scholar] [CrossRef]
- Abbott-Anderson, K.; Kwekkeboom, K.L. A systematic review of sexual concerns reported by gynecological cancer survivors. Gynecol. Oncol. 2012, 124, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Bergmark, K.; Avall-Lundqvist, E.; Dickman, P.W.; Henningsohn, L.; Steineck, G. Vaginal changes and sexuality in women with a history of cervical cancer. N. Engl. J. Med. 1999, 340, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, E.; Ussher, J.M.; Perz, J. Sexuality after gynaecological cancer: A review of the material, intrapsychic, and discursive aspects of treatment on women’s sexual-wellbeing. Maturitas 2011, 70, 42–57. [Google Scholar] [CrossRef]
- Jensen, P.T.; Groenvold, M.; Klee, M.C.; Thranov, I.; Petersen, M.A.; Machin, D. Early-stage cervical carcinoma, radical hysterectomy, and sexual function. A longitudinal study. Cancer 2004, 100, 97–106. [Google Scholar] [CrossRef]
- Lammerink, E.A.; de Bock, G.H.; Pras, E.; Reyners, A.K.; Mourits, M.J. Sexual functioning of cervical cancer survivors: A review with a female perspective. Maturitas 2012, 72, 296–304. [Google Scholar] [CrossRef]
- Lindau, S.T.; Gavrilova, N.; Anderson, D. Sexual morbidity in very long-term survivors of vaginal and cervical cancer: A comparison to national norms. Gynecol. Oncol. 2007, 106, 413–418. [Google Scholar] [CrossRef]
- Pieterse, Q.D.; Maas, C.P.; Ter Kuile, M.M.; Lowik, M.; Van Eijkeren, M.A.; Trimbos, J.B.M.Z.; Kenter, G.G. An observational longitudinal study to evaluate miction, defecation, and sexual function after radical hysterectomy with pelvic lymphadenectomy for early-stage cervical cancer. Int. J. Gynecol. Cancer 2006, 16, 1119–1129. [Google Scholar] [CrossRef]
- Grover, S.; Hill-Kayser, C.E.; Vachani, C.; Hampshire, M.K.; DiLullo, G.A.; Metz, J.M. Patient reported late effects of gynecological cancer treatment. Gynecol. Oncol. 2012, 124, 399–403. [Google Scholar] [CrossRef]
- White, I.D.; Sangha, A.; Lucas, G.; Wiseman, T. Assessment of sexual difficulties associated with multi-modal treatment for cervical or endometrial cancer: A systematic review of measurement instruments. Gynecol. Oncol. 2016, 143, 664–673. [Google Scholar] [CrossRef]
- Nout, R.A.; Putter, H.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Mens, J.W.M.; Slot, A.; Stenfert Kroese, M.C.; van Bunningen, B.N.; et al. Quality of life after pelvic radiotherapy or vaginal brachytherapy for endometrial cancer: First results of the randomized PORTEC-2 trial. J. Clin. Oncol. 2009, 27, 3547–3556. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.; Chong, T.; Hollands, E.; Tan, J.; Mohan, G.R.K.A.; Cohen, P.A. Screening for sexual health concerns in survivors of gynecological cancer. Supportive Care Cancer 2020, 28, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Cull, A.; Cowıe, V.J.; Farquharson, D.I.M.; Lıvıngstone, J.R.B.; Smart, G.E.; Elton, R.A. Early stage cervical cancer: Psychosocial and sexual outcomes of treatment. Br. J. Cancer 1993, 68, 1216–1220. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M. Preventing or reducing late side effects of radiation therapy: Radiobiology meets molecular pathology. Nat. Rev. Cancer 2006, 6, 702–713. [Google Scholar] [CrossRef]
- Grigsby, P.W.; Russell, A.; Bruner, D.; Eifel, P.; Koh, W.J.; Spanos, W.; Stetz, J.; Stitt, J.A.; Sullivan, J. Late injury of cancer therapy on the female reproductive tract. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1281–1299. [Google Scholar] [CrossRef]
- Pitkin, R.M.; Bradbury, J.T. The effect of topical estogen on irradiated vaginal epithelium. Am. J. Obstet. Gynecol. 1965, 92, 175–182. [Google Scholar] [CrossRef]
- Eltabbakh, G.H.; Piver, M.; Hempling, R.E.; Shin, K.H. Excellent long-term survival and absence of vaginal recurrences in 332 patients with low-risk stage I endometrial adenocarcinoma treated with hysterectomy and vaginal brachytherapy without formal staging lymph node sampling: Report of a prospective trial. Int. J. Radiat. Oncol. 1997, 38, 373–380. [Google Scholar] [CrossRef]
- Abitbol, M.M.; Davenport, J.H. The irradiated vagina. Obstet. Gynecol. 1974, 44, 249–256. [Google Scholar]
- Chan, J.L.; Letourneau, J.; Salem, W.; Cil, A.P.; Chan, S.W.; Chen, L.M.; Rosen, M.P. Sexual satisfaction and quality of life in survivors of localized cervical and ovarian cancers following fertility-sparing surgery. Gynecol. Oncol. 2015, 139, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Xiao, M.; Gao, H.; Bai, H.; Zhang, Z. Quality of life and sexuality in disease-free survivors of cervical cancer after radical hysterectomy alone: A comparison between total laparoscopy and laparotomy. Medicine 2016, 95, e4787. [Google Scholar] [CrossRef] [PubMed]
- Fleming, N.D.; Ramirez, P.T.; Soliman, P.T.; Schmeler, K.M.; Chisholm, G.B.; Nick, A.M.; Westin, S.N.; Frumovitz, M. Quality of life after radical trachelectomy for early-stage cervical cancer: A 5-year prospective evaluation. Gynecol. Oncol. 2016, 143, 596–603. [Google Scholar] [CrossRef]
- Plotti, F.; Terranova, C.; Capriglione, S.; Crispino, S.; Pomi, A.L.; de Cicco Nardone, C.; Montera, R.; Panici, P.B.; Angioli, R.; Scaletta, G. Assessment of quality of life and urinary and sexual function after radical hysterectomy in long-term cervical cancer survivors. Int. J. Gynecol. Cancer 2018, 28, 818–823. [Google Scholar] [CrossRef]
- Zhou, J.; Rao, L.; Yu, G.; Cook, T.R.; Chen, X.; Huang, F. Supramolecular cancer nanotheranostics. Chem. Soc. Rev. 2021, 50, 2839–2891. [Google Scholar] [CrossRef]
- Zhou, J.; Yu, G.; Huang, F. Supramolecular chemotherapy based on host-guest molecular recognition: A novel strategy in the battle against cancer with a bright future. Chem. Soc. Rev. 2017, 46, 7021–7053. [Google Scholar] [CrossRef]
- Nkiwane, K.S.; Pötter, R.; Tanderup, K.; Federico, M.; Lindegaard, J.C.; Kirisits, C. Single line source with and without vaginal loading and the impact on target coverage and organ at risk doses for cervix cancer Stages IB, II, and IIIB: Treatment planning simulation in patients treated with MRIguided adaptive brachytherapy in a multicentre study (EMBRACE). Brachytherapy 2013, 12, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Lindegaard, J.C.; Fokdal, L.U.; Nielsen, S.K.; Christensen, J.J.; Tanderup, K. MRI-guided adaptive radiotherapy in locally advanced cervical cancer from a Nordic perspective. Acta Oncol. 2013, 52, 1510–1519. [Google Scholar] [CrossRef]
- Amsterdam, A.; Krychman, M. Sexual dysfunction in patients with gynecologic neoplasms: A retrospective pilot study. J. Sex. Med. 2006, 3, 646–649. [Google Scholar] [CrossRef]
- Bourgeois-Law, G.; Lotocki, R. Sexuality and gynecological cancer: A needs assessment. Can. J. Hum. Sex. 1999, 8, 231–240. [Google Scholar]
- Bukovic, D.; Silovski, H.; Silovski, T.; Hojsak, I.; Sakic, K.; Hrgovic, Z. Sexual functioning and body image of patients treated for ovarian cancer. Sex. Disabil. 2008, 26, 63–73. [Google Scholar] [CrossRef]
- Juraskova, I.; Butow, P.; Robertson, R.; Sharpe, L.; McLeod, C.; Hacker, N. Post-treatment sexual adjustment following cervical and endometrial cancer: A qualitative insight. Psychooncology 2003, 12, 267–279. [Google Scholar] [CrossRef]
- Lancellotta, V.; De Sanctis, V.; Cornacchione, P.; Barbera, F.; Fusco, V.; Vidali, C.; Scalise, S.; Panza, G.; Tenore, A.; Colloca, G.; et al. HAPPY—Humanity Assurance Protocol in interventional radiotheraPY (brachytherapy)—An AIRO Interventional Radiotherapy Study Group project. J. Contemp. Brachytherapy 2019, 11, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Ferrandina, G.; Mantegna, G.; Petrillo, M.; Fuoco, G.; Venditti, L.; Terzano, S.; Moruzzi, C.; Lorusso, D.; Marcellusi, A.; Scambia, G. Quality of life and emotional distress in early stage and locally advanced cervical cancer patients: A prospective, longitudinal study. Gynecol. Oncol. 2012, 124, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Van Gijn, W.; Van Stiphout, R.G.P.M.; Van De Velde, C.J.H.; Valentini, V.; Lammering, G.; Gambacorta, M.A.; Påhlman, L.; Bujko, K.; Lambin, P. Nomograms to predict survival and the risk for developing local or distant recurrence in patients with rectal cancer treated with optional short-term radiotherapy. Ann. Oncol. 2015, 26, 928–935. [Google Scholar] [CrossRef]
- Gambacorta, M.A.; Valentini, C.; Dinapoli, N.; Boldrini, L.; Caria, N.; Barba, M.C.; Mattiucci, G.C.; Pasini, D.; Minsky, B.; Valentini, V. Clinical validation of atlas-based auto-segmentation of pelvic volumes and normal tissue in rectal tumors using auto-segmentation computed system. Acta Oncol. 2013, 52, 1676–1681. [Google Scholar] [CrossRef]
- Ferrandina, G.; Gambacorta, A.; Gallotta, V.; Smaniotto, D.; Fagotti, A.; Tagliaferri, L.; Foti, E.; Fanfani, F.; Autorino, R.; Scambia, G.; et al. Chemoradiation with concomitant boosts followed by radical surgery in locally advanced cervical cancer: Long-term results of the ROMA-2 prospective phase 2 study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 778–785. [Google Scholar] [CrossRef]
- Rai, B.; Dhanireddy, B.; Patel, F.D.; Kumari, R.; Oinam, A.S.; Simha, V.; Sharma, S. Vaginal dose, toxicity and sexual outcomes in patients of cervical cancer undergoing image based brachytherapy. Asian Pac. J. Cancer Prev. 2014, 15, 3619–3623. [Google Scholar] [CrossRef]
- Perrone, A.M.; Tesei, M.; Ferioli, M.; De Terlizzi, F.; Della Gatta, A.N.; Boussedra, S.; Dondi, G.; Galuppi, A.; Morganti, A.G.; De Iaco, P. Results of a phase i-ii study on laser therapy for vaginal side effects after radiotherapy for cancer of uterine cervix or endometrium. Cancers 2020, 12, 1639. [Google Scholar] [CrossRef]
- Flynn, P.; Kew, F.; Kisely, S.R. Interventions for psychosexual dysfunction in women treated for gynaecological malignancy. Cochrane Database Syst. Rev. 2009, 2009, CD004708. [Google Scholar] [CrossRef]
- Balducci, M.; Fiorentino, A.; De Bonis, P.; Chiesa, S.; Manfrida, S.; D’Agostino, G.R.; Mantini, G.; Frascino, V.; Mattiucci, G.C.; De Bari, B.; et al. Impact of age and co-morbidities in patients with newly diagnosed glioblastoma: A pooled data analysis of three prospective mono-institutional phase II studies. Med. Oncol. 2012, 29, 3478–3483. [Google Scholar] [CrossRef] [PubMed]
- Coco, C.; Valentini, V.; Manno, A.; Rizzo, G.; Gambacorta, M.A.; Mattana, C.; Verbo, A.; Picciocchi, A. Functional results after radiochemotherapy and total mesorectal excision for rectal cancer. Int. J. Colorectal Dis. 2007, 22, 903–910. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Period | Study | Tumor | Sample Size, n | Median Age, Years | Stage | Type of Treatment | FSFI | QoL | Main Results | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bae [11] | Retrospective | Cervix | 137 | 50 (28–59) | I: 114 II: 2 III: 1 IV: 2 | Surgery: 85 Surgery + RT: 12 Surgery + RT-CT: 22 Surgery + CT: 5 RT-CT: 13 | 4.83 ± 4.16 Sexual desire: 1.53 ± 0.67 Satisfaction: 1.32 ± 0.64 Sexual arousal: 0.52 ± 0.88 Pain: 0.49 ± 0.86 Orgasm: 0.50 ± 0.82 Lubrication: 0.46 ± 0.75 | FACT-G 57.33 ± 8.47 Physical well-being: 16.91 ± 3.21 Functional well-being: 4.47 ± 4.51 Emotional well-being: 14.00 ± 2.41 Social well-being: 11.95 ± 2.25 | Cervical cancer patients with high sexual function tended to have low levels of depression and exhibited a higher quality of life | |||
| Frumovitz [14] | 1991–98 | Retrospective | Cervix | RT: 37 S: 37 | RT: 46.9 S: 43.6 | RT Ia1: 0 Ia2: 0 Ib1: 22 Ib2: 15 | S Ia1: 1 Ia2:3 Ib1: 33 Ib2: 0 | RT: 37 S: 37 | RT: 17.1 Sexual desire: 2.9 Satisfaction: 3.2 Sexual arousal: 2.6 Pain: 2.7 Orgasm: 2.8 Lubrication: 2.9 | S: 25.1 Sexual desire: 3.4 Satisfaction: 4.4 Sexual arousal: 4 Pain: 4.6 Orgasm: 4.2 Lubrication: 4.5 | MCS RT: 47 S: 50.5 NS | Radiation patients had significantly poorer scores on health-related quality of life, psychosocial distress and sexual functioning. The disparity in sexual function remained significant in a multivariate analysis. |
| Conway [6] | 2008–10 | Retrospective | Cervix | 27 | 50 (30–64) | IB: 15 IIA-IIB: 11 IIIA-B: 1 | CRT + IRT: 27 | Baseline: 16.4 1.5 months: 22.3 3 months: 23 6 months: 21.8 9 months: 23.9 12 months: 22.1 | Patients with higher FIGO stages (≥IIB) had significantly worse sexual adjustment (p = 0.005) | |||
| Correira [12] | 2015–16 | Retrospective | Cervix | 46 | 28 (30–49) | Surgery: 9 Surgery + RT: 9 RT-CT: 28 (IRT: 24) | Sexual desire: 3.20 Satisfaction: 4.23 Sexual arousal: 3.38 Pain: 4.10 Orgasm: 3.10 Lubrication: 3.65 | The types of treatment (p = 0.03) and of RT (p = 0.01), and the stage (p = 0.02) interfered with the sexual function. The most affected domains of the FSFI were lubrication (p = 0.03) and pain (p = 0.04) | ||||
| Fakunle [13] | Retrospective | Cervix | 147 | 44 (30–73) | EBRT + IRT: 89 RT-CT + IRT: 58 | Sexual desire: 2.5 Satisfaction: 3.1 Sexual arousal: 2.2 Pain: 2.4 Orgasm: 2.5 Lubrication: 2.4 | Not find a statistically significant relationship between type of treatmentReceived, counseling, age and sexual function | |||||
| Zhou [15] | 2007–10 | Retrospective | Cervix | 140 | 45.6 (27–68) | I-III | Surgery: 120 CT: 80 RT: 108 | Sexual desire: 2.58 Satisfaction: 2.80 Sexual arousal: 1.81 Pain: 2.47 Orgasm: 2.13 Lubrication: 2.09 | FACT-G 124.45 Physical well-being: 22.2 ± 4.96 Functional well-being: 18.43 ± 5.65 Emotional well-being: 18.35 ± 4.75 Social well-being: 21.96 ± 4.60 | Sexual function was affected by radiotherapy, age, type of surgery, sleep disorders, and occupation | ||
| Authors | Total FSFI | Desire | Arousal | Orgasm | Lubrification | Pain | Satisfaction | Main Results |
|---|---|---|---|---|---|---|---|---|
| Bae [11] | 57.33 ± 8.47 | 1.53 ± 0.67 | 0.52 ± 0.88 | 0.50 ± 0.82 | 0.46 ± 0.75 | 0.49 ± 0.86 | 1.32 ± 1.64 | Patients aged 20–39 years old (p < 0.001), married (p = 0.031), high education (p = 0.022), work (p > 0.001), spouse (p = 0.016) and CT treatment (p = 0.030) had significantly worse sexual activity |
| Conway [6] | Time 0: 48.5 12 m: 49.7 | Time 0: 8.4 12 m: 8.9 | Time 0: 2.8 12 m: 3.7 | Time 0: 6.3 12 m: 6.4 | Time 0: 7.8 12 m: 8.5 | Time 0: 10 12 m: 7.3 | Time 0: 6.4 12 m: 6.3 | Patients with higher FIGO stages (>IIB) had significantly worse sexual adjustment (p = 0.005) |
| Correira [12] | 21.66 | 3.20 | 3.38 | 3.10 | 3.65 | 4.10 | 4.23 | The treatment interfered with sexual activity (p < 0.001). The type of treatment (p = 0.03), the type of RT (p = 0.01) and the stage of the disease (p = 0.02) were associated with whether or not the woman was sexually active after the treatment. Lubrication (p = 0.03) and pain (p = 0.04) were influenced by the type of treatment. |
| Fakunle [13] | At 3 m: 13.9 At 12 m: 15.7 | At 3 m: 2.4 At 12 m: 2.5 | At 3 m: 2.1 At 12 m: 2.2 | At 3 m: 2.3 At 12 m: 2.5 | At 3 m: 2.2 At 12 m: 2.4 | At 3 m: 2.0 At 12 m: 2.8 | At 3 m: 2.9 At 12 m: 3.2 | In terms of the full FSFI score, only 5.4% (n = 8) of the women experienced good sexual function. Age, treatment received, and counseling did not impact sexual function |
| Frumovitz [14] | RT: 17.1 S + RT: 25.1 | RT: 2.9 S + RT: 3.4 | RT: 2.6 S + RT: 4.0 | RT: 2.8 S + RT: 4.2 | RT: 2.9 S + RT: 4.5 | RT: 2.7 S + RT: 4.6 | RT: 3.2 S + RT: 4.4 | Irradiated patients showed significantly worse sexual functioning |
| Zhou [15] | 13.9 | 2.58 | 1.81 | 2.13 | 2.09 | 2.47 | 2.80 | Factors that were significantly associated with the total FSFI score were age, RT, sleep disorders, radical hysterectomy, and white-collar occupation (p < 0.05) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tramacere, F.; Lancellotta, V.; Casà, C.; Fionda, B.; Cornacchione, P.; Mazzarella, C.; De Vincenzo, R.P.; Macchia, G.; Ferioli, M.; Rovirosa, A.; et al. Assessment of Sexual Dysfunction in Cervical Cancer Patients after Different Treatment Modality: A Systematic Review. Medicina 2022, 58, 1223. https://doi.org/10.3390/medicina58091223
Tramacere F, Lancellotta V, Casà C, Fionda B, Cornacchione P, Mazzarella C, De Vincenzo RP, Macchia G, Ferioli M, Rovirosa A, et al. Assessment of Sexual Dysfunction in Cervical Cancer Patients after Different Treatment Modality: A Systematic Review. Medicina. 2022; 58(9):1223. https://doi.org/10.3390/medicina58091223
Chicago/Turabian StyleTramacere, Francesco, Valentina Lancellotta, Calogero Casà, Bruno Fionda, Patrizia Cornacchione, Ciro Mazzarella, Rosa Pasqualina De Vincenzo, Gabriella Macchia, Martina Ferioli, Angeles Rovirosa, and et al. 2022. "Assessment of Sexual Dysfunction in Cervical Cancer Patients after Different Treatment Modality: A Systematic Review" Medicina 58, no. 9: 1223. https://doi.org/10.3390/medicina58091223