
Minimally Invasive Spinal Treatment (MIST)—A New Concept in the Treatment of Spinal Diseases: A Narrative Review

 , ,
, ,  , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Results and Discussion
3.1. History and Development of Minimally Invasive Decompression
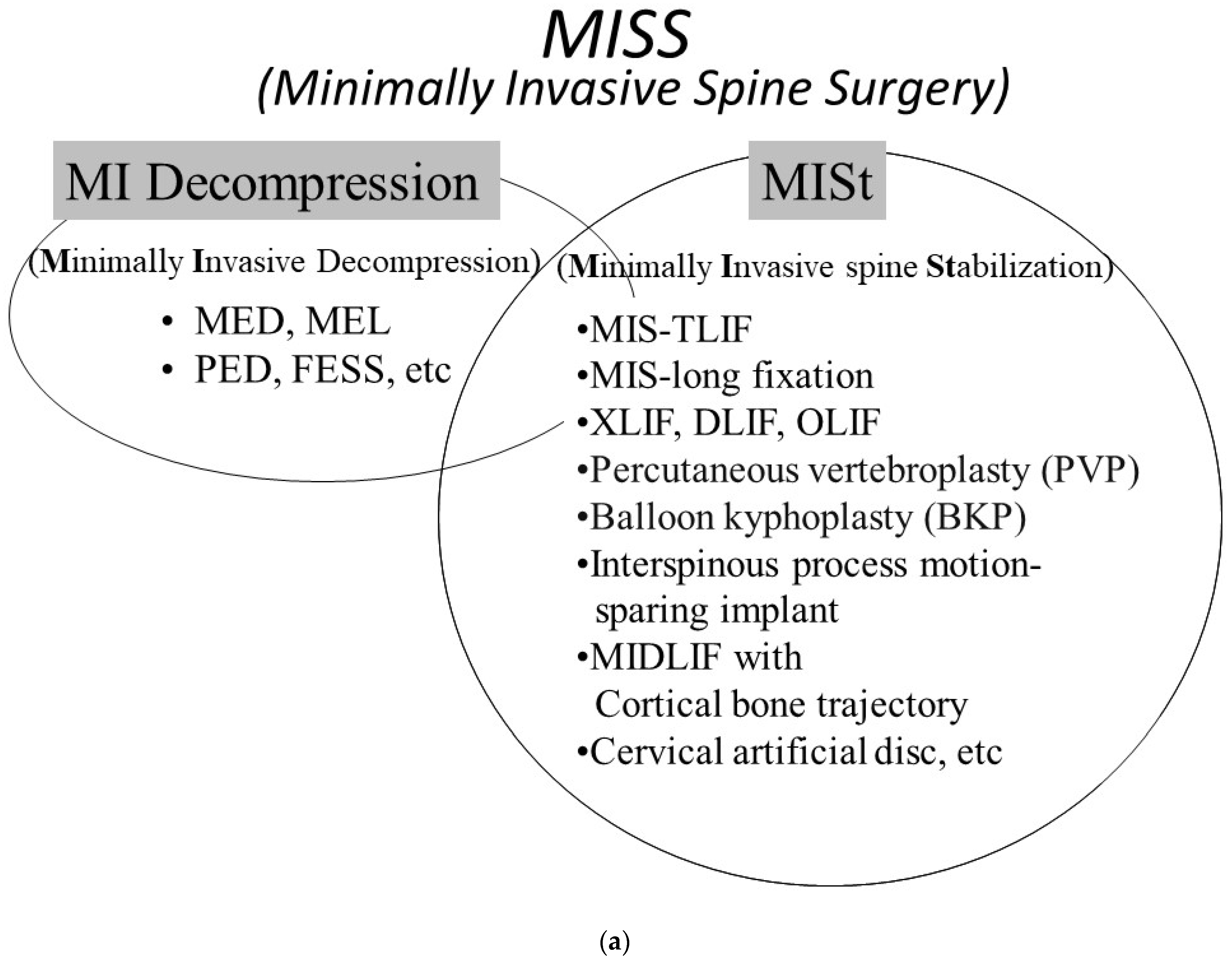
3.2. Concept of the Minimally Invasive Spine Stabilization (MISt) Procedure
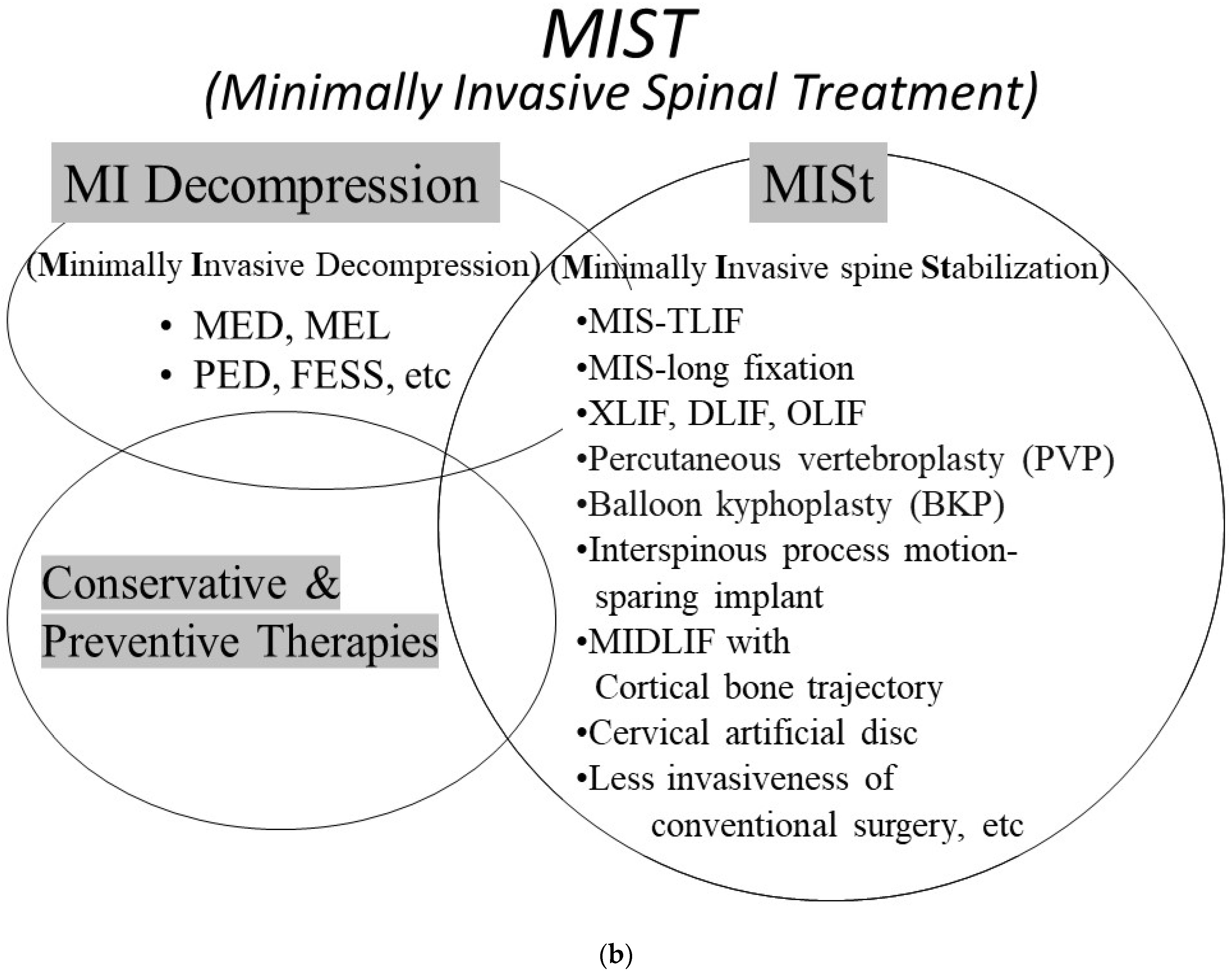
3.3. Concept of Minimally Invasive Spinal Treatment (MIST)
3.4. Technical Advances in Minimally Invasive Spinal Treatment (MIST): Navigation, Augmented Reality, and Beyond
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Keller, T.; Holland, M.C. Some notable American spine surgeons of the 19th century. Spine 1997, 22, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Mixter, W.J.; Barr, J.S. Rupture of the intervertebral disc with involvement of the spinal canal. N. Engl. J. Med. 1934, 211, 210–215. [Google Scholar] [CrossRef]
- Yaşargil, M.G.; Krayenbühl, H. The use of the binocular microscope in neurosurgery. Bibl. Ophthalmol. 1970, 81, 62–65. [Google Scholar] [PubMed]
- Hijikata, S. Percutaneous nucleotomy. A new concept technique and 12 years’ experience. Clin. Orthop. Relat. Res. 1989, 238, 9–23. [Google Scholar] [CrossRef]
- Kambin, P.; O’Brien, E.; Zhou, L.; Schaffer, J.L. Arthroscopic microdiscectomy and selective fragmentectomy. Clin. Orthop. Relat. Res. 1998, 247, 150–167. [Google Scholar] [CrossRef]
- Yeung, A.T.; Tsou, P.M. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine 2002, 27, 722–731. [Google Scholar] [CrossRef]
- Foley, K.T.; Smith, M.M. Microendoscopic discectomy. Technol. Neurosurg. 1997, 3, 301–307. [Google Scholar]
- Schick, U.; Döhnert, J.; Richter, A.; König, A.; Vitzthum, H.E. Microendoscopic lumbar discectomy versus open surgery: An intraoperative EMG study. Eur. Spine J. 2002, 11, 20–26. [Google Scholar] [CrossRef]
- Shin, D.A.; Kim, K.N.; Shin, H.C.; Yoon, D.H. The efficacy of microendoscopic discectomy in reducing iatrogenic muscle injury. J. Neurosurg. Spine 2008, 8, 39–43. [Google Scholar] [CrossRef]
- Harrington, J.F.; French, P. Open versus minimally invasive lumbar microdiscectomy: Comparison of operative times, length of hospital stay, narcotic use and complications. Minim. Invasive Neurosurg. 2008, 51, 30–35. [Google Scholar] [CrossRef]
- Foley, K.T.; Smith, M.M.; Rampersaud, Y.R. Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurg. Focus 1999, 7, e5. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Watanabe, K.; Ishii, K.; Tsuji, T.; Takaishi, H.; Nakamura, M.; Toyama, Y.; Chiba, K. Posterior decompression surgery for extraforaminal entrapment of the fifth lumbar spinal nerve at the lumbosacral junction. J. Neurosurg. Spine 2010, 12, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Adamson, T.E. Microendoscopic posterior cervical laminoforaminotomy for unilateral radiculopathy: Results of a new technique in 100 cases. J. Neurosurg. 2001, 95, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Matsumoto, M.; Watanabe, K.; Nakamura, M.; Chiba, K.; Toyama, Y. Endoscopic resection of cystic lesions in the lumbar spinal canal: A report of two cases. Minim. Invasive Neurosurg. 2005, 48, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Smith, N.; Masters, J.; Jensen, C.; Khan, A.; Sprowson, A. Systematic review of microendoscopic discectomy for lumbar disc herniation. Eur. Spine J. 2013, 22, 2458–2465. [Google Scholar] [CrossRef]
- Ishii, K.; Arizono, T.; Hachiya, Y.; Hoshino, M.; Kotani, Y.; Nakanishi, K.; Saito, T.; Sato, K.; Shinohara, A.; Tanaka, M.; et al. Minimally invasive spine stabilization. Bone Jt. Nerve 2014, 4, 541–545. [Google Scholar]
- Foley, K.; Holly, L.; Schwender, J. Minimally invasive lumbar fusion. Spine 2003, 28, S26–S35. [Google Scholar] [CrossRef]
- Khoo, L.T.; Palmer, S.; Laich, D.T.; Fessler, R.G. Minimally invasive percutaneous posterior lumbar interbody fusion. Neurosurgery 2002, 51, S166–S181. [Google Scholar] [CrossRef]
- Ishii, K. Up-to-date techniques: Minimally invasive posterior fusion. Orthotimes 2011, 5, 1. [Google Scholar]
- Hikata, T.; Isogai, N.; Shiono, Y.; Funao, H.; Okada, E.; Fujita, N.; Iwanami, A.; Watanabe, K.; Tsuji, T.; Nakamura, M.; et al. A Retrospective Cohort Study Comparing the Safety and Efficacy of Minimally Invasive Versus Open Surgical Techniques in the Treatment of Spinal Metastases. Clin. Spine Surg. 2017, 30, E1082–E1087. [Google Scholar] [CrossRef]
- Eck, J.C. Minimally invasive corpectomy and posterior stabilization for lumbar burst fracture. Spine J. 2011, 11, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Shiono, Y.; Funao, H.; Singh, K.; Matsumoto, M. A Novel Groove-Entry Technique for Inserting Thoracic Percutaneous Pedicle Screws. Clin. Spine Surg. 2017, 30, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme Lateral Interbody Fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef]
- Pimenta, L. Lateral endoscopic transpsoas retroperitoneal approach for lumbar spine surgery. In Proceedings of the VIII Brazilian Spine Society Meeting, Belo Horizonte, Brazil, May 2001. [Google Scholar]
- Mayer, H.M. A new microsurgical technique for minimally invasive anterior lumbar interbody fusion. Spine 1997, 22, 691–699, discussion 700. [Google Scholar] [CrossRef]
- Santoni, B.G.; Hynes, R.A.; McGilvray, K.C.; Rodriguez-Canessa, G.; Lyons, A.S.; Henson, M.A.; Womack, W.J.; Puttlitz, C.M. Cortical bone trajectory for lumbar pedicle screws. Spine J. 2009, 9, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Anand, N.; Baron, E.M.; Thaiyananthan, G.; Khalsa, K.; Goldstein, T.B. Minimally invasive multilevel percutaneous correction and fusion for adult lumbar degenerative scoliosis: A technique and feasibility study. J. Spinal Disord. Tech. 2008, 21, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Tomycz, L.; Parker, S.L.; McGirt, M.J. Minimally invasive transpsoas L2 corpectomy and percutaneous pedicle screw fixation for osteoporotic burst fracture in the elderly: A technical report. J. Spinal Disord. Tech. 2015, 28, 53–60. [Google Scholar] [CrossRef]
- Deininger, M.H.; Unfried, M.I.; Vougioukas, V.I.; Hubbe, U. Minimally invasive dorsal percutaneous spondylodesis for the treatment of adult pyogenic spondylodiscitis. Acta Neurochir. 2009, 151, 1451–1457. [Google Scholar] [CrossRef]
- Holly, L.T.; Foley, K.T. Intraoperative spinal navigation. Spine 2003, 28, S54–S61. [Google Scholar] [CrossRef]
- Larson, A.N.; Santos, E.R.; Polly, D.W., Jr.; Ledonio, C.G.; Sembrano, J.N.; Mielke, C.H.; Guidera, K.J. Pediatric pedicle screw placement using intraoperative computed tomography and 3-dimensional image-guided navigation. Spine 2012, 37, E188–E194. [Google Scholar] [CrossRef]
- Ray, W.Z.; Ravindra, V.M.; Schmidt, M.H.; Dailey, A.T. Stereotactic navigation with the O-arm for placement of S-2 alar iliac screws in pelvic lumbar fixation. J. Neurosurg. Spine 2013, 18, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Drazin, D.; Liu, J.C.; Acosta, F.L., Jr. CT navigated lateral interbody fusion. J. Clin. Neurosci. 2013, 20, 1438–1441. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Sugimoto, M.; Imura, S.; Morine, Y.; Ikemoto, T.; Iwahashi, S.; Yamada, S.; Shimada, M. Intraoperative 3D Hologram Support with Mixed Reality Techniques in Liver Surgery. Ann. Surg. 2020, 271, e4–e7. [Google Scholar] [CrossRef]
- Yamada, Y.; Nakamura, T.; Yamada, M.; Maruyama, J.; Maruyama, K.; Azuma, E. Use of Augmented Reality to Assist Teaching for Future Perfusionists in Extracorporeal Technology. J. Extra Corpor. Technol. 2019, 51, 244–247. [Google Scholar] [PubMed]
- Peh, S.; Chatterjea, A.; Pfarr, J.; Schäfer, J.P.; Weuster, M.; Klüter, T.; Seekamp, A.; Lippross, S. Accuracy of augmented reality surgical navigation for minimally invasive pedicle screw insertion in the thoracic and lumbar spine with a new tracking device. Spine J. 2020, 20, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Burström, G.; Nachabé, R.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Edström, E.; Gerdhem, P. Augmented reality navigation with intraoperative 3D imaging vs fluoroscopy-assisted free-hand surgery for spine fixation surgery: A matched-control study comparing accuracy. Sci. Rep. 2020, 10, 707. [Google Scholar] [CrossRef]
- Nachabe, R.; Strauss, K.; Schueler, B.; Bydon, M. Radiation dose and image quality comparison during spine surgery with two different, intraoperative 3D imaging navigation systems. J. Appl. Clin. Med. Phys. 2019, 20, 136–145. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishii, K.; Watanabe, G.; Tomita, T.; Nikaido, T.; Hikata, T.; Shinohara, A.; Nakano, M.; Saito, T.; Nakanishi, K.; Morimoto, T.; et al. Minimally Invasive Spinal Treatment (MIST)—A New Concept in the Treatment of Spinal Diseases: A Narrative Review. Medicina 2022, 58, 1123. https://doi.org/10.3390/medicina58081123
Ishii K, Watanabe G, Tomita T, Nikaido T, Hikata T, Shinohara A, Nakano M, Saito T, Nakanishi K, Morimoto T, et al. Minimally Invasive Spinal Treatment (MIST)—A New Concept in the Treatment of Spinal Diseases: A Narrative Review. Medicina. 2022; 58(8):1123. https://doi.org/10.3390/medicina58081123
Chicago/Turabian StyleIshii, Ken, Goichi Watanabe, Takashi Tomita, Takuya Nikaido, Tomohiro Hikata, Akira Shinohara, Masato Nakano, Takanori Saito, Kazuo Nakanishi, Tadatsugu Morimoto, and et al. 2022. "Minimally Invasive Spinal Treatment (MIST)—A New Concept in the Treatment of Spinal Diseases: A Narrative Review" Medicina 58, no. 8: 1123. https://doi.org/10.3390/medicina58081123