
Feasibility, Usability, and Customer Satisfaction of the Tele-COVID19 Project, Sicilian Model

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
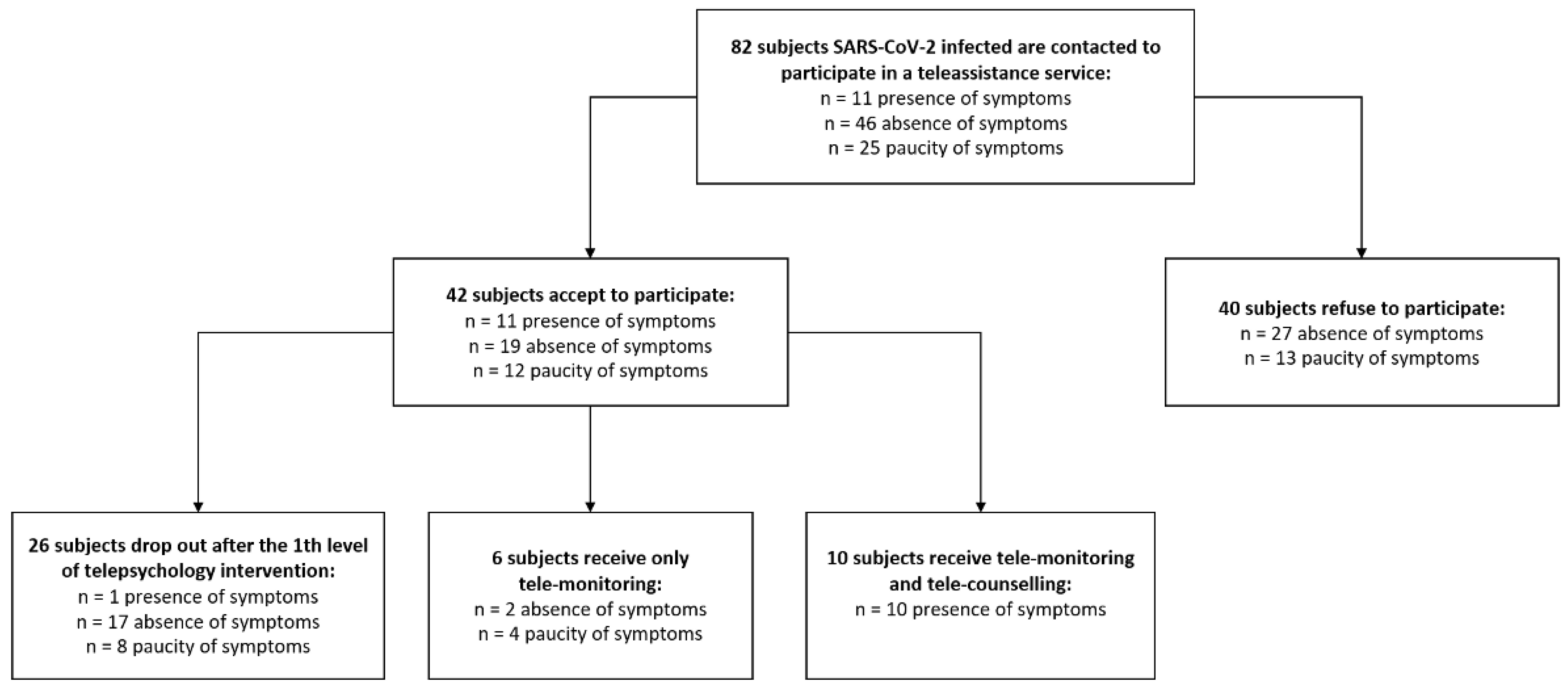
2.1. Study Design and Setting
2.2. Study Population
2.3. Assessment
2.4. Statistical Analysis
3. Procedure
3.1. The Telemedicine Service
3.2. The Telemedicine Platform
4. Results
4.1. Telemedicine Service Feasibility
4.2. Patient Satisfaction and Usability
4.3. Quality of the Service
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ferran, M.; De La Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic Impacts of Confinement during the COVID-19 Pandemic Due to Modified Diet and Physical Activity Habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef] [PubMed]
- Ali, I.; Alharbi, O.M. COVID-19: Disease, management, treatment, and social impact. Sci. Total Environ. 2020, 728, 138861. [Google Scholar] [CrossRef]
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef]
- While, A.; Dewsbury, G. Nursing and information and communication technology (ICT): A discussion of trends and future directions. Int. J. Nurs. Stud. 2011, 48, 1302–1310. [Google Scholar] [CrossRef]
- Kruse, C.S.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating barriers to adopting telemedicine worldwide: A systematic review. J. Telemed. Telecare 2018, 24, 4–12. [Google Scholar] [CrossRef]
- Bello-Chavolla, O.Y.; Bahena-Lopez, J.P.; Antonio-Villa, N.E.; Vargas-Vázquez, A.; González-Díaz, A.; Márquez-Salinas, A.; Fermín-Martínez, C.A.; Naveja, J.J.; Aguilar-Salinas, C.A. Predicting mortality due to SARS-CoV-2: A mechanistic score relating obesity and diabetes to COVID-19 outcomes in Mexico. J. Clin. Endocrinol. Metab. 2020, 105, 2752–2761. [Google Scholar] [CrossRef]
- Mehrotra, A.; Ray, K.; Brockmeyer, D.M.; Barnett, M.L.; Bender, J.A. Rapidly converting to “virtual practices”: Outpatient care in the era of COVID-19. NEJM Catal. Innov. Care Deliv. 2020, 1. [Google Scholar] [CrossRef]
- Reforma, L.G.; Duffy, C.; Ai-ris, Y.C.; Wylie, B.J.; Shainker, S.A.; Golen, T.H.; Herlihy, M.; Lydeard, A.; Zera, C.A. Multidisciplinary telemedicine model for management of coronavirus disease 2019 (COVID-19) in obstetrical patients. Am. J. Obstet. Gynecol. MFM 2020, 2, 100180. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Battiato, S.; Agodi, A. Modeling the novel coronavirus (SARS-CoV-2) outbreak in Sicily, Italy. Int. J. Environ. Res. Public Health 2020, 17, 4964. [Google Scholar] [CrossRef]
- Mantovani, E.; Zucchella, C.; Bottiroli, S.; Federico, A.; Giugno, R.; Sandrini, G.; Chiamulera, C.; Tamburin, S. Telemedicine and Virtual Reality for Cognitive Rehabilitation: A Roadmap for the COVID-19 Pandemic. Front. Neurol. 2020, 11, 926. [Google Scholar] [CrossRef]
- Cassarino, L.; Santoro, F.; Gelardi, D.; Panerai, S.; Papotto, M.; Tripodi, M.; Cosentino, F.I.I.; Neri, V.; Ferri, R.; Ferlito, S.; et al. Post-stroke aphasia at the time of COVID-19 pandemic: A telerehabilitation perspective. J. Integr. Neurosci. 2022, 21, 8. [Google Scholar] [CrossRef]
- Brooke, J. SUS—A quick and dirty usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, A.L., Eds.; Taylor and Francis: London, UK, 1986. [Google Scholar]
- De Cola, M.C.; Maresca, G.; D’Aleo, G.; Carnazza, L.; Giliberto, S.; Maggio, M.G.; Bramanti, A.; Calabrò, R.S. Teleassistance for frail elderly people: A usability and customer satisfaction study. Geriatr. Nurs. 2020, 41, 463–467. [Google Scholar] [CrossRef]
- Han, Y.; Lie, R.K.; Guo, R. The Internet Hospital as a Telehealth Model in China: Systematic Search and Content Analysis. J. Med. Internet Res. 2020, 22, e17995. [Google Scholar] [CrossRef]
- Dhippayom, T.; Rattanachaisit, N.; Jhunsom, S.; Dilokthornsakul, P.; Chaiyakunapruk, N.; Devine, B. Comparative effects of telemedicine and face-to-face warfarin management: A systematic review and network meta-analysis. J. Am. Pharm. Assoc. 2020, 22, 204–214. [Google Scholar] [CrossRef]
- Sorinmade, O.A.; Kossoff, L.; Peisah, C. COVID-19 and Telehealth in Older Adult Psychiatry-opportunities for now and the Future. Int. J. Geriatr. Psychiatry 2020, 35, 1427–1430. [Google Scholar] [CrossRef]
- Battisti, N.M.L.; Mislang, A.R.; Cooper, L.; O’Donovan, A.; Audisio, R.A.; Cheung, K.-L.; Sarrió, R.G.; Stauder, R.; Soto-Perez-De-Celis, E.; Jaklitsch, M.; et al. Adapting care for older cancer patients during the COVID-19 pandemic: Recommendations from the International Society of Geriatric Oncology (SIOG) COVID-19 Working Group. J. Geriatr. Oncol. 2020, 11, 1190–1198. [Google Scholar] [CrossRef]
- Deora, H.; Mishra, S.; Tripathi, M.; Garg, K.; Tandon, V.; Borkar, S.; Varshney, N.; Raut, R.; Chaurasia, B.; Chandra, P.S.; et al. Adapting Neurosurgery Practice During the COVID-19 Pandemic in the Indian Subcontinent. World Neurosurg. 2020, 142, e396–e406. [Google Scholar] [CrossRef]
- Moccia, M.; Lanzillo, R.; Morra, V.B.; Bonavita, S.; Tedeschi, G.; Leocani, L.; Lavorgna, L. Assessing disability and relapses in multiple sclerosis on tele-neurology. Neurol. Sci. 2020, 41, 1369–1371. [Google Scholar] [CrossRef]
- Amparore, D.; Claps, F.; Cacciamani, G.E.; Esperto, F.; Fiori, C.; Liguori, G.; Serni, S.; Trombetta, C.; Carini, M.; Porpiglia, F.; et al. Impact of the COVID-19 pandemic on urology residency training in Italy. Minerva Urol. Nefrol. 2020, 72, 505–509. [Google Scholar] [CrossRef]
- Torrisi, M.; Maresca, G.; De Cola, M.C.; Cannavò, A.; Sciarrone, F.; Silvestri, G.; Bramanti, A.; De Luca, R.; Calabrò, R.S. Using telerehabilitation to improve cognitive function in post-stroke survivors: Is this the time for the continuity of care? Int. J. Rehabil. Res. 2019, 42, 344–351. [Google Scholar] [CrossRef]
- Maresca, G.; De Cola, M.C.; Caliri, S.; De Luca, R.; Manuli, A.; Scarcella, I.; Silvestri, G.; Bramanti, P.; Torrisi, M.; Calabrò, R.S.; et al. Moving towards novel multidisciplinary approaches for improving elderly quality of life: The emerging role of telemedicine in Sicily. J. Telemed. Telecare 2019, 25, 318–324. [Google Scholar] [CrossRef]
- Jothimani, D.; Daniel, H.; Danielraj, S.; Ramachandran, H.; Rela, M. COVID-19 Lockdown: Impact on Liver Transplant Recipients—A Single Centre Survey. J. Assoc. Physicians India 2020, 68, 96. [Google Scholar]
- Tiwaskar, M.; Vora, A. COVID 19 in India: What we have Accomplished so Far. J. Assoc. Physicians India 2020, 68, 11–12. [Google Scholar]
- Wang, Y.; Duan, Z.; Ma, Z.; Mao, Y.; Li, X.; Wilson, A.; Qin, H.; Ou, J.; Peng, K.; Zhou, F.; et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl. Psychiatry 2020, 10, 263. [Google Scholar] [CrossRef]
- Cameron, E.E.; Joyce, K.M.; Delaquis, C.P.; Reynolds, K.; Protudjer, J.L.; Roos, L.E. Maternal psychological distress & mental health service use during the COVID-19 pandemic. J. Affect. Disord. 2020, 276, 765–774. [Google Scholar] [CrossRef]
- López-Pelayo, H.; Aubin, H.-J.; Drummond, C.; Dom, G.; Pascual, F.; Rehm, J.; Saitz, R.; Scafato, E.; Gual, A. “The post-COVID era”: Challenges in the treatment of substance use disorder (SUD) after the pandemic. BMC Med. 2020, 18, 241. [Google Scholar] [CrossRef]
- Priya, S. Singapore Government Launches COVID-19 Chatbot. 2020. Available online: https://opengovasia.com/singapore-government-launches-covid-19-chatbot/ (accessed on 8 March 2020).



{kind=link}
{kind=link}
| All | Men | Women | p-Value | |
|---|---|---|---|---|
| Subjects, N (%) | 40 (100) | 17 (42.50) | 23 (57.50) | - |
| Age, mean ± SD (years) | 46.45 ± 22.58 | 37.70 ± 21.26 | 52.91 ± 21.73 | 0.10 |
| Area of residence, N (%) Urban Rural | 23 (57.5) 17 (42.5) | 12 (70.59) 5 (20.41) | 11 (47.83) 12 (52.17) | 0.26 |
| Reason, N (%) Useless Personal issues Diffidence Other reasons | 3 (7.5) 3 (7.5) 32 (80) 2 (5) | 1 (5.88) 2 (11.77) 13 (76.47) 1 (5.88) | 2 (8.69) 1 (4.35) 19 (82.61) 1 (4.35) | 0.90 |
| Presence | Absence | Paucity | p-Value | |
|---|---|---|---|---|
| Gender, N (%) Male Female | 8 (72.73) 3 (27.27) | 11 (57.89) 8 (42.11) | 4 (33.33) 8 (66.67) | 0.15 |
| Age, mean ± SD (years) | 49.36 ± 14.19 | 43.05 ± 22.89 | 55.92 ± 25.38 | 0.28 |
| Area of residence, N (%) Urban Rural | 7 (63.64) 4 (36.36) | 13 (68.42) 6 (31.58) | 4 (33.33) 8 (66.67) | 0.14 |
| Telemedicine program, N (%) Only 1th level telepsychology Only tele-monitoring Complete * | 1 (9.1) 0 (0.0) 10 (90.9) | 17 (89.5) 2 (10.5) 0 (0.0) | 8 (66.7) 4 (33.3) 0 (0.0) | <0.001 0.06 <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maresca, G.; Anchesi, S.; Bonanno, L.; Bramanti, A.; Carnazza, L.; Cimino, V.; Corallo, F.; Lo Buono, V.; Giambò, F.M.; Latella, D.; et al. Feasibility, Usability, and Customer Satisfaction of the Tele-COVID19 Project, Sicilian Model. Medicina 2022, 58, 1110. https://doi.org/10.3390/medicina58081110
Maresca G, Anchesi S, Bonanno L, Bramanti A, Carnazza L, Cimino V, Corallo F, Lo Buono V, Giambò FM, Latella D, et al. Feasibility, Usability, and Customer Satisfaction of the Tele-COVID19 Project, Sicilian Model. Medicina. 2022; 58(8):1110. https://doi.org/10.3390/medicina58081110
Chicago/Turabian StyleMaresca, Giuseppa, Smeralda Anchesi, Lilla Bonanno, Alessia Bramanti, Lara Carnazza, Vincenzo Cimino, Francesco Corallo, Viviana Lo Buono, Fabio Mauro Giambò, Desiree Latella, and et al. 2022. "Feasibility, Usability, and Customer Satisfaction of the Tele-COVID19 Project, Sicilian Model" Medicina 58, no. 8: 1110. https://doi.org/10.3390/medicina58081110