
Electrocardiographic Changes Associated with Early Repolarization Pattern in Healthy Young Males


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
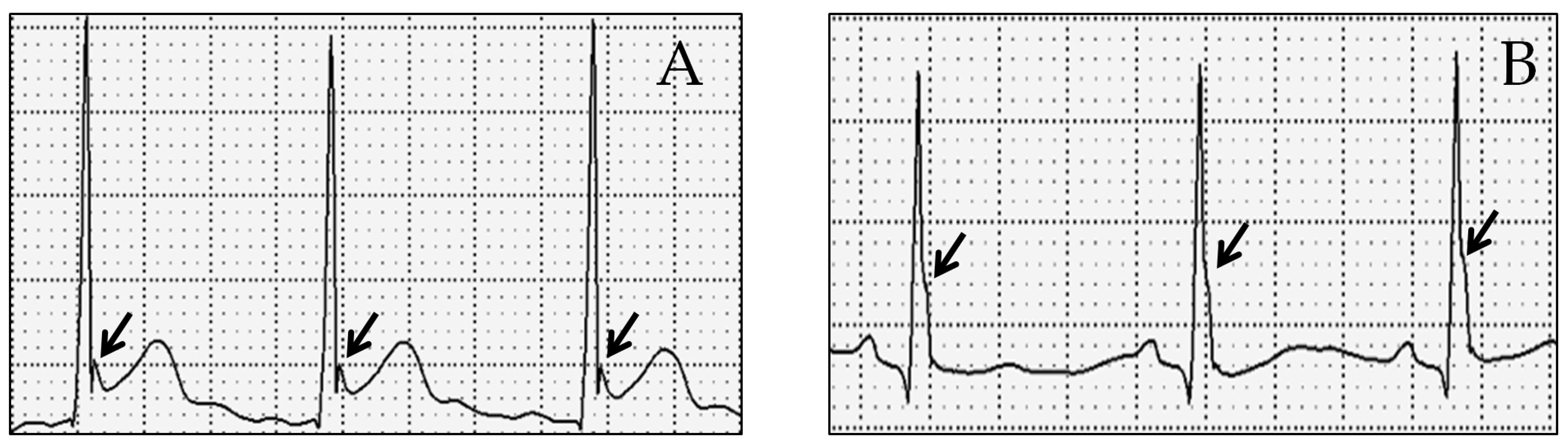
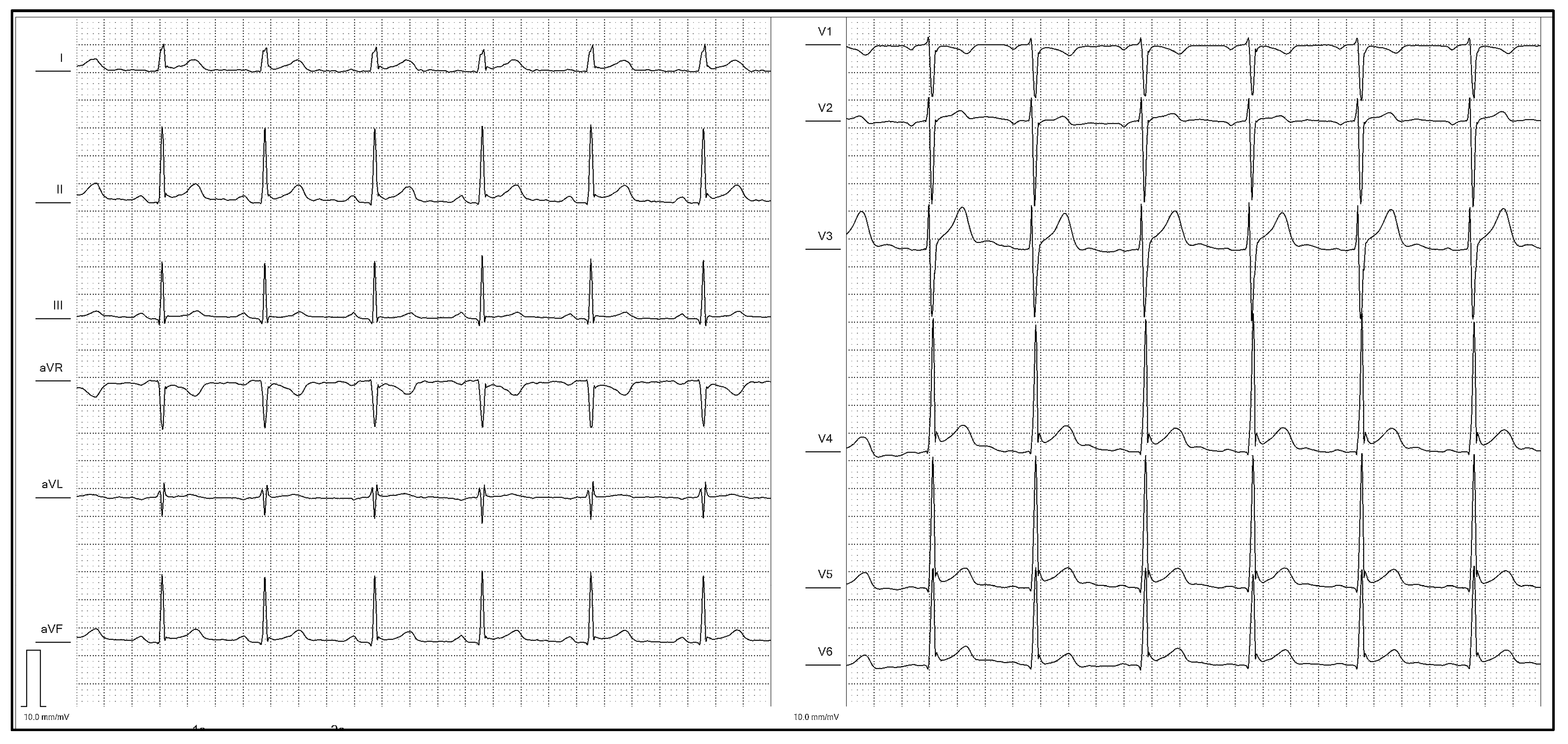
2.2. Resting ECG Recordings: Diagnosis of ERP
2.3. ECG Parameters and Their Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haïssaguerre, M.; Derval, N.; Sacher, F.; Jesel, L.; Deisenhofer, I.; de Roy, L.; Pasquié, J.-L.; Nogami, A.; Babuty, D.; Yli-Mayry, S.; et al. Sudden cardiac arrest associated with early repolarization. N. Engl. J. Med. 2008, 358, 2016–2023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.H.; Lin, X.X.; Cheng, Y.J.; Qiang, C.C.; Zhang, J. Early repolarization pattern and risk for arrhythmia death. J. Am. Coll. Cardiol. 2013, 61, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antzelevitch, C.; Di Diego, J.M. J wave syndromes: Whats new? Trends Cardiovasc. Med. 2021, 32, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Maury, P.; Rollin, A. Prevalence of early repolarisation/J wave patterns in the normal population. J. Electrocardiol. 2013, 5, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.Y.; Hu, N.; Liu, R.; Zhou, H.R.; Gao, W.L.; Quan, X.Q. Worldwide prevalence of early repolarization pattern in general population and physically active individuals. Medicine 2021, 100, e25978. [Google Scholar] [CrossRef] [PubMed]
- Antzelevitch, C.; Yan, G.X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace 2017, 19, 665–694. [Google Scholar] [CrossRef]
- Macfarlane, P.W.; Antzelevitch, C.; Haissaguerre, M.; Huikuri, H.V.; Potse, M.; Rosso, R.; Sacher, F.; Tikkanen, J.T.; Wellens, H.; Yan, G.X. The early repolarization pattern. J. Am. Coll. Cardiol. 2015, 66, 470–477. [Google Scholar] [CrossRef]
- Patton, K.K.; Ellinor, P.T.; Ezekowitz, M.; Kowey, P.; Lubitz, S.A.; Perez, M.; Piccini, J.; Turakhia, M.; Wang, P.; Viskin, S. Electrocardiographic early repolarization. Circulation 2016, 133, 1520–1529. [Google Scholar] [CrossRef]
- Tikkanen, J.T.; Junttila, M.J.; Anttonen, O.; Aro, A.L.; Luttinen, S.; Kerola, T.; Sager, S.J.; Rissanen, H.A.; Myerburg, R.J.; Reunanen, A.; et al. Early repolarization: Electrocardiographic phenotypes associated with favorable long-term outcome. Circulation 2011, 123, 2666–2673. [Google Scholar] [CrossRef] [Green Version]
- Adler, A.; Rosso, R.; Viskin, D.; Halkin, A.; Viskin, S. What do we know about the “malignant form” of early repolarization? J. Am. Coll. Cardiol. 2013, 62, 863–868. [Google Scholar] [CrossRef] [Green Version]
- Bourier, F.; Denis, A.; Cheniti, G.; Lam, A.; Vlachos, K.; Takigawa, M.; Kitamura, T.; Frontera, A.; Duchateau, J.; Pambrun, T.; et al. Early repolarization syndrome: Diagnostic and therapeutic approach. Front. Cardiovasc. Med. 2018, 5, 169. [Google Scholar] [CrossRef] [PubMed]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part III: Intra-ventricular conduction disturbances a scientific statement from the American heart association electrocardiography and ar-rhythmias committee, council on clinical cardiology; the American college of cardiology foundation; and the heart rhythm society endorsed by the international society for computerized electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar] [CrossRef] [Green Version]
- Rautaharju, P.M.; Surawicz, B.; Gettes, L.S. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part IV: The ST segment, T and U waves, and the QT interval a scientific statement from the American heart association electrocardiography and arrhythmias committee, council on clinical cardiology; the American college of cardiology foundation; and the heart rhythm society endorsed by the international society for computerized electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 982–991. [Google Scholar] [CrossRef] [Green Version]
- Hancock, E.W.; Deal, B.J.; Mirvis, D.M.; Okin, P.; Kligfield, P.; Gettes, L.S. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. Part V: Electrocar-diogram changes associated with cardiac chamber hypertrophy a scientific statement from the American heart association electrocardiography and arrhythmias committee, council on clinical cardiology; the American college of cardiology foundation; and the heart rhythm society endorsed by the international society for computerized electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 992–1002. [Google Scholar] [CrossRef] [Green Version]
- Postema, P.G.; De Jong, J.S.; Van der Bilt, I.A.V.; Wilde, A.A. Accurate electrocardiographic assessment of the QT interval: Teach the tangent. Heart Rhythm 2008, 5, 1015–1018. [Google Scholar] [CrossRef] [PubMed]
- Supreeth, R.; Francis, J. Fragmented QRS–its significance. Indian Pacing Electrophysiol. J. 2020, 20, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Johner, N.; Namdar, M.; Shah, D.C. Intra- and interatrial conduction abnormalities: Hemodynamic and arrhythmic significance. J. Interv. Card. Electrophysiol. 2018, 52, 293–302. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Watanabe, H.; Ikami, Y.; Otsuki, S.; Iijima, K.; Yagihara, N.; Sato, A.; Izumi, D.; Minamino, T. Early repolarization and risk of lone atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 565–568. [Google Scholar] [CrossRef]
- Al-Azzam, B.A.; Darbar, D. Atrial fibrillation in inherited channelopathies. Card. Electrophysiol. Clin. 2021, 13, 155–163. [Google Scholar] [CrossRef]
- Szabó, I.A.; Kocsis, L.; László, S.; Fehérvári, L.; Fárr, A.-M.; Frigy, A. Korai repolarizációs mintázatot mutató fiatal férfiak echokardiográfiás jellemzőinek összehasonlító vizsgálata. Orv. Hetil. 2021, 162, 741–745. [Google Scholar] [CrossRef]
- Terho, H.K.; Tikkanen, J.T.; Junttila, J.M.; Anttonen, O.; Kenttä, T.V.; Aro, A.L.; Kerola, T.; Rissanen, H.A.; Reunanen, A.; Huikuri, H.V. Prevalence and prognostic significance of fragmented QRS complex in middle-aged subjects with and without clinical or electrocardiographic evidence of cardiac disease. Am. J. Cardiol. 2014, 114, 141–147. [Google Scholar] [CrossRef]
- Virk, H.U.H.; Farooq, S.; Ghani, A.R.; Arora, S. QRS fragmentation: Its role in sherlocking the arrhythmogenic heart. J. Commun. Hosp. Intern. Med. Perspect. 2016, 6, 31235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seong, C.S.; Gwag, H.B.; Hwang, J.K.; Park, S.J.; Park, K.M.; Kim, J.S.; On, Y.K. Clinical significance of fragmented QRS complexes or J waves in patients with idiopathic ventricular arrhythmias. PLoS ONE 2018, 13, e0194363. [Google Scholar] [CrossRef] [Green Version]
- Yonezu, K.; Shinohara, T.; Sato, H.; Hirota, K.; Kondo, H.; Fukui, A.; Teshima, Y.; Yufu, K.; Nakagawa, M.; Takahashi, N. Role of fragmented QRS and Shanghai score system in recurrence of ventricular fibrillation in patients with early repolarization syndrome. Ann. Noninvasive Electrocardiol. 2021, 26, e12873. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Zhang, Y.; Yan, Q.; Mao, J.; Dong, J.; Ma, C.; Liu, X. Fragmented QRS complex in healthy adults: Prevalence, characteristics, mechanisms, and clinical implications. Int. J. Heart Rhythm 2017, 2, 34–39. [Google Scholar] [CrossRef]
- Tse, G.; Gong, M.; Wong, W.T.; Georgopoulos, S.; Letsas, K.P.; Vassiliou, V.S.; Chan, Y.S.; Yan, B.P.; Wong, S.H.; Wu, W.K.; et al. The T peak-T end interval as an electrocardiographic risk marker of arrhythmic and mortality outcomes: A systematic review and meta-analysis. Heart Rhythm 2017, 14, 1131–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tse, G.; Gong, M.; Li, C.K.H.; Leung, K.S.K.; Georgopoulos, S.; Bazoukis, G.; Letsas, K.P.; Sawant, A.C.; Mugnai, G.; Wong, M.C.; et al. T Peak-T end, T peak-T end/QT ratio and T peak-T end dispersion for risk stratification in Brugada syndrome: A systematic review and meta-analysis. J. Arrhythm. 2018, 34, 587–597. [Google Scholar] [CrossRef]
- Yoon, N.; Hong, S.N.; Cho, J.G.; Jeong, H.K.; Lee, K.H.; Park, H.W. Experimental verification of the value of the T peak-T end interval in ventricular arrhythmia inducibility in an early repolarization syndrome model. J. Cardiovasc. Electrophysiol. 2019, 30, 2098–2105. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| The Dominant Appearance of J Wave | Slurring | Notching | |
| Dominant appearance (in ≥2 contiguous leads) of J wave in the lateral leads (n) | 4 | 12 | |
| Dominant appearance (in ≥2 contiguous leads) of J wave in the inferior leads (n) | 13 | 18 | |
| The type of ST segment slope in leads presenting ERP | Horizontal | Downward | Upward |
| ST segment slope in lateral leads (n) | 7 | 3 | 36 |
| ST segment slope in inferior leads (n) | 13 | 25 | 54 |
| ECG Parameter | “ERP-” Group (n = 182) | “ERP+” Group (n = 38) | Difference between Groups | p-Values |
|---|---|---|---|---|
| Negative terminal P in inferior lead (s) (%) | 19.3 | 34.2 | +14.9 | 0.044 |
| Longest P wave in I, II, III, aVL, aVF (PDurmax) (ms) | 110.4 ± 10.2 | 114.2 ± 9.4 | +3.8 | 0.032 |
| Average P wave duration (ms) | 101.5 ± 9.2 | 106.8 ± 9.9 | +5.3 | 0.004 |
| Fragmented QRS (notching of QRS <120 ms in at least one lead, excepting aVR) (%) | 67.6 | 92.1 | +24.5 | 0.002 |
| Fragmented QRS (notching of QRS <120 ms in at least two contigous leads, excepting aVR) (%) | 49.5 | 73.7 | +24.2 | 0.006 |
| Intrinsicoid deflection in V5 (ms) | 43.4 ± 7.3 | 41.0 ± 6.3 | −2.4 | 0.045 |
| QRS duration in II (ms) | 92.2 ± 15.3 | 76.9 ± 11.9 | −15.33 | <0.001 |
| QRS duration in V2 (ms) | 96.8 ± 11.9 | 91.8 ± 8.6 | −5.0 | 0.003 |
| QRS duration in V5 (ms) | 92.1 ± 12.9 | 78.5 ± 9.4 | −13.6 | <0.001 |
| Max of QRS duration from lead II, V2, V5 (ms) | 98.7 ± 11.8 | 92.5 ± 8.0 | −6.2 | <0.001 |
| Sokolow-Lyon index for RVH (R in V1 or V2 + S in V5 or V6) (mm) | 11.0 ± 4.0 | 9.7 ± 3.3 | −1.3 | 0.043 |
| Male type ECG pattern (ST-elevation > 1 mm in V2-4) (%) | 38.6 | 57.9 | +19.3 | 0.029 |
| QT max/QRS in V5 | 4.1 ± 0.6 | 4.7 ± 0.6 | +0.6 | <0.001 |
| QT max corrected/QRS in V5 | 4.5 ± 0.8 | 5.4 ± 1.1 | +0.9 | <0.001 |
| QT dispersion = difference of max and min QT in I, aVF, V2 (ms) | 25.1 ± 12.5 | 16.7 ± 9.9 | −8.4 | <0.001 |
| QT dispersion corrected (Bazett’s formula) (ms) | 26.2 ± 12.5 | 17.9 ± 11.4 | 8.3 | <0.001 |
| QT dispersion/QT average | 0.070 ± 0.034 | 0.046 ± 0.028 | 0.024 | <0.001 |
| Tpeak—Tend average (ms) | 70.9 ± 8.1 | 67.8 ± 8.0 | 3.1 | 0.036 |
| Tpeak—Tend average corrected (Bazett’s formula) (ms) | 77.1 ± 10.4 | 72.4 ± 10.5 | 4.7 | 0.016 |
| Tpeak—Tend max corrected (Bazett’s formula) (ms) | 90.3 ± 14.6 | 83.4 ± 13.1 | −6.9 | 0.005 |
| Tpeak—Tend average/QT average | 0.202 ± 0.022 | 0.190 ± 0.019 | −0.012 | 0.001 |
| Atrial premature beats (%) | 0.6 | 7.9 | +7.3 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frigy, A.; Gábor-Kelemen, H.; László, S.A.; Szabó, I.A.; Kocsis, L. Electrocardiographic Changes Associated with Early Repolarization Pattern in Healthy Young Males. Medicina 2022, 58, 1048. https://doi.org/10.3390/medicina58081048
Frigy A, Gábor-Kelemen H, László SA, Szabó IA, Kocsis L. Electrocardiographic Changes Associated with Early Repolarization Pattern in Healthy Young Males. Medicina. 2022; 58(8):1048. https://doi.org/10.3390/medicina58081048
Chicago/Turabian StyleFrigy, Attila, Hunor Gábor-Kelemen, Szabolcs Attila László, István Adorján Szabó, and Lóránd Kocsis. 2022. "Electrocardiographic Changes Associated with Early Repolarization Pattern in Healthy Young Males" Medicina 58, no. 8: 1048. https://doi.org/10.3390/medicina58081048