
The Significance of FDG PET/CT–Derived Parameters in Determining Prognosis of Cases with Pancreatic Adenocarcinoma: A Prospective Study

 and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.1.1. Inclusion Criteria
- Patients aged between 18 and 70 years.
- Patients who had radiotherapy and chemotherapy.
- Patients who had initial FDG PET/CT staging images with an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2.
- Patients who had adequate bone marrow reserve (WBCs count 3.5 × 109/L, ANC count 1.5 × 109/L, platelets 100 × 109/L, and hemoglobin 10 g/dL).
- Patients who had normal renal functions (measured creatinine clearance 60 mL/min).
- All patients had histologic or cytologic evidence of pancreatic adenocarcinoma.
2.1.2. Exclusion Criteria
- Patients with severe arrhythmia, prior surgery, peripheral neuropathy, chemotherapy or radiotherapy, symptomatic heart failure, active infection.
- Pregnant or lactating mothers.
- Patients with other malignant diseases.
- Patients with other comorbid diseases.
2.2. Intervention
2.2.1. Pre- and on-Treatment Evaluation
2.2.2. PET/CT Protocol
2.2.3. Image Analysis
2.2.4. Measurement of Serum MMP-2 by ELISA Technique
2.2.5. Treatment Protocol
Surgery
Chemotherapy
Dose Adjustment of FOLFIRINOX
Chemoradiotherapy
2.2.6. Evaluation during Concurrent Gemcitabine—IMRT External Beam Radiation Therapy
2.2.7. Restaging
2.3. Outcomes
2.4. Time Frame
2.5. Statistical Analysis
3. Results
3.1. Patients’ and Tumors’ Characteristics
3.2. FDG PET/CT Parameters Results
3.3. Tumor Glycolytic Activity
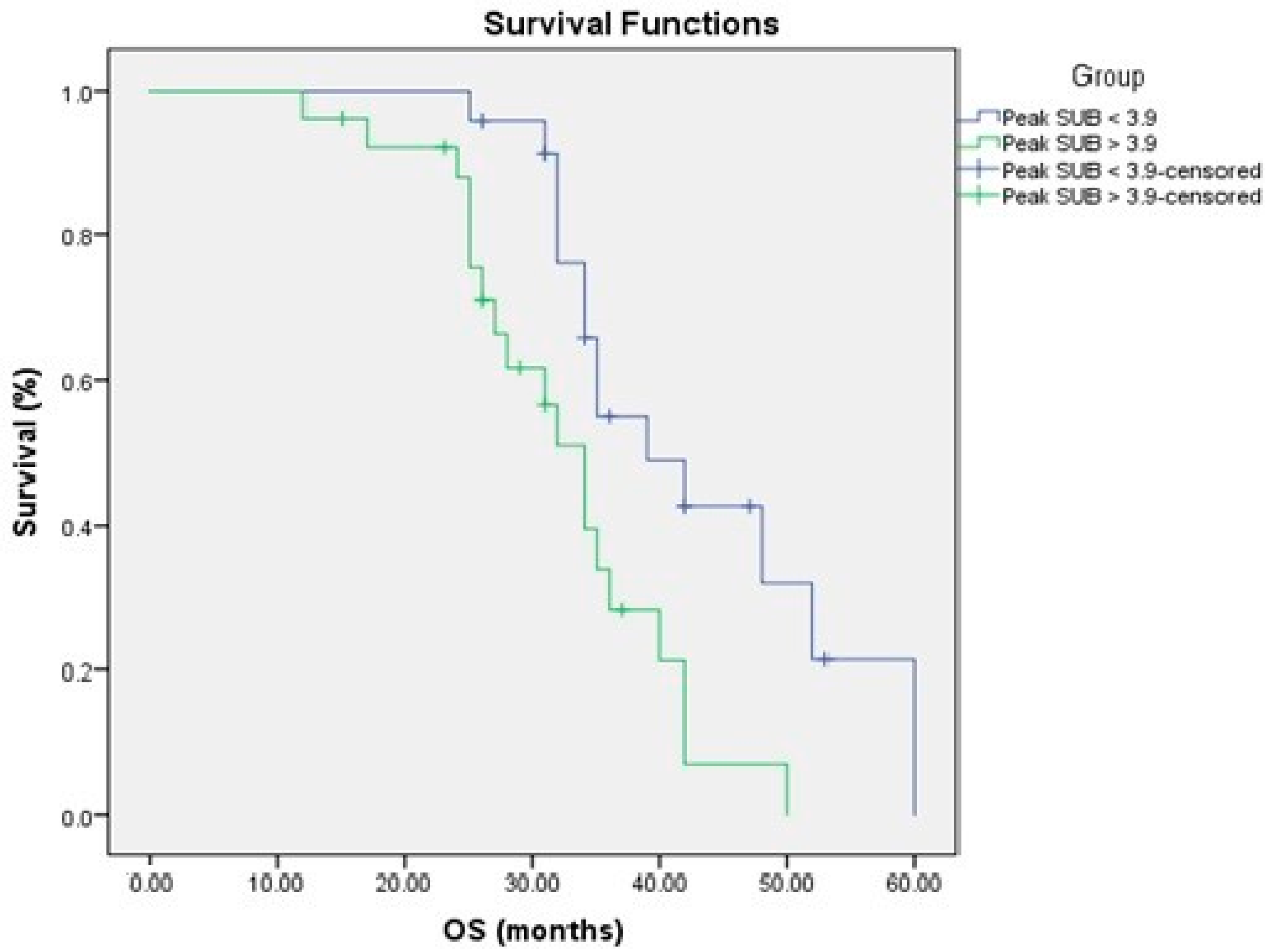
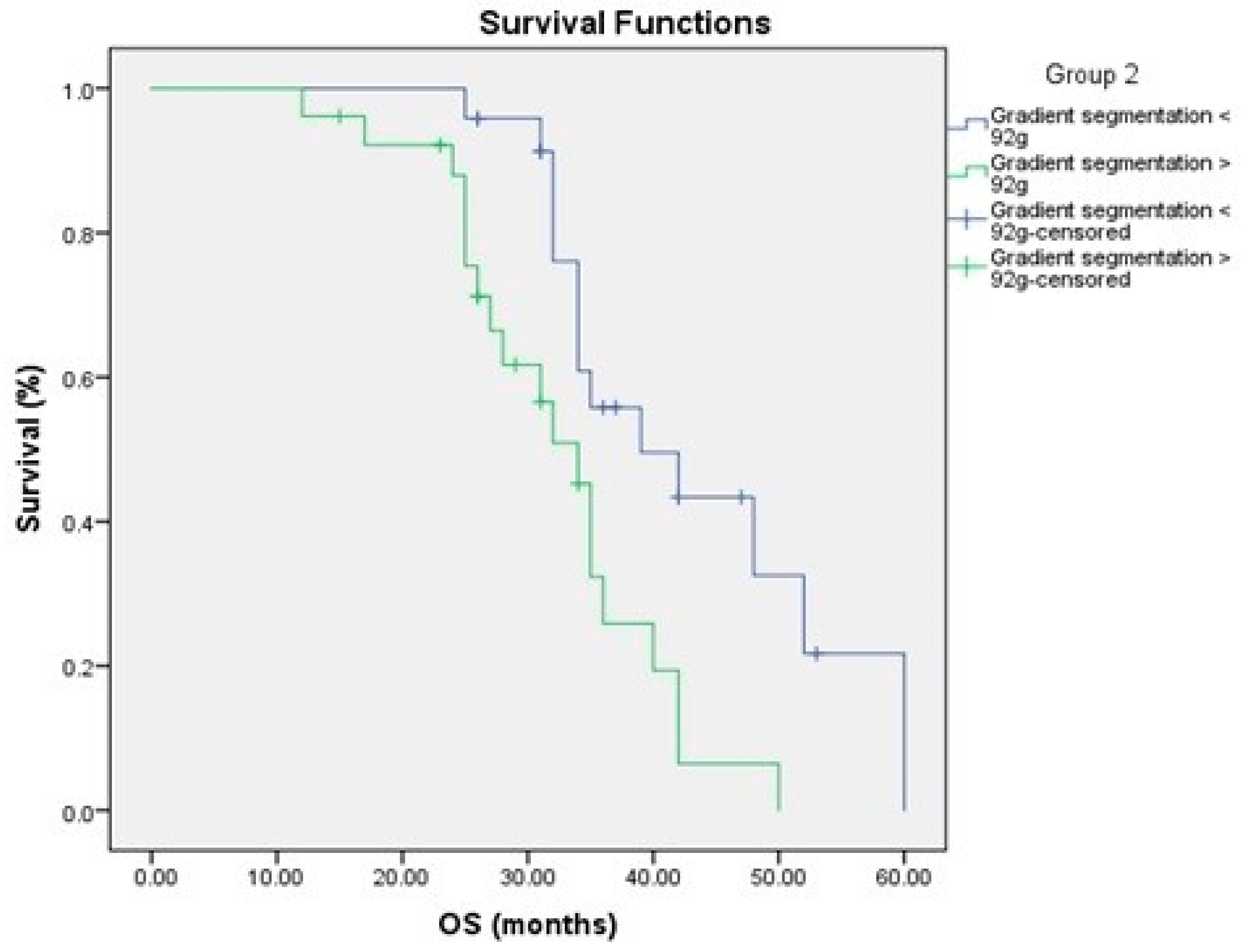
3.4. Relationship to Survival
3.5. Serum MMP-2 Levels
4. Discussion
5. Conclusions
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Dreyer, S.B.; Upstill-Goddard, R.; Legrini, A.; Biankin, A.V.; Jamieson, N.B.; Chang, D.K.; Australian Pancreatic Genome Initiative; Glasgow Precision Oncology Laboratory. Genomic and Molecular Analyses Identify Molecular Subtypes of Pancreatic Cancer Recurrence. Gastroenterology 2022, 162, 320–324.e4. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Kavaliauskas, P.; Dulskas, A.; Kildusiene, I.; Arlauskas, R.; Stukas, R.; Smailyte, G. Trends in Pancreatic Cancer Incidence and Mortality in Lithuania, 1998–2015. Int. J. Environ. Res. Public Health 2022, 19, 949. [Google Scholar] [CrossRef]
- Connor, A.A.; Gallinger, S. Pancreatic cancer evolution and heterogeneity: Integrating omics and clinical data. Nat. Rev. Cancer 2022, 22, 131–142. [Google Scholar] [CrossRef]
- Karakas, Y.; Lacin, S.; Yalcin, S. Recent advances in the management of pancreatic adenocarcinoma. Expert Rev. Anticancer Ther. 2018, 18, 51–62. [Google Scholar] [CrossRef]
- Yousaf, M.N.; Ehsan, H.; Wahab, A.; Muneeb, A.; Chaudhary, F.S.; Williams, R.; Haas, C.J. Endoscopic retrograde cholangiopancreatography guided interventions in the management of pancreatic cancer. World J. Gastrointest. Endosc. 2020, 12, 323–340. [Google Scholar] [CrossRef] [PubMed]
- Pu, Y.; Wang, C.; Zhao, S.; Xie, R.; Zhao, L.; Li, K.; Yang, C.; Zhang, R.; Tian, Y.; Tan, L.; et al. The clinical application of 18F-FDG PET/CT in pancreatic cancer: A narrative review. Transl. Cancer Res. 2021, 10, 3560–3575. [Google Scholar] [CrossRef]
- Huang, S.; Chong, H.; Sun, X.; Wu, Z.; Jia, Q.; Zhang, Y.; Lan, X. The Value of 18F-FDG PET/CT in Diagnosing Pancreatic Lesions: Comparison with CA19-9, Enhanced CT or Enhanced MR. Front. Med. 2021, 8, 668697. [Google Scholar] [CrossRef]
- Parlak, C.; Topkan, E.; Onal, C.; Reyhan, M.; Selek, U. Prognostic value of gross tumor volume delineated by FDG-PET-CT based radiotherapy treatment planning in patients with locally advanced pancreatic cancer treated with chemoradiotherapy. Radiat. Oncol. 2012, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Topkan, E.; Parlak, C.; Kotek, A.; Yapar, A.F.; Pehlivan, B. Predictive value of metabolic 18FDG-PET response on outcomes in patients with locally advanced pancreatic carcinoma treated with definitive concurrent chemoradiotherapy. BMC Gastroenterol. 2011, 11, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, J.; Abisoye-Ogunniyan, A.; Metcalf, K.J.; Werb, Z. Concepts of extracellular matrix remodelling in tumour progression and metastasis. Nat. Commun. 2020, 11, 5120. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Li, H. Prognostic values of tumoral MMP2 and MMP9 overexpression in breast cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 149. [Google Scholar] [CrossRef] [PubMed]
- Jakubowska, K.; Pryczynicz, A.; Januszewska, J.; Sidorkiewicz, I.; Kemona, A.; Niewiński, A.; Lewczuk, Ł.; Kędra, B.; Guzińska-Ustymowicz, K. Expressions of Matrix Metalloproteinases 2, 7, and 9 in Carcinogenesis of Pancreatic Ductal Adenocarcinoma. Dis. Markers 2016, 2016, 9895721. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; O, J.H.; Choi, M.; Choi, J.Y. Impact of F-18 Fluorodeoxyglucose PET/CT and PET/MRI on Initial Staging and Changes in Management of Pancreatic Ductal Adenocarcinoma: A Systemic Review and Meta-Analysis. Diagnostics 2020, 10, 952. [Google Scholar] [CrossRef]
- Zhu, D.; Wang, L.; Zhang, H.; Chen, J.; Wang, Y.; Byanju, S.; Liao, M. Prognostic value of 18F-FDG-PET/CT parameters in patients with pancreatic carcinoma: A systematic review and meta-analysis. Medicine 2017, 96, e7813. [Google Scholar] [CrossRef]
- Evangelista, L.; Zucchetta, P.; Moletta, L.; Serafini, S.; Cassarino, G.; Pegoraro, N.; Bergamo, F.; Sperti, C.; Cecchin, D. The role of FDG PET/CT or PET/MRI in assessing response to neoadjuvant therapy for patients with borderline or resectable pancreatic cancer: A systematic literature review. Ann. Nucl. Med. 2021, 35, 767–776. [Google Scholar] [CrossRef]
- Zhang, Q.; Zeng, L.; Chen, Y.; Lian, G.; Qian, C.; Chen, S.; Li, J.; Huang, K. Pancreatic Cancer Epidemiology, Detection, and Management. Gastroenterol. Res. Pract. 2016, 2016, 8962321. [Google Scholar] [CrossRef] [Green Version]
- Muniraj, T.; Jamidar, P.A.; Aslanian, H.R. Pancreatic cancer: A comprehensive review and update. Disease Month 2013, 59, 368–402. [Google Scholar] [CrossRef]
- Hicks, A.M.; Chou, J.; Capanu, M.; Lowery, M.A.; Yu, K.H.; O’Reilly, E.M. Pancreas Adenocarcinoma: Ascites, Clinical Manifestations, and Management Implications. Clin. Colorectal Cancer 2016, 15, 360–368. [Google Scholar] [CrossRef] [Green Version]
- Hyun, S.H.; Kim, H.S.; Choi, S.H.; Choi, D.W.; Lee, J.K.; Lee, K.H.; Park, J.O.; Lee, K.-H.; Kim, B.-T.; Choi, J.Y. Intratumoral heterogeneity of 18FFDG uptake predicts survival in patients with pancreatic ductal adenocarcinoma. Eur. J. Nucl. Med. Mol. 2016, 43, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.J.; Lee, J.W.; Kang, B.; Song, S.Y.; Lee, J.D.; Lee, J.-H. Prognostic significance of volume-based FDG PET/CT parameters in patients with locally advanced pancreatic cancer treated with chemoradiation therapy. Yonsei Med. J. 2014, 55, 1498–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casneuf, V.; Delrue, L.; Kelles, A.; van Damme, N.; van Huysse, J.; Berrevoet, F.; de Vos, M.; Duyck, P.; Peeters, M. Is combined 18Ffluorodeoxyglucose-positron emission tomography/computed tomography superior to positron emission tomography or computed tomography alone for diagnosis, staging and restaging of pancreatic lesions? Acta Gastroenterol. Belg. 2007, 70, 331–338. [Google Scholar] [PubMed]
- Heinrich, S.; Goerres, G.W.; Schäfer, M.; Sagmeister, M.; Bauerfeind, P.; Pestalozzi, B.C.; Hany, T.F.; von Schulthess, G.K.; Clavien, P.-A. Positron emission tomography/computed tomography influences on the management of resectable pancreatic cancer and its cost-effectiveness. Ann. Surg. 2005, 242, 235–243. [Google Scholar] [CrossRef]
- Moon, S.Y.; Joo, K.R.; So, Y.R.; Lim, J.U.; Cha, J.M.; Shin, H.P.; Yang, Y.-J. Predictive value of maximum standardized uptake value (SUVmax) on 18F-FDG PET/CT in patients with locally advanced or metastatic pancreatic cancer. Clin. Nucl. Med. 2013, 38, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Yu, L.J.; Li, X.Y. Prognostic value of metabolic tumor volume on 18F-FDG PET/CT imaging in patients with pancreatic cancer. Chin. J. Nucl. Med. Mol. Imaging 2016, 36, 408–412. [Google Scholar]
- Sun, Y.; Duan, Q.; Wang, S.; Zeng, Y.; Wu, R. Diagnosis of pancreatic cancer using 18F-FDG PET/CT and CA19-9 with SUVmax association to clinical characteristics. JBUON 2015, 20, 452–459. [Google Scholar]
- Davison, J.; Mercier, G.; Russo, G.; Subramaniam, R.M. PET-based primary tumor volumetric parameters and survival of patients with non-small cell lung carcinoma. AJR 2013, 200, 635–640. [Google Scholar] [CrossRef]
- Chang, K.-P.; Tsang, N.-M.; Liao, C.-T.; Hsu, C.-L.; Chung, M.-J.; Lo, C.-W.; Chan, S.-C.; Ng, S.-H.; Wang, H.-M.; Yen, T.-C. Prognostic significance of 18F-FDG PET parameters and plasma Epstein-Barr virus DNA load in patients with nasopharyngeal carcinoma. J. Nucl. Med. 2012, 53, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Schellenberg, D.; Quon, A.; Minn, A.Y.; Graves, E.E.; Kunz, P.; Ford, J.M.; Fisher, G.A.; Goodman, K.A.; Koong, A.C.; Chang, D.T. 18Fluorodeoxyglucose PET is prognostic of progressionfree and overall survival in locally advanced pancreas cancer treated with stereotactic radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 1420–1425. [Google Scholar] [CrossRef]
- Lee, J.W.; Kang, C.M.; Choi, H.J.; Lee, W.J.; Song, S.Y.; Lee, J.-H.; Lee, J.D. Prognostic value of metabolic tumor volume and total lesion glycolysis on preoperative 18F-FDG PET/CT in patients with pancreatic cancer. J. Nucl. Med. 2014, 55, 898–904. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.-X.; Chen, T.; Wang, W.-Q.; Wu, C.-T.; Liu, C.; Long, J.; Xu, J.; Zhang, Y.-J.; Chen, R.-H.; Liu, L.; et al. Metabolic tumor burden assessed by 18F-FDG PET/CT associated with serum CA19-9 predicts pancreatic cancer outcome after resection. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1093–1102. [Google Scholar] [CrossRef]
- Chan, A.K.; Bruce, J.I.; Siriwardena, A.K. Glucose metabolic phenotype of pancreatic cancer. World J. Gastroenterol. 2016, 22, 3471–3485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, X.; Liu, X.; Wang, H.; Yang, X.; Gu, Y. Glycolysis in the progression of pancreatic cancer. Am. J. Cancer Res. 2022, 12, 861–872. [Google Scholar] [PubMed]
- Curcio, C.; Brugiapaglia, S.; Bulfamante, S.; Follia, L.; Cappello, P.; Novelli, F. The Glycolytic Pathway as a Target for Novel Onco-Immunology Therapies in Pancreatic Cancer. Molecules 2021, 26, 1642. [Google Scholar] [CrossRef]
- Choi, H.J.; Kang, C.M.; Lee, W.J.; Song, S.Y.; Cho, A.; Yun, M.; Lee, J.D.; Kim, J.H.; Lee, J.-H. Prognostic value of 18F-fluorodeoxyglucose positron emission tomography in patients with resectable pancreatic cancer. Yonsei Med. J. 2013, 54, 1377–1383. [Google Scholar] [CrossRef] [Green Version]
- Nakata, B.; Nishimura, S.; Ishikawa, T.; Ohira, M.; Nishino, H.; Kawabe, J.; Ochi, H.; Hirakawa, K. Prognostic predictive value of 18F-fluorodeoxyglucose positron emission tomography for patients with pancreatic cancer. Int. J. Oncol. 2001, 19, 53–58. [Google Scholar] [CrossRef]
- Sperti, C.; Pasquali, C.; Chierichetti, F.; Ferronato, A.; Decet, G.; Pedrazzoli, S. 18-Fluorodeoxyglucose positron emission tomography in predicting survival of patients with pancreatic carcinoma. J. Gastrointest. Surg. 2003, 7, 953–959. [Google Scholar] [CrossRef]
- Łukaszewicz-Zając, M.; Gryko, M.; Pączek, S.; Szmitkowski, M.; Kędra, B.; Mroczko, B. Matrix metalloproteinase 2 (MMP-2) and its tissue inhibitor 2 (TIMP-2) in pancreatic cancer (PC). Oncotarget 2019, 10, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, H.; Yamamoto, H.; Itoh, F.; Nakamura, H.; Min, Y.; Horiuchi, S.; Iku, S.; Sasaki, S.; Imai, K. Association of matrilysin mRNA expression with K-ras mutations and progression in pancreatic ductal adenocarcinomas. Carcinogenesis 2001, 22, 1049–1052. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, K.; Nishiyama, T.; Hori, Y. Gemcitabine Enhances Kras-MEK-Induced Matrix Metalloproteinase-10 Expression Via Histone Acetylation in Gemcitabine-Resistant Pancreatic Tumor-initiating Cells. Pancreas 2017, 46, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javadrashid, D.; Baghbanzadeh, A.; Derakhshani, A.; Leone, P.; Silvestris, N.; Racanelli, V.; Solimando, A.G.; Baradaran, B. Pancreatic Cancer Signaling Pathways, Genetic Alterations, and Tumor Microenvironment: The Barriers Affecting the Method of Treatment. Biomedicines 2021, 9, 373. [Google Scholar] [CrossRef] [PubMed]
- Niland, S.; Riscanevo, A.X.; Eble, J.A. Matrix Metalloproteinases Shape the Tumor Microenvironment in Cancer Progression. Int. J. Mol. Sci. 2021, 23, 146. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FDG Uptake in the Primary Pancreatic Tumor | Chi-Square | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Peak SUV < 3.9 | Peak SUV ≥ 3.9 | Total | |||||||
| N | % | N | % | N | % | X2 | p-Value | ||
| Age | <60 | 10 | 20% | 11 | 22% | 21 | 42% | 0.012 | 0.963 |
| >60 | 14 | 28% | 15 | 30% | 29 | 58% | |||
| Sex | Male | 11 | 22% | 17 | 34% | 28 | 56% | 1.938 | 0.164 |
| Female | 13 | 26% | 9 | 18% | 22 | 44% | |||
| ECOG performance status | 0 | 3 | 6% | 1 | 2% | 4 | 8% | 1.271 | 0.260 |
| 1 | 21 | 42% | 25 | 50% | 46 | 92% | |||
| Tumor Stage | II | 3 | 6% | 0 | 0% | 3 | 6% | 3.928 | 0.140 |
| III | 11 | 22% | 11 | 22% | 22 | 44% | |||
| IV | 10 | 20% | 15 | 30% | 25 | 50% | |||
| Tumor Grade | Grade I | 0 | 0% | 0 | 0% | 0 | 0% | 6.462 | 0.011 * |
| Grade II | 14 | 28% | 6 | 12% | 20 | 40% | |||
| Grade III | 10 | 20% | 20 | 40% | 30 | 60% | |||
| Therapy | None | 0 | 0% | 3 | 6% | 3 | 6% | 6.029 | 0.110 |
| chemotherapy | 7 | 14% | 8 | 16% | 15 | 30% | |||
| chemoradiotherapy | 14 | 28% | 15 | 30% | 29 | 58% | |||
| Chemoradiotherapy + surgery | 3 | 6% | 0 | 0% | 3 | 6% | |||
| glycolytic activity | gradient segmentation > 92 g | 4 | 8% | 20 | 40% | 24 | 48% | 18.147 | 0.001 * |
| gradient segmentation ≤ 92 g | 20 | 40% | 6 | 12% | 26 | 52% | |||
| 50% SUVmax threshold | >82 | 2 | 4% | 21 | 42% | 23 | 46% | 26.631 | 0.001 * |
| ≤82 | 22 | 44% | 5 | 10% | 27 | 54% | |||
| metabolic tumor volume | <3 cm3 | 9 | 18% | 1 | 2% | 10 | 20% | 18.486 | 0.001 * |
| ≥3 cm3–5 cm3 | 10 | 20% | 6 | 12% | 16 | 32% | |||
| >5 cm3–8 cm3 | 5 | 10% | 9 | 18% | 14 | 28% | |||
| >8 cm3 | 0 | 0.00% | 10 | 20% | 10 | 20% | |||
| Mortality | Alive | 5 | 10% | 5 | 10% | 10 | 20% | 0.023 | 0.887 |
| Died | 19 | 38% | 21 | 42% | 40 | 80% | |||
| Tumor Glycolytic Activity Gradient Segmentation > 92 g | Gradient Segmentation ≤ 92 g | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | N | X2 | p-Value | ||
| Age | <60 | 9 | 18% | 12 | 24% | 21 | 42% | 0.381 | 0.536 |
| >60 | 15 | 30% | 14 | 28% | 29 | 58% | |||
| Sex | Male | 13 | 26% | 15 | 30% | 28 | 56% | 0.063 | 0.802 |
| Female | 11 | 22% | 11 | 22% | 22 | 44% | |||
| ECOG performance status | 0 | 2 | 4% | 2 | 4% | 4 | 8% | 0.013 | 0.933 |
| 1 | 22 | 44% | 24 | 48% | 35 | 92% | |||
| Tumor Stage | II | 0 | 0% | 3 | 6% | 3 | 6% | 5.469 | 0.077 * |
| III | 10 | 20% | 12 | 24% | 22 | 44% | |||
| IV | 14 | 28% | 11 | 22% | 25 | 50% | |||
| Tumor Grade | Grade I | 0 | 0% | 0 | 0.00% | 0 | 0% | 5.256 | 0.033 * |
| Grade II | 7 | 14% | 13 | 26% | 20 | 40% | |||
| Grade III | 17 | 34% | 13 | 26% | 30 | 60% | |||
| Therapy | None | 2 | 4% | 1 | 2% | 3 | 6% | 5.786 | 0.022 * |
| Chemotherapy | 10 | 20% | 5 | 10% | 15 | 30% | |||
| Chemoradiotherapy | 12 | 24% | 17 | 34% | 29 | 58% | |||
| Chemoradiotherapy + surgery | 0 | 0 | 3 | 6 | 3 | 6% | |||
| SUVmax | >6.5 | 17 | 34% | 9 | 18% | 26 | 52% | 6.562 | 0.010 * |
| ≤6.5 | 7 | 14% | 17 | 34% | 24 | 48% | |||
| 50% SUVmax threshold | >82 | 18 | 36% | 5 | 10% | 23 | 46% | 15.629 | 0.001 * |
| ≤82 | 6 | 12% | 21 | 42% | 27 | 54% | |||
| metabolic tumor volume | <3 cm3 | 3 | 6% | 7 | 14% | 10 | 20% | 5.409 | 0.020 * |
| ≥3 cm3–5 cm3 | 6 | 12% | 10 | 20% | 16 | 32% | |||
| >5 cm3–8 cm3 | 8 | 16% | 6 | 12 | 14 | 28% | |||
| >8 cm3 | 7 | 14% | 3 | 6% | 10 | 20% | |||
| Mortality | Alive | 1 | 2% | 9 | 18% | 10 | 20% | 7.231 | 0.007 * |
| Died | 23 | 46% | 17 | 34% | 40 | 80% | |||
| Group | Mean | Median | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% CI | Estimate | Std. Error | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
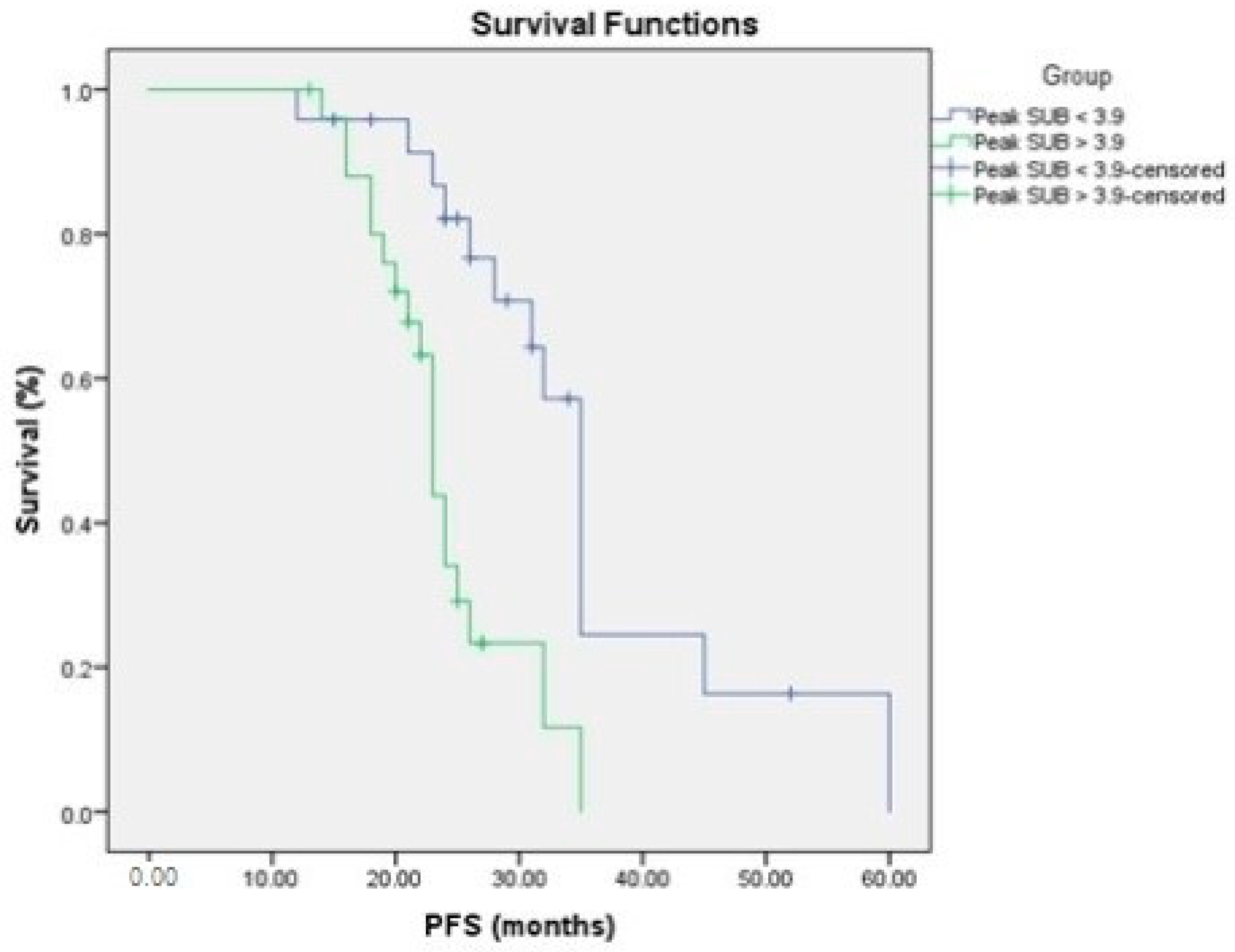
| Peak SUV < 3.9 | 35.877 | 3.334 | 29.343 | 42.412 | 35.000 | 1.089 | 32.865 | 37.135 |
| Peak SUV > 3.9 | 24.092 | 1.319 | 21.507 | 26.677 | 23.000 | 0.543 | 21.936 | 24.064 |
| Overall | 30.157 | 2.089 | 26.063 | 34.252 | 28.000 | 3.786 | 20.580 | 35.420 |
| Group 2 | Mean | Median | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% CI | Estimate | Std. Error | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
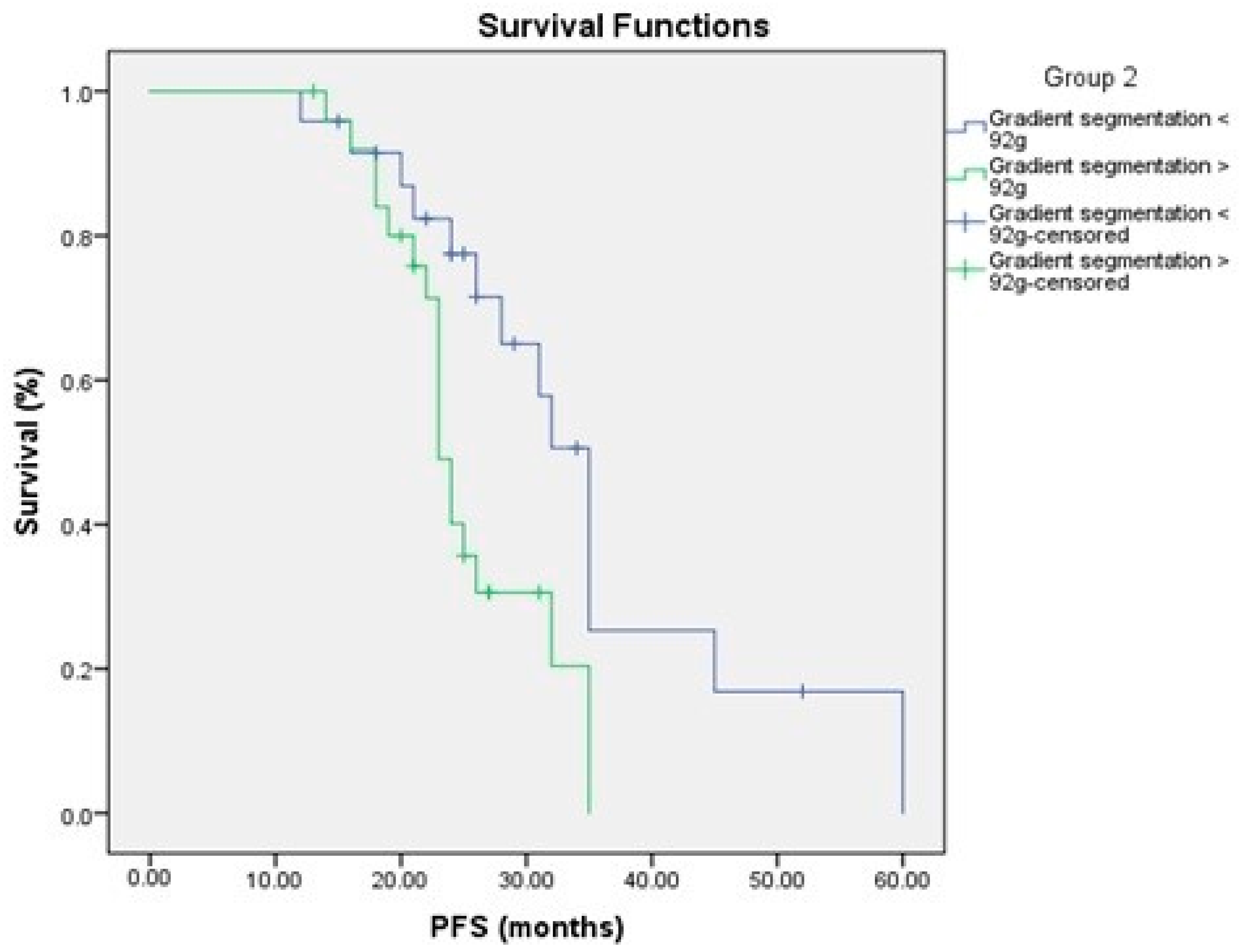
| Gradient segmentation < 92 g | 34.915 | 3.564 | 27.929 | 41.901 | 35.000 | 1.483 | 32.094 | 37.906 |
| Gradient segmentation > 92 g | 25.365 | 1.372 | 22.676 | 28.054 | 23.000 | 0.667 | 21.693 | 24.307 |
| Overall | 30.157 | 2.089 | 26.063 | 34.252 | 28.000 | 3.786 | 20.580 | 35.420 |
| Group | Mean | Median | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% CI | Estimate | Std. Error | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Peak SUV < 3.9 | 40.216 | 2.785 | 37.572 | 48.546 | 39.000 | 3.990 | 31.180 | 46.820 |
| Peak SUV > 3.9 | 31.586 | 1.865 | 28.710 | 36.410 | 34.000 | 1.948 | 30.183 | 37.817 |
| Overall | 37.831 | 1.878 | 34.151 | 41.512 | 35.000 | 1.260 | 32.531 | 37.469 |
| Group 2 | Mean | Median | ||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | Std. Error | 95% CI | Estimate | Std. Error | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||
| Gradient segmentation < 92 g | 43.150 | 2.802 | 37.658 | 48.643 | 39.000 | 6.472 | 26.314 | 51.686 |
| Gradient segmentation > 92 g | 32.419 | 1.935 | 28.626 | 36.211 | 34.000 | 1.822 | 30.429 | 37.571 |
| Overall | 37.831 | 1.878 | 34.151 | 41.512 | 35.000 | 1.260 | 32.531 | 37.469 |
| Serum MMP-2 | Chi-Square | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal Group (n = 38) | High Group (n = 12) | Total | |||||||
| N | % | N | % | N | % | X2 | p-Value | ||
| Age (years) | <60 | 15 | 39.5 | 6 | 50 | 21 | 42% | 0.095 | 0.758 |
| >60 | 23 | 60.5 | 6 | 50 | 29 | 58% | |||
| Sex | Male | 18 | 47.4 | 5 | 41.7 | 23 | 46% | 0.12 | 0.73 |
| Female | 20 | 52.6 | 7 | 58.3 | 27 | 54% | |||
| ECOG performance status | 0 | 13 | 34.2 | 0 | 0 | 13 | 26% | 5.548 | 0.019 * |
| 1 | 25 | 65.8 | 12 | 100 | 37 | %74 | |||
| Tumor Stage | II | 2 | 5.3 | 1 | 8.3 | 3 | 6% | 6.267 | 0.043 * |
| III | 25 | 65.8 | 3 | 25 | 28 | 56% | |||
| IV | 11 | 29 | 8 | 66.7 | 19 | 38% | |||
| Tumor Grade | Grade I | 7 | 18.4 | 3 | 25 | 10 | 20% | 0.747 | 0.689 |
| Grade II | 18 | 47.4 | 4 | 33.3 | 22 | 44% | |||
| Grade III | 13 | 34.2 | 5 | 41.7 | 18 | 36% | |||
| Therapy | None | 2 | 5.3 | 1 | 8.3 | 3 | 6% | 0.883 | 0.83 |
| chemotherapy | 7 | 18.4 | 3 | 25 | 10 | 20% | |||
| chemoradiotherapy | 18 | 47.4 | 6 | 50 | 14 | 28% | |||
| Chemoradiotherapy + surgery | 11 | 28.9 | 2 | 16.7 | 13 | 26% | |||
| glycolytic activity | gradient segmentation > 92 g | 14 | 36.8 | 9 | 75 | 23 | 46% | 5.346 | 0.021 * |
| gradient segmentation ≤ 92 g | 24 | 63.2 | 3 | 25 | 27 | 54% | |||
| 50% SUVmax threshold | >82 | 13 | 31.6 | 10 | 83.3 | 23 | 46% | 8.860 | 0.003 * |
| ≤82 | 25 | 36.8 | 2 | 16.7 | 27 | 54% | |||
| metabolic tumor volume | <3 cm3 | 9 | 23.7 | 1 | 8.3 | 10 | 20% | 2.332 | 0.506 |
| ≥3 cm3–5 cm3 | 17 | 44.7 | 7 | 58.3 | 24 | 48% | |||
| >5 cm3–8 cm3 | 9 | 23.7 | 2 | 16.7 | 11 | 22% | |||
| >8 cm3 | 3 | 7.9 | 2 | 16.7 | 5 | 10% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mokhtar, H.M.; Youssef, A.; Naguib, T.M.; Magdy, A.A.; Salama, S.A.; Kabel, A.M.; Sabry, N.M. The Significance of FDG PET/CT–Derived Parameters in Determining Prognosis of Cases with Pancreatic Adenocarcinoma: A Prospective Study. Medicina 2022, 58, 1027. https://doi.org/10.3390/medicina58081027
Mokhtar HM, Youssef A, Naguib TM, Magdy AA, Salama SA, Kabel AM, Sabry NM. The Significance of FDG PET/CT–Derived Parameters in Determining Prognosis of Cases with Pancreatic Adenocarcinoma: A Prospective Study. Medicina. 2022; 58(8):1027. https://doi.org/10.3390/medicina58081027
Chicago/Turabian StyleMokhtar, Hwaida M., Amira Youssef, Tamer M. Naguib, Amr A. Magdy, Samir A. Salama, Ahmed M. Kabel, and Nesreen M. Sabry. 2022. "The Significance of FDG PET/CT–Derived Parameters in Determining Prognosis of Cases with Pancreatic Adenocarcinoma: A Prospective Study" Medicina 58, no. 8: 1027. https://doi.org/10.3390/medicina58081027