
In Vitro Toxicological Profile of Labetalol-Folic Acid/Folate Co-Administration in H9c2(2-1) and HepaRG Cells

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Cell Culture
2.3. Cellular Viability
2.4. Cellular Morphology and Confluence
2.5. Wound Regeneration
2.6. Statistical Analysis
3. Results
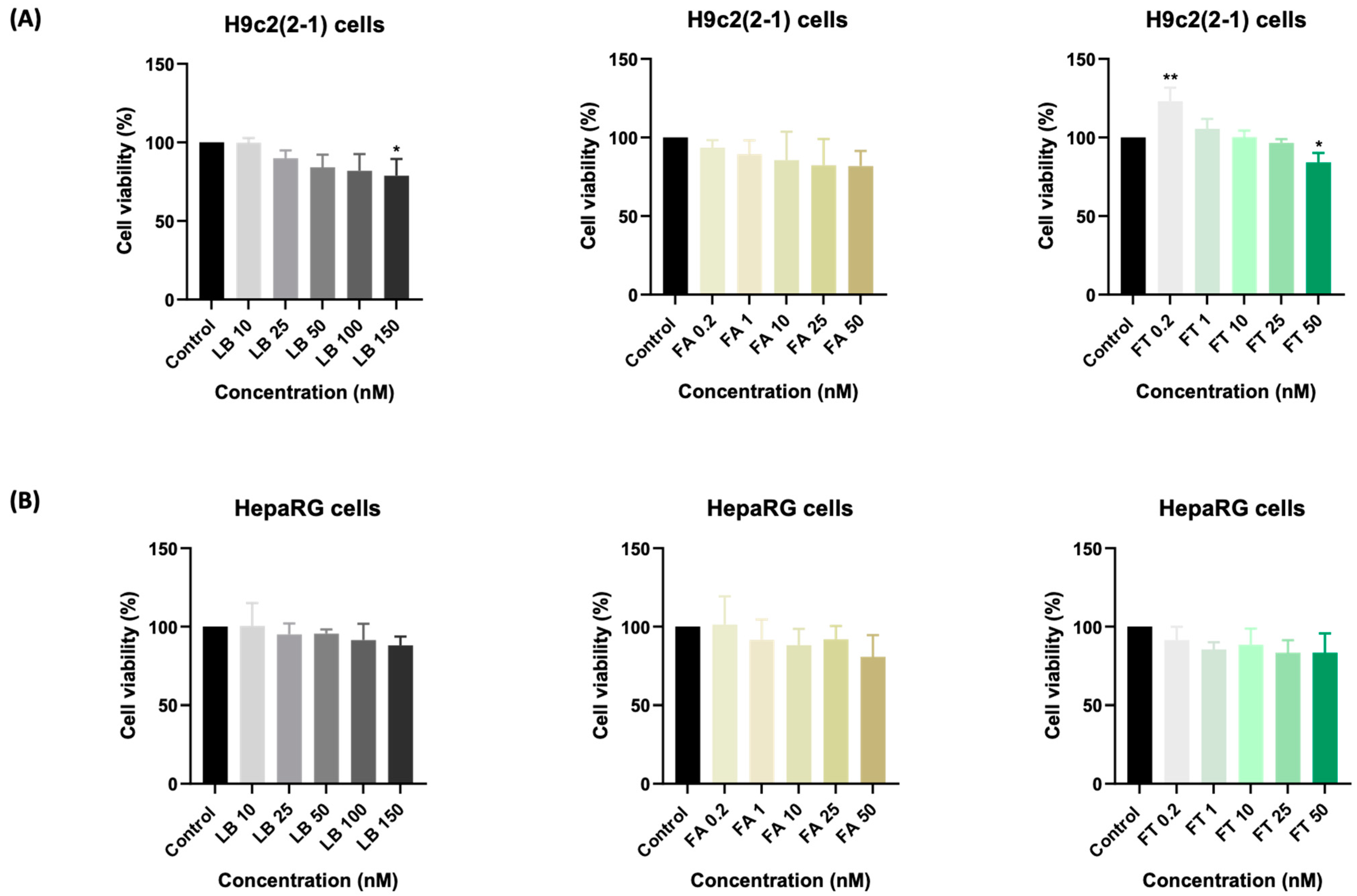
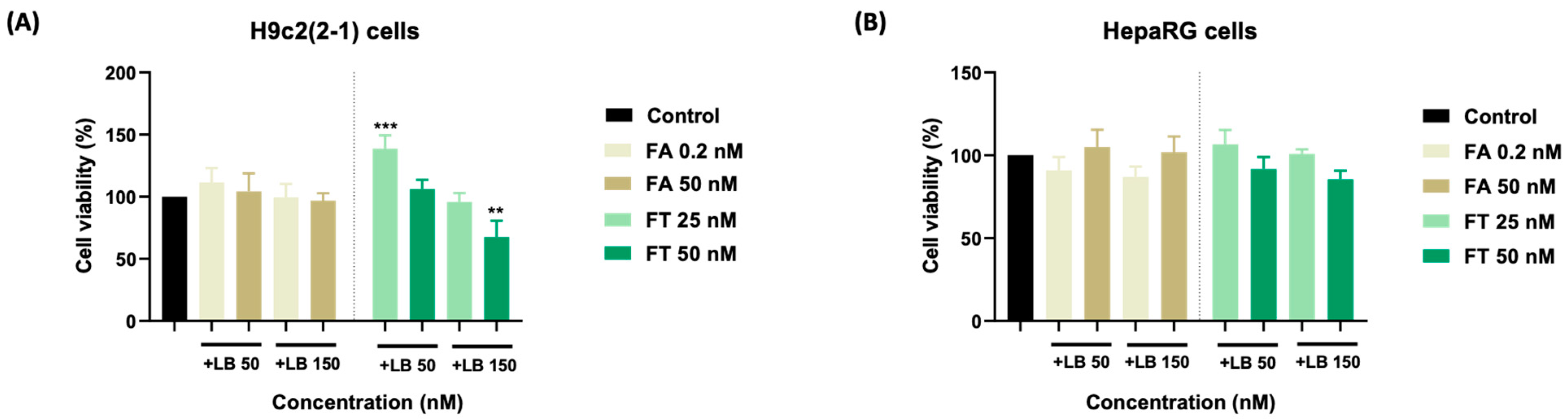
3.1. Cellular Viability
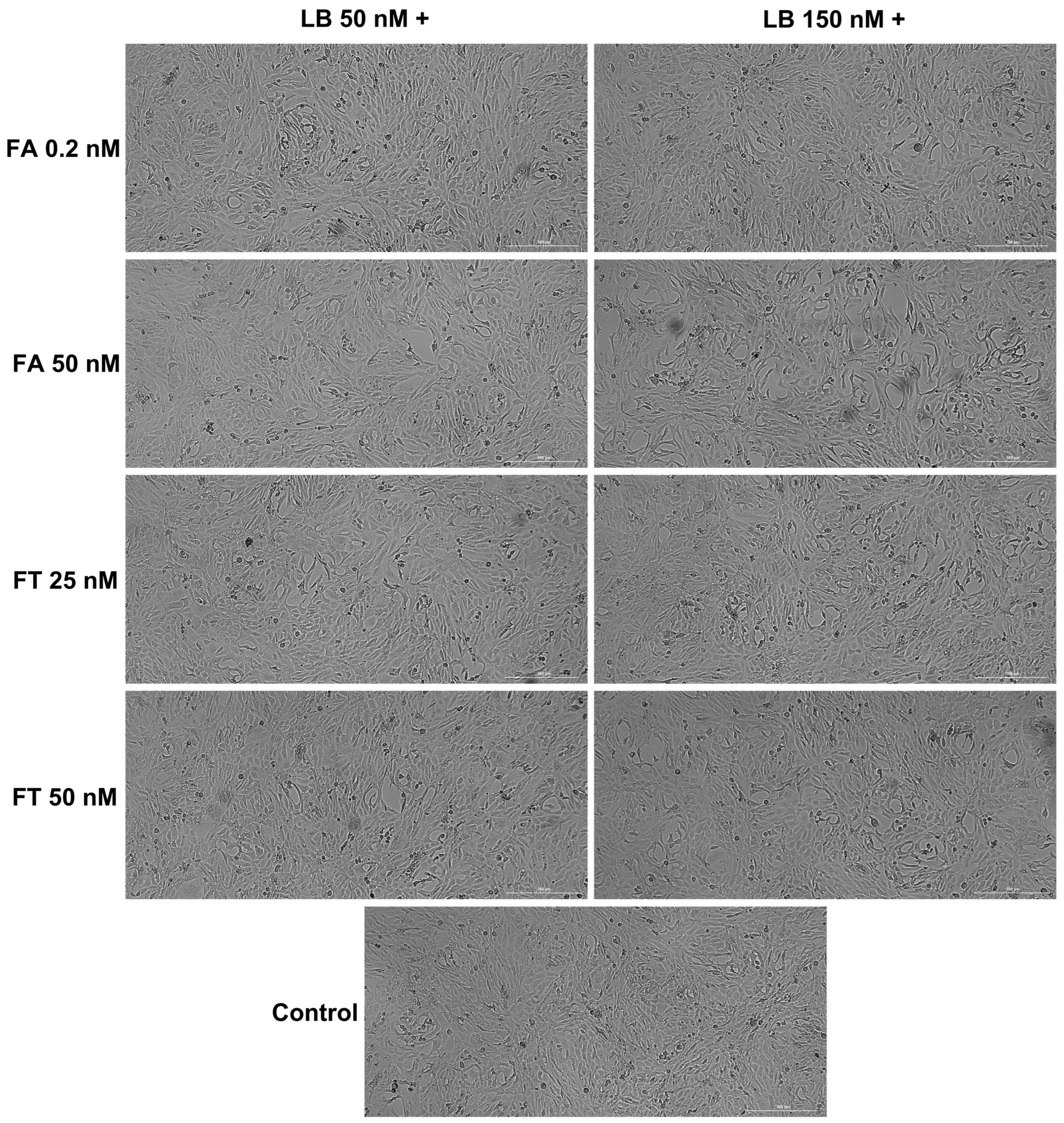
3.2. Cellular Morphology and Confluence
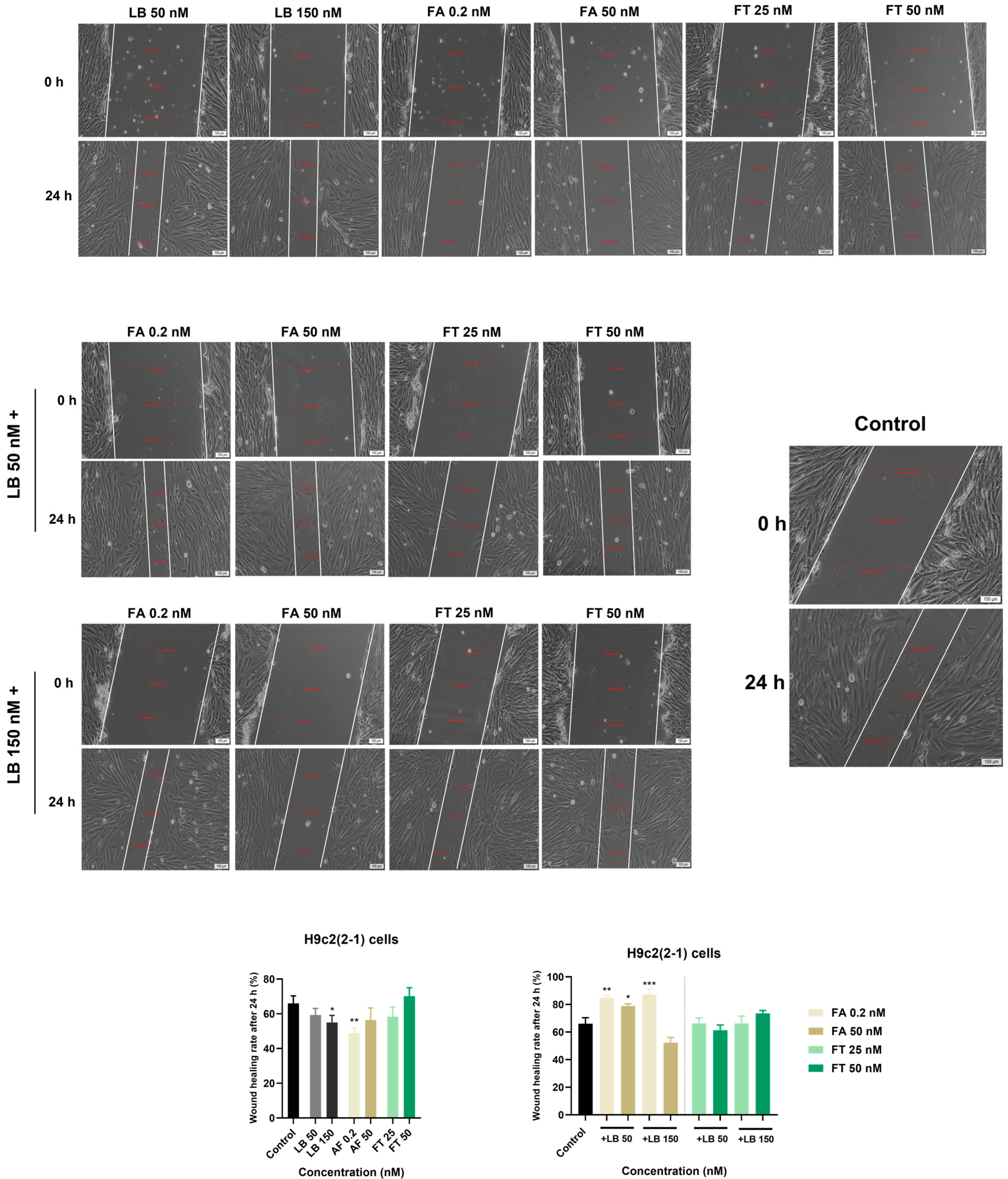
3.3. Wound Regeneration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xiang, C.; Luo, J.; Yang, G.; Sun, M.; Liu, H.; Yang, Q.; Ouyang, Y.; Xi, Y.; Yong, C.; Khan, M.J.; et al. Dietary Supplement Use during Pregnancy: Perceptions versus Reality. Int. J. Environ. Res. Public Health 2022, 19, 4063. [Google Scholar] [CrossRef] [PubMed]
- Ballestín, S.S.; Campos, M.I.G.; Ballestín, J.B.; Bartolomé, M.J.L. Is Supplementation with Micronutrients Still Necessary during Pregnancy? A Review. Nutrients 2021, 13, 3134. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.; Gahche, J.J.; Potischman, N.; Dwyer, J.T.; Guenther, P.M.; Sauder, K.A.; Bailey, R.L. Dietary Supplement Use and Its Micronutrient Contribution During Pregnancy and Lactation in the United States. Obstet. Gynecol. 2020, 135, 623–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbour, R.S.; Macleod, M.; Mires, G.; Anderson, A.S. Uptake of folic acid supplements before and during pregnancy: Focus group analysis of women’s views and experiences. J. Hum. Nutr. Diet. 2012, 25, 140–147. [Google Scholar] [CrossRef]
- Field, M.S.; Stover, P.J. Safety of folic acid. Ann. N. Y. Acad. Sci. 2018, 1414, 59–71. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, J.A.; Bell, S.J.; Guan, Y.; Yu, Y.H. Folic Acid supplementation and pregnancy: More than just neural tube defect prevention. Rev. Obstet. Gynecol. 2011, 4, 52–59. [Google Scholar]
- Shulpekova, Y.; Nechaev, V.; Kardasheva, S.; Sedova, A.; Kurbatova, A.; Bueverova, E.; Kopylov, A.; Malsagova, K.; Dlamini, J.C.; Ivashkin, V. The Concept of Folic Acid in Health and Disease. Molecules 2021, 26, 3731. [Google Scholar] [CrossRef]
- Duthie, S.J. Folate and cancer: How DNA damage, repair and methylation impact on colon carcinogenesis. J. Inherit. Metab. Dis. 2011, 34, 101–109. [Google Scholar] [CrossRef]
- Scaglione, F.; Panzavolta, G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica 2014, 44, 480–488. [Google Scholar] [CrossRef]
- Feghali, M.; Venkataramanan, R.; Caritis, S. Pharmacokinetics of drugs in pregnancy. Semin. Perinatol. 2015, 39, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Charlton, F.; Makris, A.; Hennessy, A. Antihypertensive drugs methyldopa, labetalol, hydralazine, and clonidine improve trophoblast interaction with endothelial cellular networks in vitro. J. Hypertens. 2014, 32, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xie, X.; Yuan, T.; Wang, Y.; Zhao, F.; Zhou, Z.; Zhang, H. Epidemiological trends of maternal hypertensive disorders of pregnancy at the global, regional, and national levels: A population-based study. BMC Pregnancy Childbirth 2021, 21, 364. [Google Scholar] [CrossRef] [PubMed]
- Kintiraki, E.; Papakatsika, S.; Kotronis, G.; Goulis, D.G.; Kotsis, V. Pregnancy-Induced hypertension. Hormones (Athens) 2015, 14, 211–223. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Xu, S.; Chen, X.; Zhang, X.; Li, X.; Lin, L.; Gao, D.; Wu, M.; Yang, S.; Cao, X.; et al. Folic Acid Supplement Use and Increased Risk of Gestational Hypertension. Hypertension 2020, 76, 150–156. [Google Scholar] [CrossRef]
- Liu, C.; Liu, C.; Wang, Q.; Zhang, Z. Supplementation of folic acid in pregnancy and the risk of preeclampsia and gestational hypertension: A meta-analysis. Arch. Gynecol. Obstet. 2018, 298, 697–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kattah, A.G.; Garovic, V.D. The Management of Hypertension in Pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 229–239. [Google Scholar] [CrossRef] [Green Version]
- Khedagi, A.M.; Bello, N.A. Hypertensive Disorders of Pregnancy. Cardiol. Clin. 2021, 39, 77–90. [Google Scholar] [CrossRef]
- Brown, C.M.; Garovic, V.D. Drug treatment of hypertension in pregnancy. Drugs 2014, 74, 283–296. [Google Scholar] [CrossRef]
- Magee, L.A.; Namouz-Haddad, S.; Cao, V.; Koren, G.; von Dadelszen, P. Labetalol for hypertension in pregnancy. Expert Opin. Drug Saf. 2015, 14, 453–461. [Google Scholar] [CrossRef]
- El-Borm, H.T.; Gobara, M.S.; Badawy, G.M. Ginger extract attenuates labetalol induced apoptosis, DNA damage, histological and ultrastructural changes in the heart of rat fetuses. Saudi J. Biol. Sci. 2021, 28, 440–447. [Google Scholar] [CrossRef]
- Odigboegwu, O.; Pan, L.J.; Chatterjee, P. Use of Antihypertensive Drugs During Preeclampsia. Front. Cardiovasc. Med. 2018, 5, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelan, A.; Izewski, J.; Berkelhammer, C.; Walloch, J.; Kay, H.H. Labetalol-Induced Hepatotoxicity during Pregnancy: A Case Report. AJP Rep. 2020, 10, e210–e212. [Google Scholar] [CrossRef] [PubMed]
- Maghiari, A.L.; Coricovac, D.; Pinzaru, I.A.; Macașoi, I.G.; Marcovici, I.; Simu, S.; Navolan, D.; Dehelean, C. High Concentrations of Aspartame Induce Pro-Angiogenic Effects in Ovo and Cytotoxic Effects in HT-29 Human Colorectal Carcinoma Cells. Nutrients 2020, 12, 3600. [Google Scholar] [CrossRef] [PubMed]
- Kis, A.M.; Macasoi, I.; Paul, C.; Radulescu, M.; Buzatu, R.; Watz, C.G.; Cheveresan, A.; Berceanu, D.; Pinzaru, I.; Dinu, S.; et al. Methotrexate and Cetuximab-Biological Impact on Non-Tumorigenic Models: In Vitro and In Ovo Assessments. Medicina (Kaunas) 2022, 58, 167. [Google Scholar] [CrossRef]
- Clark, S.M.; Dunn, H.E.; Hankins, G.D. A review of oral labetalol and nifedipine in mild to moderate hypertension in pregnancy. Semin. Perinatol. 2015, 39, 548–555. [Google Scholar] [CrossRef]
- Witek, P.; Korga, A.; Burdan, F.; Ostrowska, M.; Nosowska, B.; Iwan, M.; Dudka, J. The effect of a number of H9C2 rat cardiomyocytes passage on repeatability of cytotoxicity study results. Cytotechnology 2016, 68, 2407–2415. [Google Scholar] [CrossRef] [Green Version]
- Zordoky, B.N.M.; EL-Kadi, A.O.S. H9c2 cell line is a valuable in vitro model to study the drug metabolizing enzymes in the heart. J. Pharmacol. Toxicol. Methods 2007, 56, 317–322. [Google Scholar] [CrossRef]
- Hu, L.; Wu, F.; He, J.; Zhong, L.; Song, Y.; Shao, H. Cytotoxicity of safrole in HepaRG cells: Studies on the role of CYP1A2-mediated ortho-quinone metabolic activation. Xenobiotica 2019, 49, 1504–1515. [Google Scholar] [CrossRef]
- Blidisel, A.; Marcovici, I.; Coricovac, D.; Hut, F.; Dehelean, C.A.; Cretu, O.M. Experimental models of hepatocellular carcinoma—A preclinical perspective. Cancers 2021, 13, 3651. [Google Scholar] [CrossRef]
- Han, W.; Wu, Q.; Zhang, X.; Duan, Z. Innovation for hepatotoxicity in vitro research models: A review. J. Appl. Toxicol. 2019, 39, 146–162. [Google Scholar] [CrossRef] [Green Version]
- Ayad, M.; Costantine, M.M. Epidemiology of medications use in pregnancy. Semin. Perinatol. 2015, 39, 508–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uematsu, K.; Kobayashi, E.; Katsumoto, E.; Sugimoto, M.; Kawakami, T.; Terajima, T.; Maezawa, K.; Kizu, J. Umbilical cord blood concentrations of labetalol hydrochloride administered to patients with pregnancy induced hypertension, and subsequent neonatal findings. Hypertens. Res. Pregnancy 2013, 1, 88–92. [Google Scholar] [CrossRef] [Green Version]
- Obeid, R.; Kasoha, M.; Kirsch, S.H.; Munz, W.; Herrmann, W. Concentrations of unmetabolized folic acid and primary folate forms in pregnant women at delivery and in umbilical cord blood. Am. J. Clin. Nutr. 2010, 92, 1416–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeid, R.; Holzgreve, W.; Pietrzik, K. Folate supplementation for prevention of congenital heart defects and low birth weight: An update. Cardiovasc. Diagn. Ther. 2019, 9 (Suppl. 2), S424–S433. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Wang, S.; Chen, R.; Tong, X.; Wu, Z.; Mo, X. Maternal folic acid supplementation and the risk of congenital heart defects in offspring: A meta-analysis of epidemiological observational studies. Sci. Rep. 2015, 5, 8506. [Google Scholar] [CrossRef] [Green Version]
- Garbern, J.C.; Lee, R.T. Mitochondria and metabolic transitions in car-diomyocytes: Lessons from development for stem cell-derived cardiomyocytes. Stem Cell Res. Ther. 2021, 12, 177. [Google Scholar] [CrossRef]
- Xu, X.; Wei, W.; Jiang, W.; Song, Q.; Chen, Y.; Li, Y.; Zhao, Y.; Sun, H.; Yang, X. Association of folate intake with cardiovascular-disease mortality and all-cause mortality among people at high risk of cardiovascular-disease. Clin. Nutr. 2022, 41, 246–254. [Google Scholar] [CrossRef]
- Ahmad, S.; Panda, B.P.; Kohli, K.; Fahim, M.; Dubey, K. Folic acid ameliorates celecoxib car-diotoxicity in a doxorubicin heart failure rat model. Pharm. Biol. 2017, 55, 1295–1303. [Google Scholar] [CrossRef] [Green Version]
- Octavia, Y.; Kararigas, G.; de Boer, M.; Chrifi, I.; Kietadisorn, R.; Swinnen, M.; Duimel, H.; Verheyen, F.K.; Brandt, M.M.; Fliegner, D.; et al. Folic acid reduces doxorubicin-induced cardiomyopathy by modulating endothelial nitric oxide synthase. J. Cell. Mol. Med. 2017, 21, 3277–3287. [Google Scholar] [CrossRef] [Green Version]
- Cuesta, A.M.; Albiñana, V.; Gallardo-Vara, E.; Recio-Poveda, L.; de Rojas, P.I.; de Las Heras, K.V.G.; Aguirre, D.T.; Botella, L.M. The β2-adrenergic receptor antagonist ICI-118,551 blocks the constitutively activated HIF signalling in hemangioblastomas from von Hippel-Lindau disease. Sci. Rep. 2019, 9, 10062. [Google Scholar] [CrossRef]
- Pakdemirli, A.; Toksöz, F.; Karadağ, A.; Mısırlıoğlu, H.K.; Başpınar, Y.; Ellidokuz, H.; Açıkgöz, O. Role of mesenchymal stem cell-derived soluble factors and folic acid in wound healing. Turk. J. Med. Sci. 2019, 49, 914–921. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rednic, R.; Marcovici, I.; Dragoi, R.; Pinzaru, I.; Dehelean, C.A.; Tomescu, M.; Arnautu, D.A.; Craina, M.; Gluhovschi, A.; Valcovici, M.; et al. In Vitro Toxicological Profile of Labetalol-Folic Acid/Folate Co-Administration in H9c2(2-1) and HepaRG Cells. Medicina 2022, 58, 784. https://doi.org/10.3390/medicina58060784
Rednic R, Marcovici I, Dragoi R, Pinzaru I, Dehelean CA, Tomescu M, Arnautu DA, Craina M, Gluhovschi A, Valcovici M, et al. In Vitro Toxicological Profile of Labetalol-Folic Acid/Folate Co-Administration in H9c2(2-1) and HepaRG Cells. Medicina. 2022; 58(6):784. https://doi.org/10.3390/medicina58060784
Chicago/Turabian StyleRednic, Robert, Iasmina Marcovici, Razvan Dragoi, Iulia Pinzaru, Cristina Adriana Dehelean, Mirela Tomescu, Diana Aurora Arnautu, Marius Craina, Adrian Gluhovschi, Mihaela Valcovici, and et al. 2022. "In Vitro Toxicological Profile of Labetalol-Folic Acid/Folate Co-Administration in H9c2(2-1) and HepaRG Cells" Medicina 58, no. 6: 784. https://doi.org/10.3390/medicina58060784