Pattern of Antibiotic Use in the Perinatal Period in a Public University Hospital in Romania

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Vidal, A.C.; Murphy, S.K.; Murtha, A.P.; Schildkraut, J.M.; Soubry, A.; Huang, Z.; Neelon, S.E.B.; Fuemmeler, B.; Iversen, E.; Wang, F.; et al. Associations between antibiotic exposure during pregnancy, birth weight, and aberrant methylation at imprinted genes among offspring. Int. J. Obes. 2013, 37, 907–913. [Google Scholar] [CrossRef] [Green Version]
- Andrikopoulou, M.; Huang, Y.; Duffy, C.R.; Stern-Ascher, C.N.; Wright, J.D.; Goffman, D.; D’Alton, M.E.; Friedman, A.M. Antibiotic Use Without Indication During Delivery Hospitalizations in the United States. Obstet. Gynecol. 2019, 134, 718–725. [Google Scholar] [CrossRef]
- Lee, A.C.; Mullany, L.C.; Koffi, A.K.; Rafiqullah, I.; Khanam, R.; Folger, L.V.; Rahman, M.; Mitra, D.K.; Labrique, A.; Christian, P.; et al. Urinary tract infections in pregnancy in a rural population of Bangladesh: Population-based prevalence, risk factors, etiology, and antibiotic resistance. BMC Pregnancy Childbirth 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micle, O.; Antal, L.; Naghi, P.; Țica, O.; Zaha, D.C.; Zdrînca, M.M.; Dobjanchi, L.; Sabău, M.; Mureșan, M. The prevalence of urinary tract infections in pregnancy and implications on fetal development. Farmacia 2020, 68, 32. [Google Scholar] [CrossRef]
- Flenady, V.; Hawley, G.; Stock, O.M.; Kenyon, S.; Badawi, N. Prophylactic antibiotics for inhibiting preterm labour with intact membranes. Cochrane Database Syst. Rev. 2013, 12, CD000246. [Google Scholar] [CrossRef] [Green Version]
- Puopolo, K.M.; Lynfield, R.; Cummings, J.J.; American Academy of Pediatrics, Committee on Fetus and Newborn, Committee on Infectious Diseases. Management of Infants at Risk for Group B Streptococcal Disease. Pediatrics 2019, 144, e20191881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuperman, A.A.; Koren, O. Antibiotic use during pregnancy: How bad is it? BMC Med. 2016, 14, 91. [Google Scholar] [CrossRef] [Green Version]
- Bookstaver, P.B.; Bland, C.M.; Griffin, B.; Stover, K.R.; Eiland, L.S.; McLaughlin, M. A Review of Antibiotic Use in Pregnancy. Pharmacotherapy 2015, 35, 1052–1062. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Factors Influencing the Intestinal Microbiome During the First Year of Life. Pediatr. Infect. Dis. J. 2018, 37, e315–e335. [Google Scholar] [CrossRef]
- Madan, J.C.; Salari, R.C.; Saxena, D.; Davidson, L.; O’Toole, G.A.; Moore, J.H.; Sogin, M.L.; Foster, J.A.; Edwards, W.H.; Palumbo, P.; et al. Gut microbial colonisation in premature neonates predicts neonatal sepsis. Arch. Dis. Child. Fetal Neonatal. Ed. 2012, 97, F456–F462. [Google Scholar] [CrossRef] [PubMed]
- Knip, M.; Siljander, H. The role of the intestinal microbiota in type 1 diabetes mellitus. Nat. Rev. Endocrinol. 2016, 12, 154–167. [Google Scholar] [CrossRef]
- Zimmermann, P.; Messina, N.; Mohn, W.W.; Finlay, B.B.; Curtis, N. Association between the intestinal microbiota and allergic sensitization, eczema, and asthma: A systematic review. J. Allergy Clin. Immunol. 2019, 143, 467–485. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Curtis, N. Effect of intrapartum antibiotics on the intestinal microbiota of infants: A systematic review. Arch. Dis. Child. Fetal Neonatal. Ed. 2020, 105, 201–208. [Google Scholar] [CrossRef]
- Crider, K.S.; Cleves, M.A.; Reefhuis, J.; Berry, R.J.; Hobbs, C.A.; Hu, D.J. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch. Pediatr. Adolesc. Med. 2009, 163, 978–985. [Google Scholar] [CrossRef] [Green Version]
- Adam, M.P.; Polifka, J.E.; Friedman, J.M. Evolving knowledge of the teratogenicity of medications in human pregnancy. Am. J. Med. Genet. C Semin. Med. Genet. 2011, 157, 175–182. [Google Scholar] [CrossRef]
- Meek, C. The Food and Drug Administration’s Pregnancy and Lactation Labeling Rule; Embryo Project Encyclopedia: Tempe, AZ, USA, 2014; ISSN 1940-5030. Available online: http://embryo.asu.edu/handle/10776/13100 (accessed on 3 March 2022).
- Zaha, D.C.; Bungau, S.; Uivarosan, D.; Tit, D.M.; Maghiar, T.A.; Maghiar, O.; Pantis, C.; Fratila, O.; Rus, M.; Vesa, C.M. Antibiotic consumption and microbiological epidemiology in surgery departments: Results from a single study center. Antibiotics 2020, 9, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index. 2022. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 8 March 2022).
- Food and Drug Administration. Content and format of labeling for human prescription drug and biological products: Requirements for pregnancy and lactation labeling. Fed. Regist. 2014, 79, 72064–72103. [Google Scholar]
- Thinkhamrop, J.; Hofmeyr, G.J.; Adetoro, O.; Lumbiganon, P.; Ota, E. Antibiotic prophylaxis during the second and third trimester to reduce adverse pregnancy outcomes and morbidity. Cochrane Database Syst. Rev. 2015, 1, CD002250. [Google Scholar] [CrossRef] [PubMed]
- Czeizel, A.E.; Rockenbauer, M.; Sørensen, H.T.; Olsen, J. Use of cephalosporins during pregnancy and in the presence of congenital abnormalities: A population-based, case-control study. Am. J. Obstet. Gynecol. 2001, 184, 1289–1296. [Google Scholar] [CrossRef]
- Anitha, B.; Malavika, S.; Kumar, B.; Ramesh, Y. Current trends in drugs avoided in pregnancy. J. Drug Deliv. Ther. 2018, 8, 342–350. [Google Scholar] [CrossRef]
- Sule-Odu, A.O.; Akadri, A.A.; Oluwole, A.A.; Osinupebi, O.A.; Andu, B.A.; Akiseku, A.K.; Lawal, A.I. Vaginal Candida infection in pregnancy and its implications for fetal well-being. Afr. J. Reprod. Health 2020, 24, 33–40. [Google Scholar] [CrossRef]
- Roberts, C.L.; Algert, C.S.; Rickard, K.L.; Morris, J.M. Treatment of vaginal candidiasis for the prevention of preterm birth: A systematic review and meta-analysis. Syst. Rev. 2015, 4, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brocklehurst, P.; Gordon, A.; Heatley, E.; Milan, S.J. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst. Rev. 2013, 1, CD000262. [Google Scholar] [CrossRef] [Green Version]
- Klebanoff, M.A.; Carey, J.C.; Hauth, J.C.; Hillier, S.L.; Nugent, R.P.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Wapner, R.J.; Trout, W.; et al. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. N. Engl. J. Med. 2001, 345, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Kazy, Z.; Puho, E.; Czeizel, A.E. Teratogenic potential of vaginal metronidazole treatment during pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 2, 174–178. [Google Scholar] [CrossRef]
- Yefet, E.; Schwartz, N.; Chazan, B.; Salim, R.; Romano, S.; Nachum, Z. The safety of quinolones and fluoroquinolones in pregnancy: A meta-analysis. BJOG 2018, 125, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Acar, S.; Keskin-Arslan, E.; Erol-Coskun, H.; Kaya-Temiz, T.; Kaplan, Y.C. Pregnancy outcomes following quinolone and fluoroquinolone exposure during pregnancy: A systematic review and meta-analysis. Reprod. Toxicol. 2019, 85, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Bahat Dinur, A.; Koren, G.; Matok, I.; Wiznitzer, A.; Gorodischer, R.U.E.; Levy, A. Fetal safety of macrolides. Antimicrob. Agents Chemother. 2013, 57, 3307–3311. [Google Scholar] [CrossRef] [Green Version]
- Fan, H.; Gilbert, R.; O’Callaghan, F.; Li, L. Associations between macrolide antibiotics prescribing during pregnancy and adverse child outcomes in the UK: Population based cohort study. BMJ 2020, 368, m331. [Google Scholar] [CrossRef] [Green Version]
- Sarah Jestin Kilpatrick. American Academy of Pediatrics; American College of Obstetricians and Gynecologists: Washington, DC, USA, 2017. [Google Scholar]
- Mazor-Dray, E.; Levy, A.; Schlaeffer, F.; Sheiner, E. Maternal urinary tract infection: Is it independently associated with adverse pregnancy outcome? J. Maternal. Fetal Neonatal. Med. 2009, 22, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M. Clinical practice. Uncomplicated urinary tract infection. N. Engl. J. Med. 2012, 366, 1028–1037. [Google Scholar] [CrossRef]
- Habak, P.J.; Griggs, R.P., Jr. Urinary Tract Infection In Pregnancy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Smaill, F.M.; Vazquez, J.C. Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane Database Syst. Rev. 2015, 8. [Google Scholar] [CrossRef]
- van de Mheen, L.; Smits, S.M.; Terpstra, W.E.; Leyte, A.; Bekedam, D.J.; van den Akker, E.S. Haemolytic anaemia after nitrofurantoin treatment in a pregnant woman with G6PD deficiency. BMJ Case Rep. 2014, 2014, bcr2013010087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daina, L.G.; Sabău, M.; Daina, C.M.; Neamțu, C.; Tit, D.M.; Buhaș, C.L.; Bungau, C.; Aleya, L.; Bungau, S. Improving performance of a pharmacy in a Romanian hospital through implementation of an internal management control system. Sci. Total Environ. 2019, 675, 51–61. [Google Scholar] [CrossRef]
- Daina, L.; Carp, G.; Neamțu, C.; Venter, A.; Armean, P. Antibiotherapy in hospital—Between the efficiency and quality of medical services. The role of the drug committee. Farmacia 2015, 63, 3. [Google Scholar]
- Zaha, D.C.; Bungau, S.; Aleya, S.; Tit, D.M.; Vesa, C.M.; Popa, A.R.; Pantis, C.; Maghiar, O.A.; Bratu, O.G.; Furau, C.; et al. What antibiotics for what pathogens? The sensitivity spectrum of isolated strains in an intensive care unit. Sci. Total Environ. 2019, 687, 118–127. [Google Scholar] [CrossRef]
- Fowler, J.R.; Simon, L.V. Chorioamnionitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Park, J.Y.; Park, C.W.; Moon, K.C.; Park, J.S.; Jun, J.K.; Lee, S.J.; Kim, J.H. Retinopathy of prematurity in infants without fetal growth restriction is decreased with the progression of acute histologic chorioamnionitis: New observation as a protective factor against retinopathy of prematurity. Placenta 2021, 104, 161–167. [Google Scholar] [CrossRef]
- Maki, Y.; Fujisaki, M.; Sato, Y.; Sameshima, H. Candida Chorioamnionitis Leads to Preterm Birth and Adverse Fetal-Neonatal Outcome. Infect. Dis. Obstet. Gynecol. 2017, 2017, 9060138. [Google Scholar] [CrossRef] [Green Version]
- Malloy, M.H. Chorioamnionitis: Epidemiology of newborn management and outcome United States 2008. J. Perinatol. 2014, 34, 611–655. [Google Scholar] [CrossRef] [PubMed]
- Committee Opinion No. 712: Intrapartum Management of Intraamniotic Infection. Obstet. Gynecol. 2017, 130, e95–e101.
- Woodd, S.L.; Montoya, A.; Barreix, M.; Pi, L.; Calvert, C.; Rehman, A.M.; Chou, D.; Campbell, O.M.R. Incidence of maternal peripartum infection: A systematic review and meta-analysis. PLOS Med. 2019, 16, e1002984. [Google Scholar] [CrossRef] [PubMed]
- Vică, M.L.; Glevitzky, M.; Tit, D.M.; Behl, T.; Heghedűş-Mîndru, R.C.; Ursu, F.; Popa, M.; Glevitzky, I.; Bungău, S. The antimicrobial activity of honey and propolis extracts from the central region of Romania. Food Biosci. 2021, 41, 101014. [Google Scholar] [CrossRef]


{kind=link}
| Category | Evidence | Classes or Antibiotics |
|---|---|---|
| A | There is no evidence of risk to the fetus in the first and later trimesters. | |
| B | In case of animals and pregnant women there is no evidence to demonstrate risk to the fetus. | Penicillin and beta-lactam inhibitors, carbapenems (except imipenem/cilastatin), glycopeptides, imidazole, lincosamides, macrolides, third-generation cephalosporins |
| C | Although there is evidence of detrimental effects on the fetus in animals and no adequate and well-controlled studies in humans, potential advantages may justify the drug’s usage in pregnant women despite potential dangers. | Fluoroquinolones, polymixyns, rifamycins, trimethoprim-sulfamethoxazole, gentamycin |
| D | Based on adverse reaction data from investigational or marketing experience or human trials, there is positive evidence of human fetal risk, although possible benefits may justify use of the medicine in pregnant women despite potential hazards. | Aminoglycosides—except gentamycin Tetracyclines |
| X | There has been evidence of fetal abnormalities in animals or humans, and/or there is positive evidence of human fetal risk based on adverse reaction data from experimental or marketing experience, and the dangers of using the medicine in pregnant women clearly outweigh the possible benefits. |
| ATC | Antibiotic | DDD/100 Bed Days | |||||
|---|---|---|---|---|---|---|---|
| 2017 | 2018 | 2019 | 2020 | 2021 | p-Value | ||
| J01GB06 | Amikacin | 0.61 | 0.37 | 0.13 | 0.10 | 8.55 | 1 |
| J01GB03 | Gentamicin | 7.41 | 2.56 | 1.80 | 2.21 | 24.74 | 0.73 |
| J01CA04 | Amoxicillin | 24.71 | 33.04 | 15.88 | 31.48 | 145.88 | 0.73 |
| J01CA01 | Ampicillin | 28.77 | 15.17 | 4.06 | 7.83 | 62.78 | 0.73 |
| J01CR02 | Amoxicillin/clavulanate | 15.36 | 1.55 | 1.15 | 0.84 | 5.87 | 1 |
| J01DH02 | Meropenem | 0.55 | 1.00 | 0.44 | 0.83 | 6.34 | 0.33 |
| J01DH51 | Imipenem/cilastatin | - | - | - | 0.01 | 0.13 | 0.14 |
| J01DC04 | Cefaclor | 19.72 | 18.51 | 4.32 | 2.95 | 0.00 | 0.08 |
| J01DC02 | Cefuroxime | 40.42 | 47.28 | 27.49 | 21.41 | 1.97 | 0.08 |
| J01DD04 | Ceftriaxone | 129.72 | 117.06 | 113.90 | 127.98 | 346.86 | 0.30 |
| J01DD12 | Cefoperazone | 0.01 | - | 0.001 | - | 0.00 | - |
| J01DD02 | Ceftazidime | 0.53 | 0.24 | 0.10 | 0.33 | 0.11 | 0.53 |
| J01DD08 | Cefixime | 33.06 | 16.93 | 12.63 | 22.69 | 401.63 | 0.30 |
| J01DD62 | Cefoperazone/ sulbactam | 0.02 | 0.01 | 0.008 | - | 0.12 | 1 |
| J01XD01 | Metronidazol | 13.58 | 12.34 | 15.80 | 9.39 | 176.21 | 0.73 |
| J01MA02 | Ciprofloxacin | 2.89 | 1.17 | 0.49 | 2.36 | 108.69 | 0.33 |
| J01MA01 | Ofloxacin | 0.80 | 0.33 | 0.32 | 1.16 | 3.54 | 0.30 |
| J01MA14 | Moxifloxacin | 0.03 | - | 0.032 | - | 0.00 | 1 |
| J01CF04 | Oxacillin | 0.88 | 0.34 | 0.04 | 0.03 | 0.23 | 0.73 |
| J01FF01 | Clindamycin | 6.45 | 2.97 | 2.27 | 1.66 | 12.04 | 1 |
| J01FA09 | Clarithromycin | 1.02 | 1.16 | 2.45 | 1.02 | 2.00 | 1 |
| J01FA10 | Azithromycin | 0.33 | 0.18 | 0.006 | 0.078 | 0.79 | 0.73 |
| J01FA01 | Erythromycin | - | - | 0.35 | 1.058 | 2.66 | 0.08 |
| J01CE01 | Benzyl penicillin | 0.14 | 0.08 | 0.104 | 0.069 | 0.04 | 0.30 |
| J01XA01 | Vancomycin | 0.03 | 0.10 | 0.12 | 0.040 | 0.58 | 0.73 |
| J01XB01 | Colistin | 0.11 | 0.039 | - | - | - | 0.37 |
| Total | 327.30 | 272.54 | 204.05 | 235.61 | 1311.77 | ||
| Antibiotics by Class | 2017 | 2018 | 2019 | 2020 | 2021 | Total | p-Value |
|---|---|---|---|---|---|---|---|
| Cephalosporins (third generation) | 163.37 | 134.26 | 126.65 | 151.01 | 748.73 | 1324.02 | 1 |
| Aminopenicillins | 68.85 | 49.77 | 21.10 | 40.17 | 214.53 | 394.41 | 0.73 |
| Imidazoles | 13.59 | 12.34 | 15.80 | 9.39 | 176.21 | 227.33 | 0.72 |
| Cephalosporins (second generation) | 60.15 | 65.80 | 31.82 | 24.37 | 1.97 | 184.12 | 0.08 |
| Fluoroquinolones | 3.74 | 1.51 | 0.86 | 3.53 | 112.22 | 121.86 | 0.30 |
| Aminoglycosides | 8.03 | 2.94 | 1.95 | 2.32 | 33.29 | 48.53 | 0.73 |
| Lincosamide | 6.45 | 2.97 | 2.27 | 1.67 | 12.04 | 25.40 | 1 |
| Macrolides | 1.36 | 1.35 | 2.82 | 2.17 | 5.46 | 13.16 | 0.30 |
| Carbapenems | 0.56 | 1.01 | 0.45 | 0.84 | 6.47 | 9.33 | 0.73 |
| Izoxazolilpenicillins (oxacillin) | 0.89 | 0.35 | 0.05 | 0.03 | 0.23 | 1.55 | 0.73 |
| Glycopeptides | 0.03 | 0.11 | 0.12 | 0.04 | 0.58 | 0.88 | 0.73 |
| Natural penicillins | 0.14 | 0.08 | 0.10 | 0.07 | 0.04 | 0.44 | 0.30 |
| Polypeptides | 0.11 | 0.04 | - | - | - | 0.15 | 0.37 |
| Rifampicins | 0.03 | 0.00 | 0.06 | - | - | 0.09 | 1 |
| Category of Antibiotics | 2017 | 2018 | 2019 | 2020 | 2021 | Total | p-Value |
|---|---|---|---|---|---|---|---|
| B | 313.48 (95.77) | 266.53 (97.79) | 198.69 (97.37) | 228.69 (97.06) | 1163.88 (88.82) | 2171.27 (92.34) | 0.73 |
| C | 4.88 (1.49) | 2.71 (0.99) | 3.31 (1.62) | 4.57 (1.93) | 139.09 (10.60) | 168.57 (7.16) | 0.30 |
| D | 0.61 (0.18) | 0.37 (0.13) | 0.13 (0.06) | 0.10 (0.04) | 8.55 (0.65) | 9.79 (0.41) | 1 |
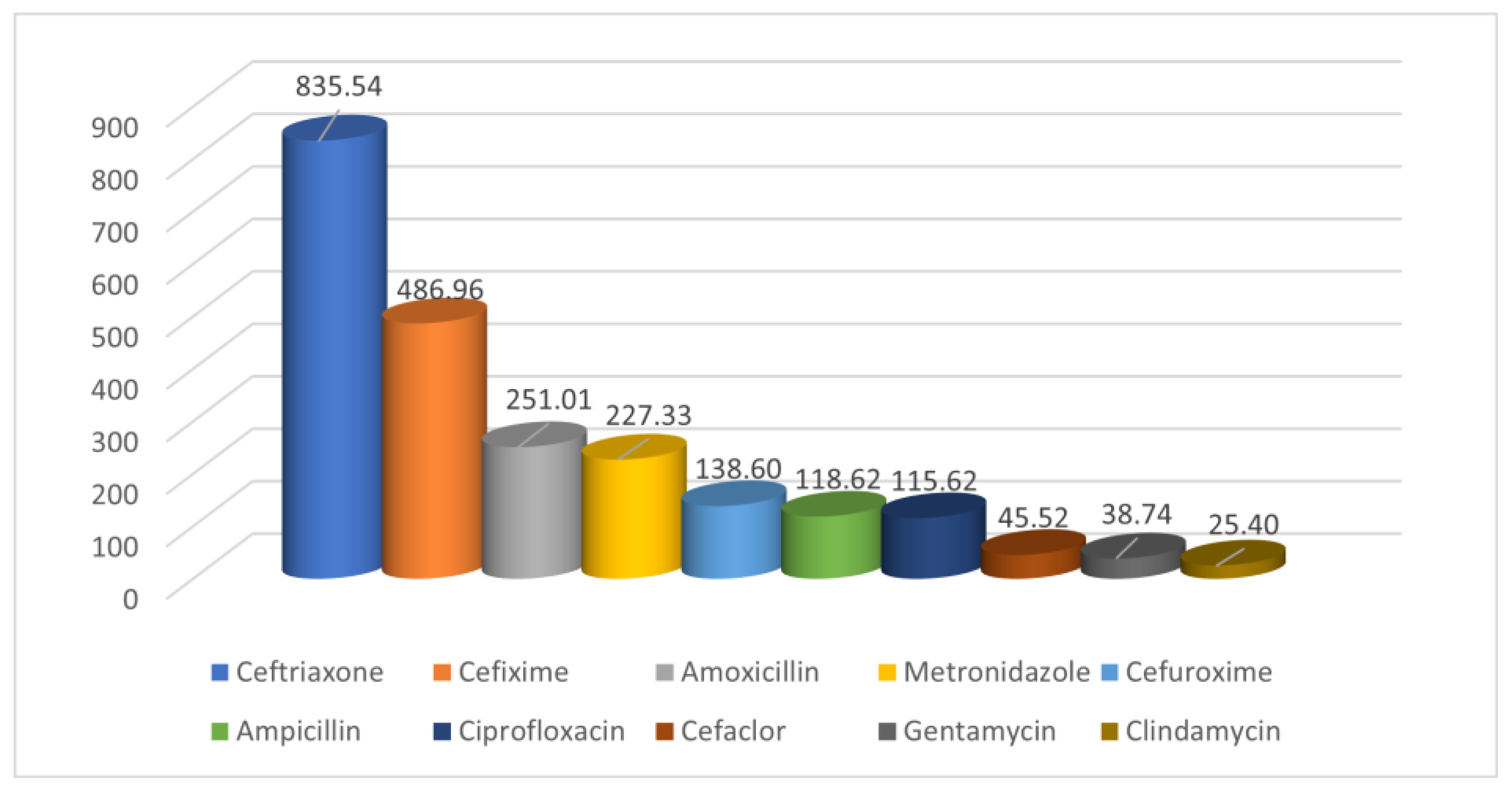
| ATC | Antibiotic | 2017 | 2018 | 2019 | 2020 | 2021 | Total |
|---|---|---|---|---|---|---|---|
| J01DD04 | Ceftriaxone | 129.73 | 117.06 | 113.90 | 127.98 | 346.86 | 835.54 |
| J01DD08 | Cefixime | 33.07 | 16.94 | 12.63 | 22.69 | 401.63 | 486.96 |
| J01CA04 | Amoxicillin | 24.72 | 33.04 | 15.88 | 31.49 | 145.88 | 251.01 |
| J01XD01 | Metronidazole | 13.59 | 12.34 | 15.80 | 9.39 | 176.21 | 227.33 |
| J01DC02 | Cefuroxime | 40.42 | 47.29 | 27,50 | 21.42 | 1.97 | 138.60 |
| J01CA01 | Ampicillin | 28.77 | 15.17 | 4,06 | 7.84 | 62.78 | 118.62 |
| J01DC04 | Cefaclor | 19.73 | 18.52 | 4.32 | 2.95 | - | 45.52 |
| J01FF01 | Clindamycin | 6.45 | 2.97 | 2.27 | 1.67 | 12.04 | 25.40 |
| J01CR02 | Amoxicillin/ clavulanate | 15.36 | 1.55 | 1.16 | 0.85 | 5.87 | 24.78 |
| J01DH02 | Meropenem | 0.56 | 1.01 | 0.45 | 0.83 | 6.34 | 9.18 |
| J01FA01 | Erythromycin | - | - | 0.36 | 1.06 | 2.66 | 4.07 |
| J01FA10 | Azithromycin | 0.34 | 0.19 | 0.01 | 0.08 | 0.79 | 1.41 |
| J01DD02 | Ceftazidime | 0.54 | 0.25 | 0.11 | 0.34 | 0.11 | 1.35 |
| J01XA01 | Vancomycin | 0.03 | 0.11 | 0.12 | 0,04 | 0.58 | 0.88 |
| J01CE01 | Benzyl penicillin | 0.14 | 0,08 | 0.10 | 0,07 | 0.04 | 0.44 |
| J01DD62 | Cefoperazone/ sulbactam | 0.03 | 0.01 | 0.01 | 0.00 | 0.12 | 0.17 |
| J01DD12 | Cefoperazone | 0.01 | - | - | - | - | 0.01 |
| ATC | Antibiotic | 2017 | 2018 | 2019 | 2020 | 2021 | Total |
|---|---|---|---|---|---|---|---|
| J01GB03 | Gentamycin | 7.41 | 2.56 | 1.81 | 2.22 | 24.74 | 38.74 |
| J01DH51 | Imipenem/ cilastatin | - | - | - | 0.01 | 0.13 | 0.14 |
| J01MA02 | Ciprofloxacin | 2.90 | 1.17 | 0.50 | 2.37 | 108.69 | 115.62 |
| J01MA01 | Ofloxacin | 0.81 | 0.34 | 0.32 | 1.17 | 3.54 | 6.17 |
| J01MA14 | Moxifloxacin | 0.04 | - | 0.03 | - | - | 0.07 |
| J01FA09 | Clarithromycin | 1.02 | 1.16 | 2.46 | 1.03 | 2.00 | 7.68 |
| J01XB01 | Colistin | 0.11 | 0.04 | - | - | - | 0.15 |
| Diagnostic | 2017 | 2018 | 2019 | 2020 | 2021 | Total | p-Value |
|---|---|---|---|---|---|---|---|
| Number (%) | |||||||
| Renal and urinary tract infections | 813 (22.38) | 1050 (29.47) | 604 (18.78) | 241 (7.27) | 470 (13.72) | 3178 (18.53) | 0.30 |
| Chorioamnionitis | 69 (1.89) | 48 (1.34) | 74 (2.30) | 69 (2.08) | 87 (2.54) | 347 (2.02) | 0.30 |
| Surgical wound infections of obstetric origin | 0 (0) | 4 (0.11) | 4 (0.12) | 7 (0.21) | 36 (1.05) | 51 (0.29) | 0.14 |
| Other genito-urinary tract infections after birth | 76 (2.09) | 97 (2.72) | 128 (3.98) | 111 (3.35) | 78 (2.27) | 490 (2.85) | 0.73 |
| Mastitis | 2 (0.05) | 4 (0.11) | 1 (0.03) | 10 (0.30) | 7 (0.20) | 24 (0.13) | 0.73 |
| Total number of births | 3632 | 3562 | 3216 | 3311 | 3425 | 17,146 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hodoșan, V.; Daina, C.M.; Zaha, D.C.; Cotrău, P.; Vladu, A.; Pantiș, C.; Dorobanțu, F.R.; Negrău, M.; Maghiar, A.; Daina, L.G. Pattern of Antibiotic Use in the Perinatal Period in a Public University Hospital in Romania. Medicina 2022, 58, 772. https://doi.org/10.3390/medicina58060772
Hodoșan V, Daina CM, Zaha DC, Cotrău P, Vladu A, Pantiș C, Dorobanțu FR, Negrău M, Maghiar A, Daina LG. Pattern of Antibiotic Use in the Perinatal Period in a Public University Hospital in Romania. Medicina. 2022; 58(6):772. https://doi.org/10.3390/medicina58060772
Chicago/Turabian StyleHodoșan, Viviana, Cristian Marius Daina, Dana Carmen Zaha, Petru Cotrău, Adriana Vladu, Carmen Pantiș, Florica Ramona Dorobanțu, Marcel Negrău, Adriana Maghiar, and Lucia Georgeta Daina. 2022. "Pattern of Antibiotic Use in the Perinatal Period in a Public University Hospital in Romania" Medicina 58, no. 6: 772. https://doi.org/10.3390/medicina58060772