
Effects of H-Reflex Onset Latency on Gait in Elderly and Hemiplegic Individuals


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Sampling
2.2. Inclusion and Exclusion Criteria
2.3. Measurements
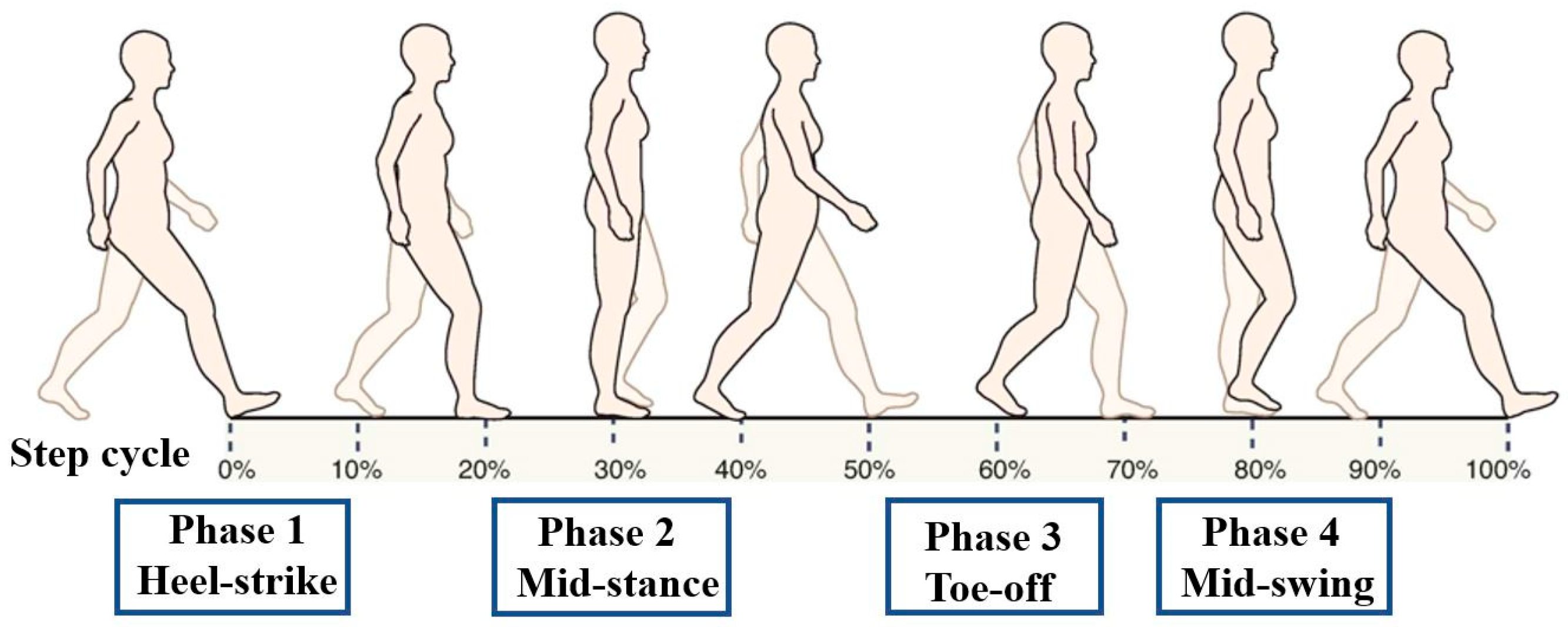
- Heel strike (HS): The moment of initial contact of the heel with the ground;
- Mid-stance (MS): The phase in which the grounded leg supports the full body weight;
- Toe off (TO): The phase in which the toe lifts off the ground;
- Mid-swing (SW): The phase in which the raised leg passes the grounded leg.
2.4. Data Analysis
3. Results
3.1. General Characteristics of Subjects
3.2. The H-Reflex Latencies during Walking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Provident, I. A Review of: “Occupational therapy for physical dysfunction 6th edition (2008)”. Occup. Ther. Health Care 2009, 23, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Demura, S. The relationship between the stipulated tempo step test, daily activity ability and gait time in elderly. Arch. Gerontol. Geriatr. 2010, 51, 333–337. [Google Scholar] [CrossRef]
- Riemann, B.L.; Myers, J.B.; Lephart, S.M. Sensorimotor system measurement techniques. J. Athl. Train. 2002, 37, 85–98. [Google Scholar] [PubMed]
- Cote, K.P.; Brunet, M.E.; Gansneder, B.M.; Shultz, S.J. Effects of pronated and supinated foot postures on static and dynamic postural stability. J. Athl. Train. 2005, 40, 41–46. [Google Scholar] [PubMed]
- Cruz, T.H.; Lewek, M.D.; Dhaher, Y.Y. Biomechanical impairments and gait adaptations post-stroke: Multi-factorial associations. J. Biomech. 2009, 42, 1673–1677. [Google Scholar] [CrossRef] [Green Version]
- Roerdink, M.; Lamoth, C.J.; Kwakkel, G.; van Wieringen, P.C.; Beek, P.J. Gait coordination after stroke: Benefits of acoustically paced treadmill walking. Phys. Ther. 2007, 87, 1009–1022. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, E.B.; Dyhre-Poulsen, P.; Alkjaer, T.; Aagaard, P.; Magnusson, S.P. Interindividual differences in H reflex modulation during normal walking. Exp. Brain Res. 2002, 142, 108–115. [Google Scholar] [CrossRef]
- Dobkin, B.H.; Firestine, A.; West, M.; Saremi, K.; Woods, R. Ankle dorsiflexion as an fMRI paradigm to assay motor control for walking during rehabilitation. Neuroimage 2004, 23, 370–381. [Google Scholar] [CrossRef] [Green Version]
- Sacco, K.; Cauda, F.; D’Agata, F.; Mate, D.; Duca, S.; Geminiani, G. Reorganization and enhanced functional connectivity of motor areas in repetitive ankle movements after training in locomotor attention. Brain Res. 2009, 1297, 124–134. [Google Scholar] [CrossRef]
- Gajos, A.; Kujawski, S.; Gajos, M.; Chatys, Ż.; Bogacki, P. Applications of the H-reflex in kinesiology: A systematic review. Biomed. Hum. Kinet. 2014, 6, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Piirainen, J.M.; Avela, J.; Sippola, N.; Linnamo, V. Age dependency of neuromuscular function and dynamic balance control. Eur. J. Sport Sci. 2010, 10, 69–79. [Google Scholar] [CrossRef]
- Palmieri, R.M.; Ingersoll, C.D.; Hoffman, M.A. The hoffmann reflex: Methodologic considerations and applications for use in sports medicine and athletic training research. J. Athl. Train. 2004, 39, 268–277. [Google Scholar] [PubMed]
- Hoffman, M.A.; Koceja, D.M. The effects of vision and task complexity on Hoffmann reflex gain. Brain Res. 1995, 700, 303–307. [Google Scholar] [CrossRef]
- Pinar, S.; Kitano, K.; Koceja, D.M. Role of vision and task complexity on soleus H-reflex gain. J. Electromyogr. Kinesiol. 2010, 20, 354–358. [Google Scholar] [CrossRef]
- Christie, A.; Lester, S.; LaPierre, D.; Gabriel, D.A. Reliability of a new measure of H-reflex excitability. Clin. Neurophysiol. 2004, 115, 116–123. [Google Scholar] [CrossRef]
- Belda-Lois, J.M.; Mena-del Horno, S.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos, A.; et al. Rehabilitation of gait after stroke: A review towards a top-down approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.S.; Zhou, S. Soleus H-reflex and its relation to static postural control. Gait Posture 2011, 33, 169–178. [Google Scholar] [CrossRef]
- Brinkworth, R.S.; Tuncer, M.; Tucker, K.J.; Jaberzadeh, S.; Turker, K.S. Standardization of H-reflex analyses. J. Neurosci. Methods 2007, 162, 1–7. [Google Scholar] [CrossRef]
- Zehr, E.P. Considerations for use of the Hoffmann reflex in exercise studies. Eur. J. Appl. Physiol. 2002, 86, 455–468. [Google Scholar] [CrossRef]
- Taube, W.; Leukel, C.; Gollhofer, A. Influence of enhanced visual feedback on postural control and spinal reflex modulation during stance. Exp. Brain Res. 2008, 188, 353–361. [Google Scholar] [CrossRef]
- Azma, K.; Raeissadat, S.A.; Hosseini, A.; Mahmoudi, H.; Sepehrian, M.; Salehi, Z. Thenar muscles H reflex in patients with fibromyalgia: A case control study. Acta Reumatol. Port. 2016, 41, 145–150. [Google Scholar] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, G.R.; Knutzen, K.M. Soleus Hoffmann-reflex modulation during walking in healthy elderly and young adults. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, B570–B579. [Google Scholar] [CrossRef] [Green Version]
- Bulbulian, R.; Darabos, B.L. Motor neuron excitability: The Hoffmann reflex following exercise of low and high intensity. Med. Sci. Sports Exerc. 1986, 18, 697–702. [Google Scholar] [CrossRef]
- Eke-Okoro, S.T. The H-reflex studied in the presence of alcohol, aspirin, caffeine, force and fatigue. Electromyogr. Clin. Neurophysiol. 1982, 22, 579–589. [Google Scholar] [PubMed]
- Hausdorff, J.M.; Ladin, Z.; Wei, J.Y. Footswitch system for measurement of the temporal parameters of gait. J. Biomech. 1995, 28, 347–351. [Google Scholar] [CrossRef]
- Kamibayashi, K.; Nakajima, T.; Fujita, M.; Takahashi, M.; Ogawa, T.; Akai, M.; Nakazawa, K. Effect of sensory inputs on the soleus H-reflex amplitude during robotic passive stepping in humans. Exp. Brain Res. 2010, 202, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Pensini, M.; Martin, A. Effect of voluntary contraction intensity on the H-reflex and V-wave responses. Neurosci. Lett. 2004, 367, 369–374. [Google Scholar] [CrossRef]
- Neddermeyer, T.J.; Fluhr, K.; Lotsch, J. Principle components analysis of pain thresholds to thermal, electrical, and mechanical stimuli suggests a predominant common source of variance. Pain 2008, 138, 286–291. [Google Scholar] [CrossRef]
- Byrne, C.A.; O’Keeffe, D.T.; Donnelly, A.E.; Lyons, G.M. Effect of walking speed changes on tibialis anterior EMG during healthy gait for FES envelope design in drop foot correction. J. Electromyogr. Kinesiol. 2007, 17, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Pizzi, A.; Carlucci, G.; Falsini, C.; Verdesca, S.; Grippo, A. Evaluation of upper-limb spasticity after stroke: A clinical and neurophysiologic study. Arch. Phys. Med. Rehabil. 2005, 86, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Eng, J.J.; Tang, P.-F. Gait training strategies to optimize walking ability in people with stroke: A synthesis of the evidence. Expert Rev. Neurother. 2007, 7, 1417–1436. [Google Scholar] [CrossRef] [Green Version]
- Jaberzadeh, S.; Scutter, S.; Warden-Flood, A.; Nazeran, H. Between-days reliability of H-reflexes in human flexor carpi radialis. Arch. Phys. Med. Rehabil. 2004, 85, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Hoch, M.C.; Staton, G.S.; Medina McKeon, J.M.; Mattacola, C.G.; McKeon, P.O. Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. J. Sci. Med. Sport 2012, 15, 574–579. [Google Scholar] [CrossRef]
- Krause, B.; Hopkins, J.; Ingersoll, C.; Cordova, M.; Edwards, J. The relationship of ankle cooling and rewarming to the human soleus H reflex. J. Sport Rehabil. 2000, 9, 1–10. [Google Scholar] [CrossRef]
- Matsugi, A.; Mori, N.; Uehara, S.; Kamata, N.; Oku, K.; Mukai, K.; Nagano, K. Task dependency of the long-latency facilitatory effect on the soleus H-reflex by cerebellar transcranial magnetic stimulation. Neuroreport 2014, 25, 1375–1380. [Google Scholar] [CrossRef]
- Knikou, M.; Rymer, W.Z. Static and dynamic changes in body orientation modulate spinal reflex excitability in humans. Exp. Brain Res. 2003, 152, 466–475. [Google Scholar] [CrossRef]
- Taube, W.; Gruber, M.; Gollhofer, A. Spinal and supraspinal adaptations associated with balance training and their functional relevance. Acta Physiol. 2008, 193, 101–116. [Google Scholar] [CrossRef]
- Okuma, Y.; Mizuno, Y.; Lee, R.G. Reciprocal Ia inhibition in patients with asymmetric spinal spasticity. Clin. Neurophysiol. 2002, 113, 292–297. [Google Scholar] [CrossRef]
- Carr, J.; Shepherd, R. Stroke Rehabilitation: Guidelines for Exercise and Training to Optimize Motor Skill; Butterworth-Heinemann: Edinburgh, UK, 2004. [Google Scholar]
- Orendurff, M.S.; Segal, A.D.; Aiona, M.D.; Dorociak, R.D. Triceps surae force, length and velocity during walking. Gait Posture 2005, 21, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.; Burnfield, J.M. Gait Analysis. Normal and Pathological Function, 2nd ed.; Slack: Thorofare, NJ, USA, 2010. [Google Scholar]
- Burridge, J.H.; Taylor, P.N.; Hagan, S.A.; Wood, D.E.; Swain, I.D. The effects of common peroneal stimulation on the effort and speed of walking: A randomized controlled trial with chronic hemiplegic patients. Clin. Rehabil. 1997, 11, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grindstaff, T.L.; Beazell, J.R.; Sauer, L.D.; Magrum, E.M.; Ingersoll, C.D.; Hertel, J. Immediate effects of a tibiofibular joint manipulation on lower extremity H-reflex measurements in individuals with chronic ankle instability. J. Electromyogr. Kinesiol. 2011, 21, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Manella, K.J.; Field-Fote, E.C. Modulatory effects of locomotor training on extensor spasticity in individuals with motor-incomplete spinal cord injury. Restor. Neurol. Neurosci. 2013, 31, 633–646. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Normal (n = 25) | Stroke (n = 25) | t | p Value |
|---|---|---|---|---|
| Age (years) | 65.52 ± 10.63 | 67.56 ± 11.25 | −0.659 | 0.513 |
| Height (cm) | 165.44 ± 9.36 | 167.84 ± 9.56 | −0.897 | 0.374 |
| Weight (kg) | 65.84 ± 11.02 | 72.72 ± 9.86 | −2.327 | 0.024 * |
| Leg length (cm) | 80.64 ± 4.36 | 87.76 ± 5.21 | −5.243 | 0.000 * |
| Phase | Group | M ± SD | t | p Value |
|---|---|---|---|---|
| Heel-strike | Stroke | 29.24 ± 2.07 | −1.157 | 0.253 |
| Normal | 30.12 ± 3.19 | |||
| Mid-stance | Stroke | 26.92 ± 2.33 | −4.793 | 0.000 * |
| Normal | 30.56 ± 3.00 | |||
| Toe-off | Stroke | 26.08 ± 2.70 | −5.515 | 0.000 * |
| Normal | 30.08 ± 2.41 | |||
| Mid-swing | Stroke | 27.72 ± 3.09 | −2.444 | 0.009 * |
| Normal | 29.96 ± 3.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-C.; Cho, S.-H. Effects of H-Reflex Onset Latency on Gait in Elderly and Hemiplegic Individuals. Medicina 2022, 58, 716. https://doi.org/10.3390/medicina58060716
Kim S-C, Cho S-H. Effects of H-Reflex Onset Latency on Gait in Elderly and Hemiplegic Individuals. Medicina. 2022; 58(6):716. https://doi.org/10.3390/medicina58060716
Chicago/Turabian StyleKim, Seon-Chil, and Sung-Hyoun Cho. 2022. "Effects of H-Reflex Onset Latency on Gait in Elderly and Hemiplegic Individuals" Medicina 58, no. 6: 716. https://doi.org/10.3390/medicina58060716