
MRI Findings of Muscle Damage after Total Hip Arthroplasty Using the Complete Muscle Preserving Anterolateral Supine Approach


Abstract
:1. Introduction
2. Materials and Methods
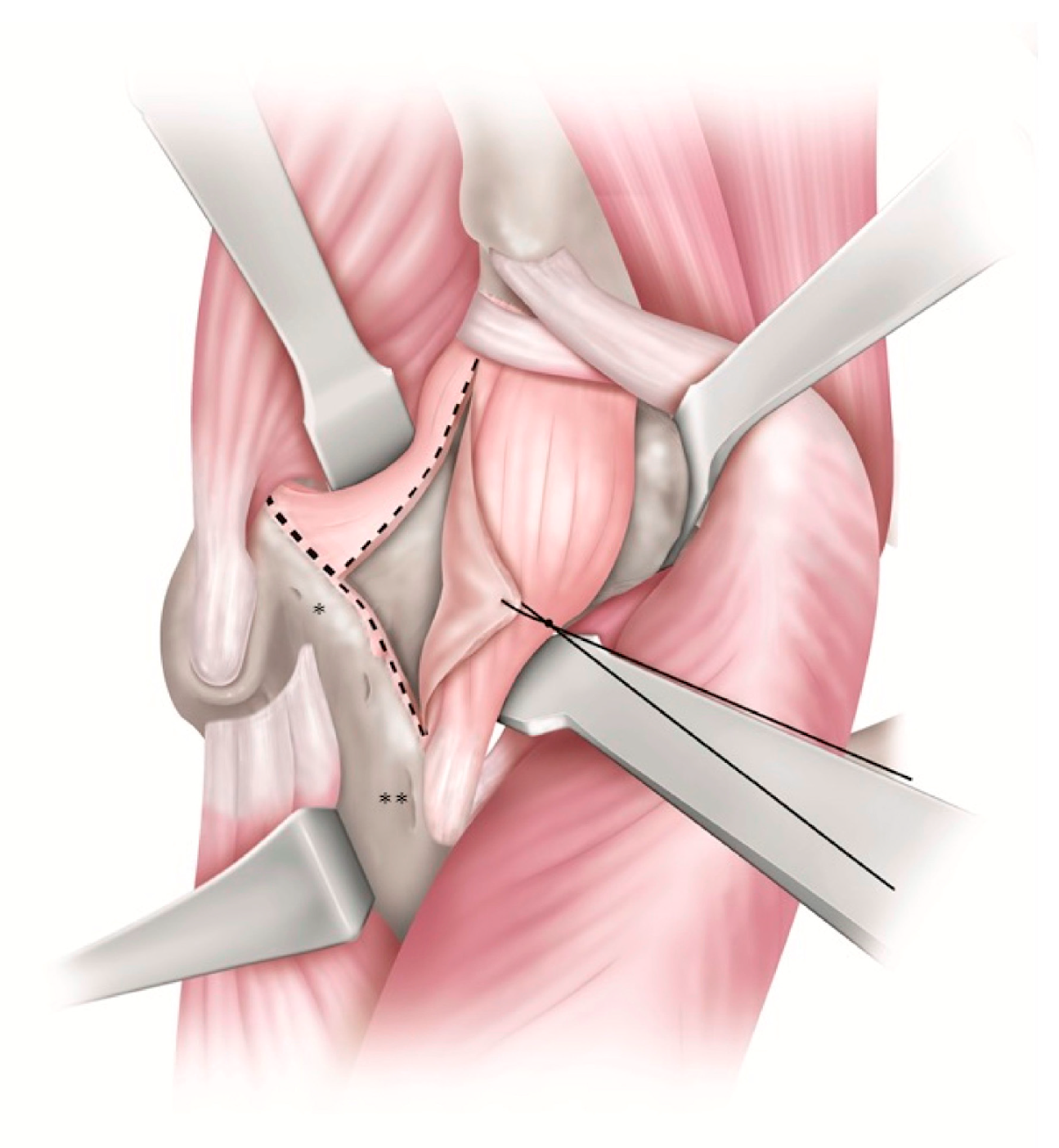
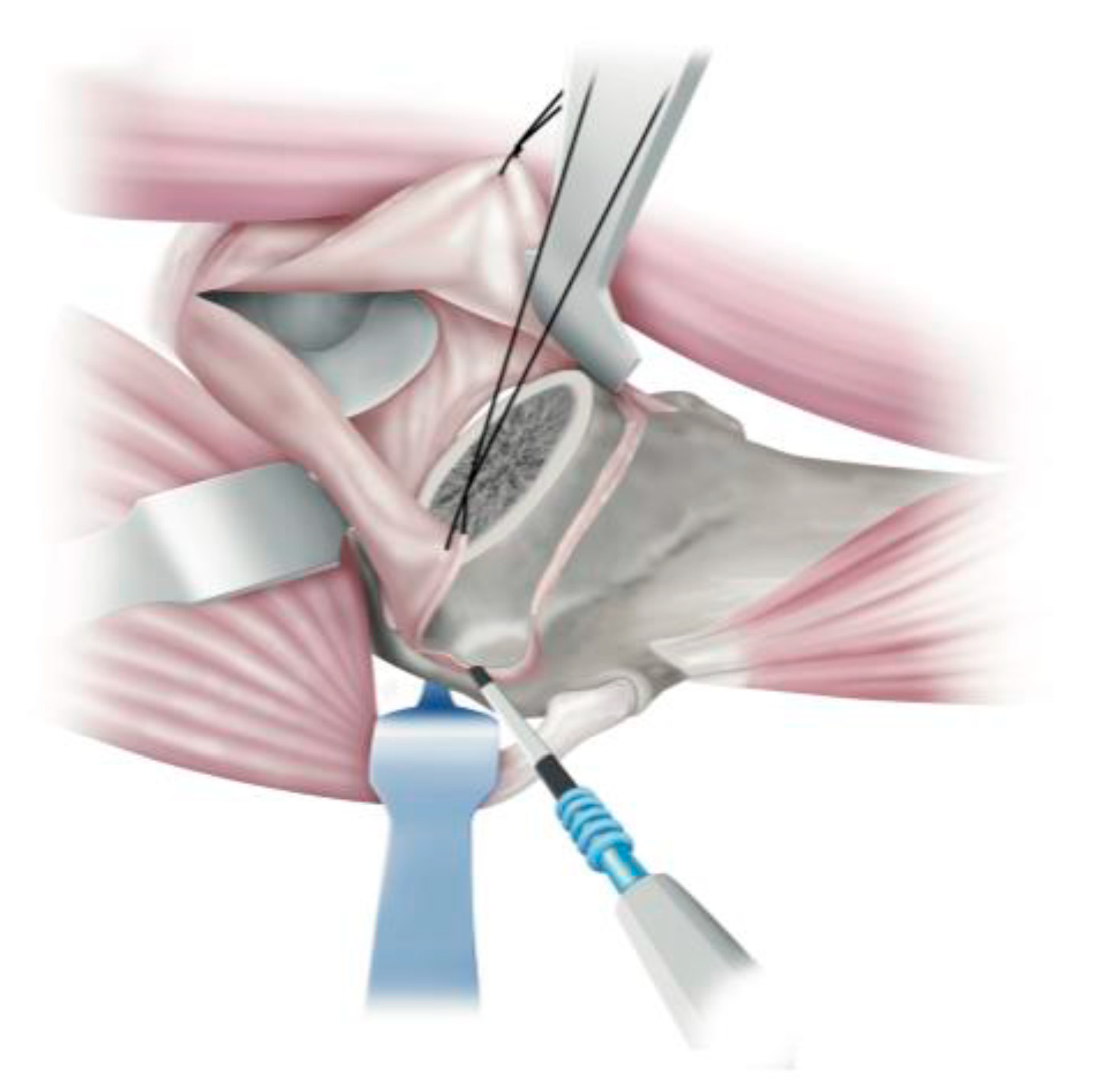
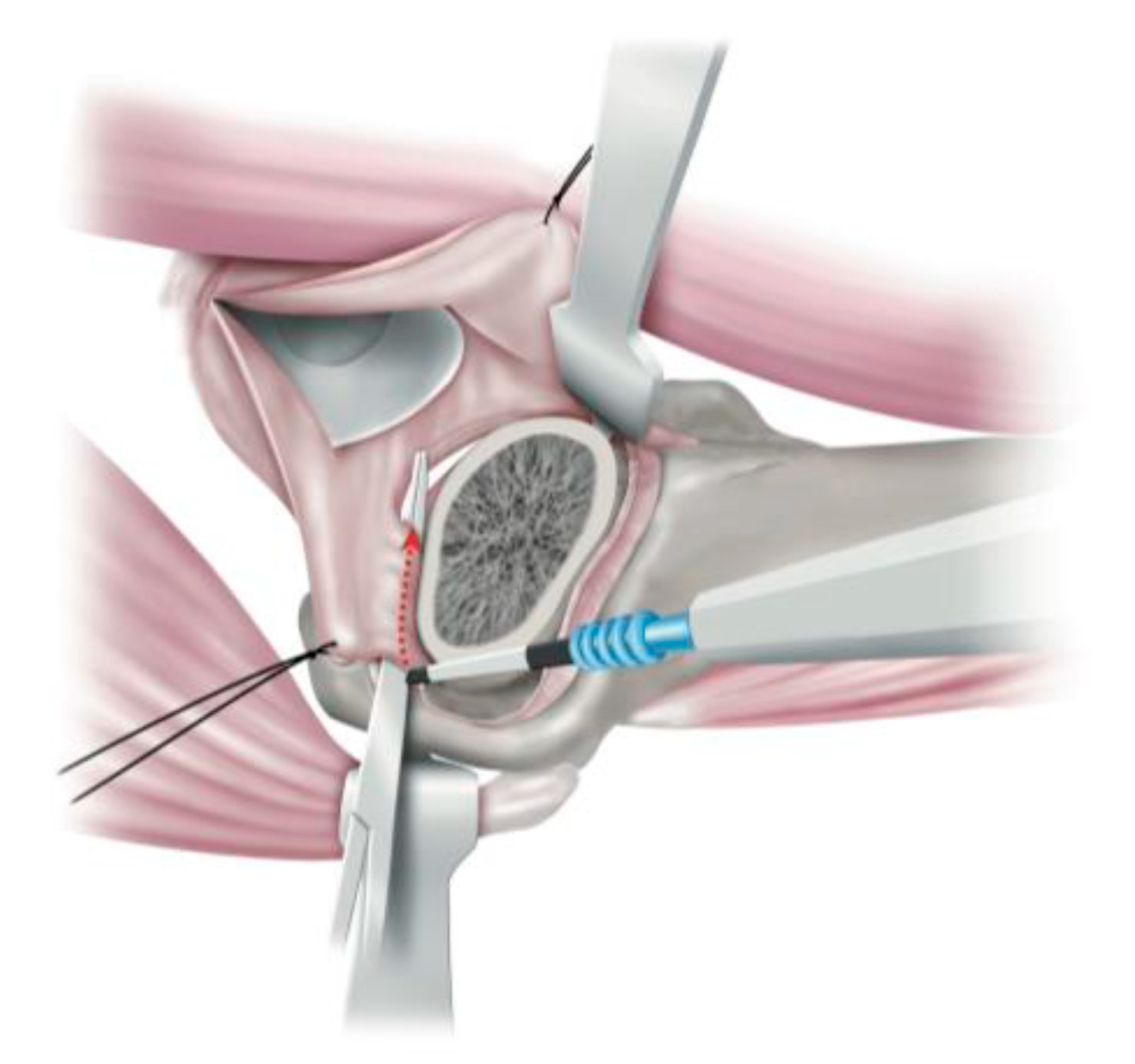
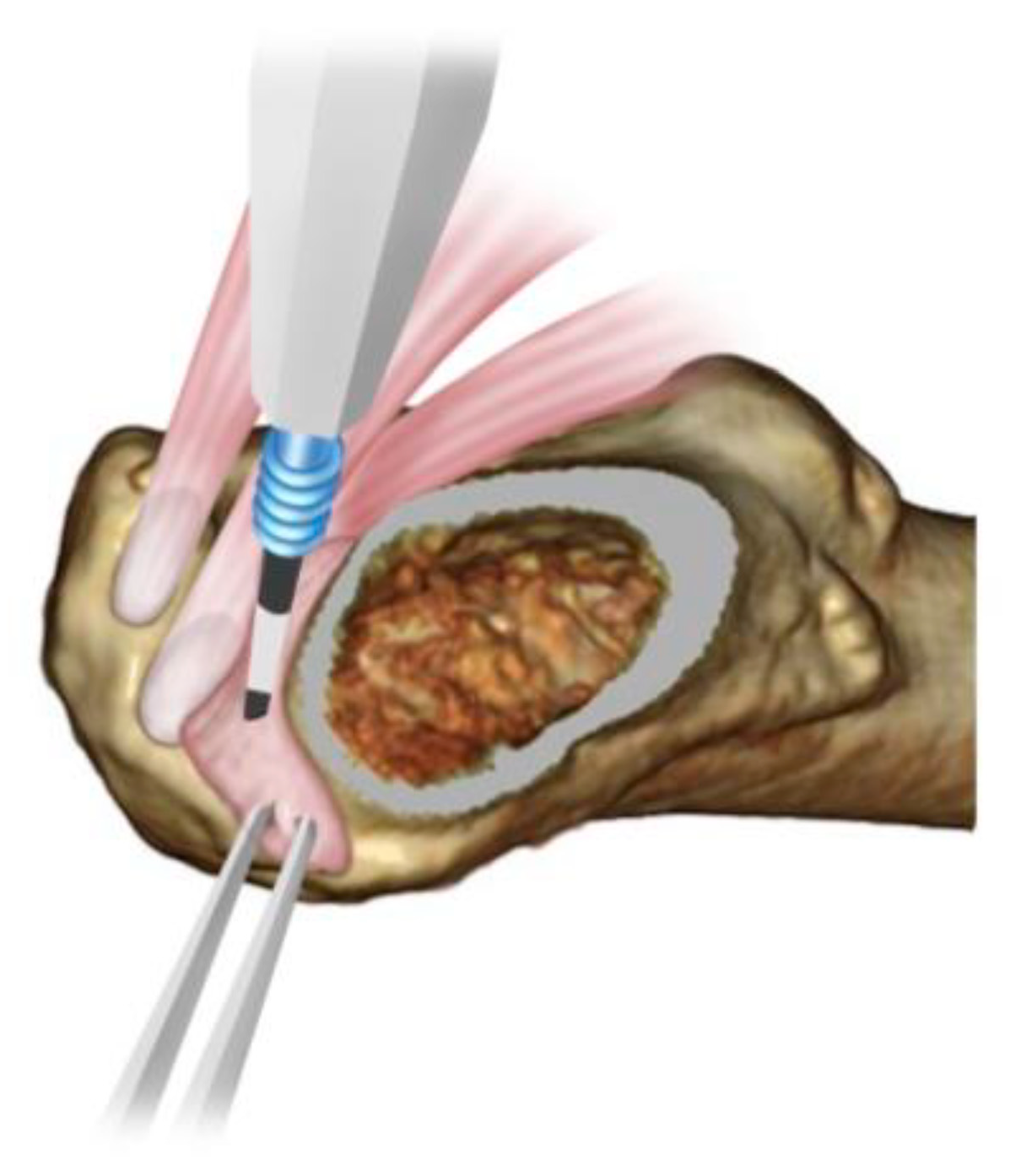
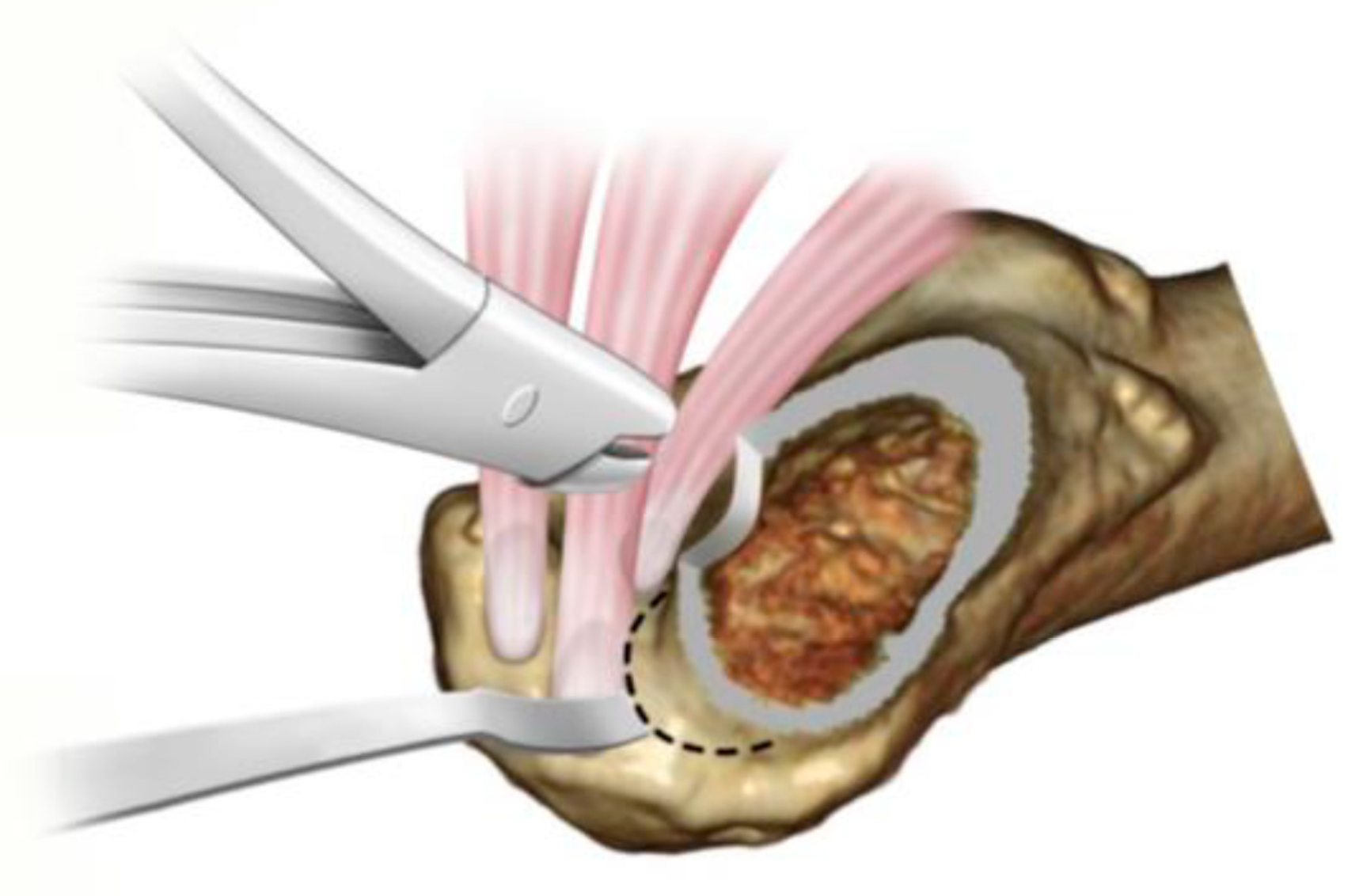
Surgical Technique of the Complete Muscle Preserving Procedure, ALS THA
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takada, R.; Jinno, T.; Miyatake, K.; Hirao, M.; Yoshii, T.; Okawa, A. Incidence of tensor fascia lata muscle atrophy after using the modified Watson-Jones anterolateral approach in total hip arthroplasty. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Tohtz, S.; Winkler, T.; Dewey, M.; Springer, I.; Perka, C. MRI findings of gluteus minimus muscle damage in primary total hip arthroplasty and the influence on clinical outcome. Arch. Orthop. Traumatol. Surg. 2010, 130, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Goutallier, D.; Postel, J.M.; Bernageau, J.; Lavau, L.; Voisin, M.C. Fatty Muscle Degeneration in Cuff Ruptures. Pre and postoperative Evaluation by CT Scan. Clin. Orthop. Relat. Res. 1994, 304, 78–83. [Google Scholar] [CrossRef]
- Stähelin, T.; Drittenbass, L.; Hersche, O.; Miehlke, W.; Munzinger, U. Failure of capsular enhanced short external rotator repair after total hip replacement. Clin. Orthop. Relat. Res. 2004, 420, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Pellicci, P.M.; Potter, H.G.; Foo, L.F.; Boettner, F. MRI shows Biologic restoration of posterior soft tissue repairs after THA. Clin. Orthop. Relat. Res. 2009, 467, 940–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agten, C.A.; Sutter, R.; Dora, C.; Pfirrmann, C.W.A. MR imaging of soft tissue alterations after total hip arthroplasty: Comparison of classic surgical approaches. Eur. Radiol. 2017, 27, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, M.; Hasegawa, Y.; Okura, T.; Ochiai, S.; Fujibayashi, T. Muscle damage after total hip arthroplasty through the direct anterior approach for developmental dysplasia of the hip. J. Arthroplast. 2017, 32, 2466–2473. [Google Scholar] [CrossRef] [PubMed]
- Kawarai, Y.; Iida, S.; Nakamura, J.; Shinada, Y.; Suzuki, C.; Ohtori, S. Does the surgical approach influence the implant alignment in total hip arthroplasty? Comparative study between the direct anterior and the anterolateral approaches in the supine position. Int. Orthop. 2017, 41, 2487–2493. [Google Scholar] [CrossRef] [PubMed]
- van Oldenrijk, J.V.; Hoogland, P.V.J.M.; Tuijthof, G.J.M.; Corveleijn, R.; Noordenbos, T.W.H.; Schafroth, M.U. Soft tissue damage after minimally invasive THA. Acta Orthop. 2010, 81, 696–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, L.G.H.; Buxton, R.A. The course of the superior gluteal nerve in the lateral approach to the hip. J. Bone Joint Surg. 1989, 71, 1239–1243. [Google Scholar] [CrossRef] [PubMed]
- Starke, V.; Stofferin, H.; Mannschatz, S.; Hörmann, R.; Dammerer, D.; Thaler, M. The anatomical course of the superior gluteal nerve with regard to the direct anterior approach for primary and revision total hip arthroplasty. J. Arthroplast. 2021, 36, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Unis, D.B.; Hawkins, E.J.; Alapatt, M.F.; Benitez, C.L. Postoperative changes in the tensor fascia Lata muscle after using the modified anterolateral approach for total hip arthroplasty. J. Arthroplast. 2013, 28, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Grob, K.; Manestar, M.; Ackland, T.; Filgueira, L.; Kuster, M.S. Potential risk to the superior gluteal nerve during the anterior approach to the hip joint: An anatomical study. J. Bone Jt. Surg. Am. 2015, 97, 1426–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismailidis, P.; Kvarda, P.; Vach, W.; Cadosch, D.; Appenzeller-Herzog, C.; Mündermann, A. Abductor Muscle Strength Deficit in Patients After total hip arthroplasty: A systematic Review and Meta-Analysis. J. Arthroplast. 2021, 36, 3015–3027. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-Operatively | 12 Months | Statistics | |
|---|---|---|---|
| Oi | 0.94 (±0.0089) | 0.92 (±0.010) | p = 0.13 |
| Oe | 0.95 (±0.0098) | 0.92 (±0.018) | p = 0.19 |
| Gmed | 0.94 (±0.0055) | 0.86 (±0.012) | p < 0.0001 |
| Gmin | 0.87 (±0.010) | 0.78 (±0.015) | p < 0.0001 |
| TFL | 0.90 (±0.017) | 0.71 (±0.025) | p < 0.0001 |
| Pre-Operatively | 12 Months | Statistics | |
|---|---|---|---|
| Oi | 769.4 (±19.9) | 758.8 (±20.0) | p = 0.36 |
| Oe | 1163.6 (±41.0) | 1137.2 (±41.5) | p = 0.27 |
| Gmed | 2203.9 (±54.6) | 2059.1 (±58.0) | p = 0.0002 |
| Gmin | 880.1 (±26.3) | 804.2 (±24.9) | p = 0.0002 |
| TFL | 530.8 (±20.1) | 449.9 (±23.6) | p = 0.0001 |
| Oi (%) | Oe (%) | Gmed (%) | Gmin (%) | TFL (%) | |
|---|---|---|---|---|---|
| No atrophy: >75% | 62 (94%) | 63 (95%) | 62 (94%) | 61 (92%) | 47 (71%) |
| Slight atrophy: 50–75% | 4 (6%) | 3 (5%) | 4 (6%) | 5 (8%) | 16 (24%) |
| Moderate atrophy: 25–50% | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 3 (5%) |
| Severe atrophy: <25% | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Pre-Operatively | 12 Months | Statistics | |
|---|---|---|---|
| Oi | 0.17 (±0.51) | 0.26 (±0.062) | p = 0.057 |
| Oe | 0.71 (±0.064) | 0.83 (±0.059) | p = 0.059 |
| Gmed | 1.24 (±0.057) | 1.33 (±0.069) | p = 0.057 |
| Gmin | 2.21 (±0.079) | 2.26 (±0.090) | p = 0.47 |
| TFL | 1.36 (±0.060) | 1.55 (±0.081) | p = 0.0063 |
| Oi (%) | Oe (%) | Gmed (%) | Gmin (%) | TFL (%) | |
|---|---|---|---|---|---|
| Improved | 2 (3%) | 3 (5%) | 2 (3%) | 4 (6%) | 0 (0%) |
| No change | 58 (88%) | 55 (83%) | 57 (86%) | 53 (80%) | 58 (88%) |
| Worsened | 6 (9%) | 8 (2%) | 7 (11%) | 9 (14%) | 8 (12%) |
| TFL Atrophy | No TFL Atrophy | Statistics | |
|---|---|---|---|
| Number | 19 | 47 | N/A |
| Age | 68.5 (±9.6) | 68.6 (±8.2) | p = 0.97 |
| Gender (Female/Male) | 14/5 | 37/10 | p = 0.91 |
| BMI | 25.5 (±3.0) | 25.0 (±2.9) | p = 0.53 |
| Pre-operative Harris hip score | 48.0 (±7.9) | 46 (±7.5) | p = 0.34 |
| Post-operative Harris hip score | 91.9 (±2.3) | 90.7 (±6.7) | p = 0.43 |
| Operative time (min) | 97.7 (±5.5) | 95.4 (±6.6) | p = 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oda, S.; Hisatome, T.; Cho, E.; Fujimaki, H.; Nakanishi, K. MRI Findings of Muscle Damage after Total Hip Arthroplasty Using the Complete Muscle Preserving Anterolateral Supine Approach. Medicina 2022, 58, 713. https://doi.org/10.3390/medicina58060713
Oda S, Hisatome T, Cho E, Fujimaki H, Nakanishi K. MRI Findings of Muscle Damage after Total Hip Arthroplasty Using the Complete Muscle Preserving Anterolateral Supine Approach. Medicina. 2022; 58(6):713. https://doi.org/10.3390/medicina58060713
Chicago/Turabian StyleOda, Shuhei, Takashi Hisatome, Eiji Cho, Hirohisa Fujimaki, and Kazuyoshi Nakanishi. 2022. "MRI Findings of Muscle Damage after Total Hip Arthroplasty Using the Complete Muscle Preserving Anterolateral Supine Approach" Medicina 58, no. 6: 713. https://doi.org/10.3390/medicina58060713