1. Introduction
The use of the superficial circumflex iliac artery (SCIA) perforator (SCIP) flap has become popular as its anatomy was well described [
1,
2,
3,
4,
5]. The elevation technique is safe, and the scar can be concealed. In addition, the donor site morbidity is low [
5]. The SCIP flap has been mainly used for extremity reconstruction. Recent advances have expanded its use ranging from head-and-neck to breast to toe reconstruction [
6,
7,
8]. Each of the SCIA branches is used as the pedicle; the skin flap is based on the superficial branch, and the sartorius muscle or the iliac bone flap is harvested based on the deep branch. By combining these branches, a chimeric flap can also be elevated [
4].
The conventional SCIP flap is harvested on the deep fascia, including the whole fat layers [
9]. Amongst donor-site morbidities of the SCIP flap are prolonged drain stay and lymphorrhea that develop due to damaging the lymphatic vessels in the deep fat. One study reported that one out of 210 patients developed lymphorrhea after the SCIP flap elevation [
10]. Recently, in pursuit of ideal resources, a thinner flap has been used for face or extremity reconstruction in which a skin flap is elevated above the superficial fascia [
10,
11,
12,
13,
14,
15]. Although this is less invasive to the donor site with the deep fat remained, the technique is challenging.
As we routinely use the SCIP flap, we have noticed a distinct fascia between the superficial and the deep fascia. We hypothesized that flap elevation above this fascia enables to save the deepest fat in a safer way as a modification of the conventional procedure, contributing to minimizing the invasiveness and enhancing the reliability simultaneously.
In this study, we introduce our modification of SCIP flap elevation saving a thin layer of the deeper fat tissue. We also compared the reconstructive result and donor site morbidity.
2. Materials and Methods
After the approval of the Institutional Review Board at Cancer Institute Hospital (2021-GB-101), all patients who had undergone the SCIP flap reconstruction with sarcoma excision by senior surgeons (YF, RK, and HY) from January 2020 through December 2021 were identified retrospectively. We excluded patients who underwent the SCIP flap transplant based on the deep branch of the SCIA, those who had non-spindle shaped SCIP flap transplant or those who had previous operations in the abdomen. The collected data included patient demographics, the location of the defect, the flap size, the elevation layer, the total operative time, the survival of flap, the duration of drain stay, the development of donor-site complications such as seroma and lymphocyst during the postoperative one month, and the necessity of revision to correct the bulkiness of the flap.
2.1. Deep Fat Saving Technique
We elevated the SCIP flap in either the supine or the lateral decubitus position under general anesthesia. The superficial branch of the SCIA was identified using a high-resolution ultrasound system (Vevo MD ultrasound device, Fujifilm Visual Sonics, Amsterdam, the Netherlands) [
16]. The flap size was decided in accordance with the defect dimension, and a spindle-shaped skin paddle was designed along the superficial branch. Based on careful consideration of the defect thickness, an SCIP flap was elevated conventionally above the Scarpa fascia or using the “deep fat saving technique”.
An SCIP flap was elevated in a proximal-to-distal fashion [
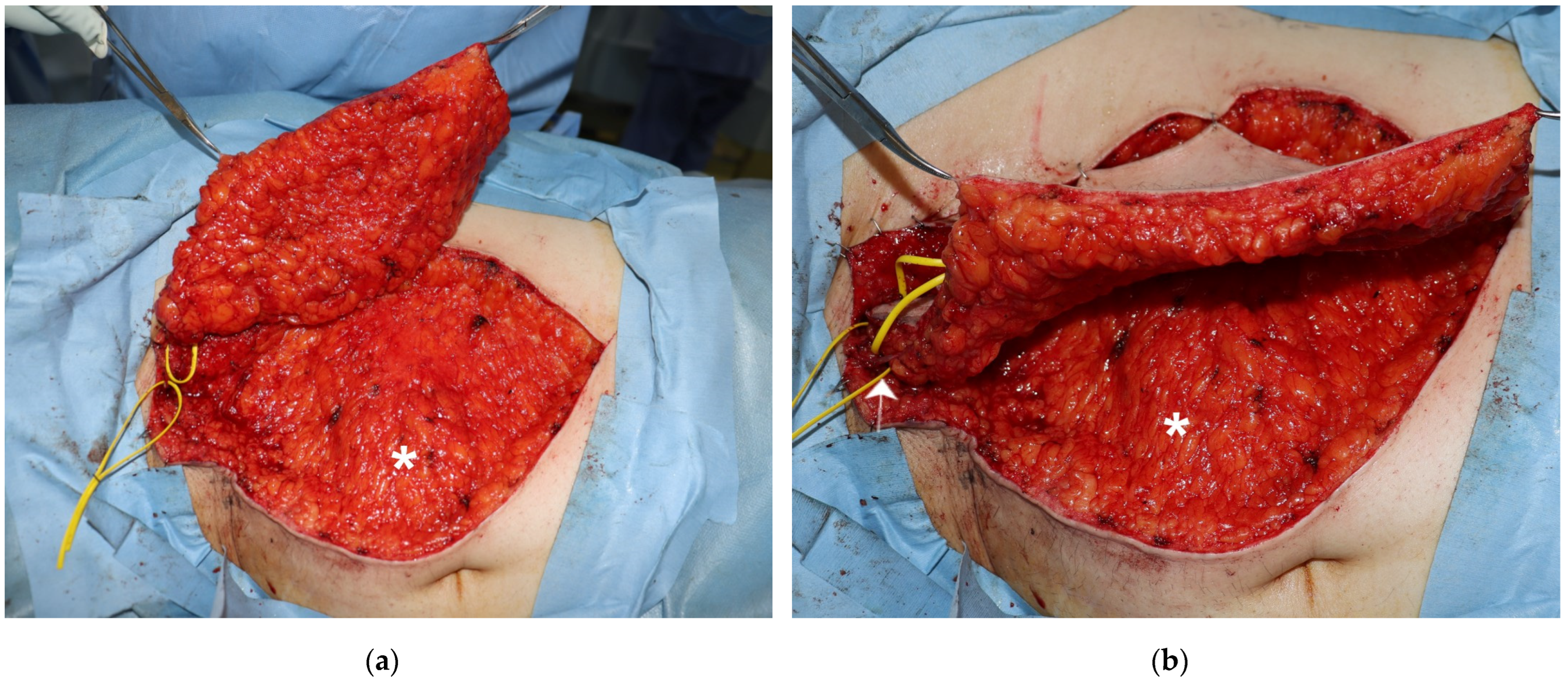
9]. A 3–4 cm skin incision was made along the pedicle marking. The pedicle was identified in the fat tissue and dissected proximally for the required length. The skin was then cut along the flap design. The fat tissue was dissected down. During the dissection, the superficial fascia was exposed and incised. Between the superficial and the Scarpa fasciae, another white fascia that is referred to as the Camper fascia was identified [
17]. The skin flap was elevated above this fascia, and the deeper fat was saved (
Figure 1). After the elevation was completed, the flap perfusion was confirmed on indocyanine green angiography [
18]. Recipient vessels were prepared within or in the adjacent of the defect after tumor excision. The free SCIP flap was transplanted, and microsurgical anastomosis was established.
The donor wound was closed directly over one suction drain of 15 Fr (BLAKE drain, Ethicon, Bridgewater, NJ, USA). The drain was maintained for at least two days and removed if discharge was less than 20 mL per day.
2.2. Statistical Analysis
Numeric variables were described using median and interquartile range (IQR), and categorical variables were shown using number and proportion. We compared the frequency of the postoperative morbidities (total or partial necrosis of the SCIP flap and donor site complications) and the duration of drain stay between the conventional and the DFS groups. The inverse probability weighting (IPW) method was used to minimize the potential imbalances between the groups [
19]. The propensity score estimating the probability of receiving the Deep Fat Saving technique was calculated using a logistic regression model with the following valuables: age, sex, body mass index (BMI), smoking history, preexisting medical conditions, the dimension of the flap, and the location of the defect. Age was categorized into two groups: <65 and ≥65 years. BMI was grouped into two: <25 and ≥25 kg/m2. These predictor factors were chosen based on consensus amongst the investigators. The thresholds categorizing the patients were decided in accordance with previous knowledge [
20,
21]. Weights were calculated for each patient as the inverse of the propensity score for the DFS group and the inverse of one minus the propensity score for the conventional group. A standardized difference of 0.10 or less was considered a negligible imbalance between groups. A weighted difference in length of drain stay was estimated using a linear regression model, respectively.
p values less than 0.05 were considered statistically significant. We used the R v. 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) for the data analyses.
3. Results
A total of 32 patients who underwent the SCIP flap reconstruction were reviewed. Out of them, 14 had the deep fat saving elevation (44%), while 18 had the conventional above-Scarpa elevation (56%). Baseline characteristics are summarized in
Table 1.
The flap survived in 14 and 17 patients in the DFS and conventional group, respectively (100 and 94%, p = 1.0). Lymphocyst developed in one case of the conventional group and subsided by aspiration. Drain stayed in the donor site for 6 days (IQR: 5.0–6.8 days) in the DFS and eight days (IQR: 7–9 days) in the conventional group, respectively.
3.1. Inverse Probability Weighting
After IPW, pseudo-populations were obtained with a size of 31.3 for the conventional group and 35.9 for the DFS group (
Table 1). All standardized mean differences were lower than 10%.
Table 2 compares postoperative complication rates between the weighted groups. The rates of flap necrosis and donor site morbidities were not significantly different, while the duration of drain stay was longer in the conventional group. The total operative time was similar. In a multiple regression analysis, the performance of the DFS technique decreased the drain stay by 1.6 days (0.4–2.8 days,
p = 0.01).
3.2. Clinical Cases
3.2.1. Case 1
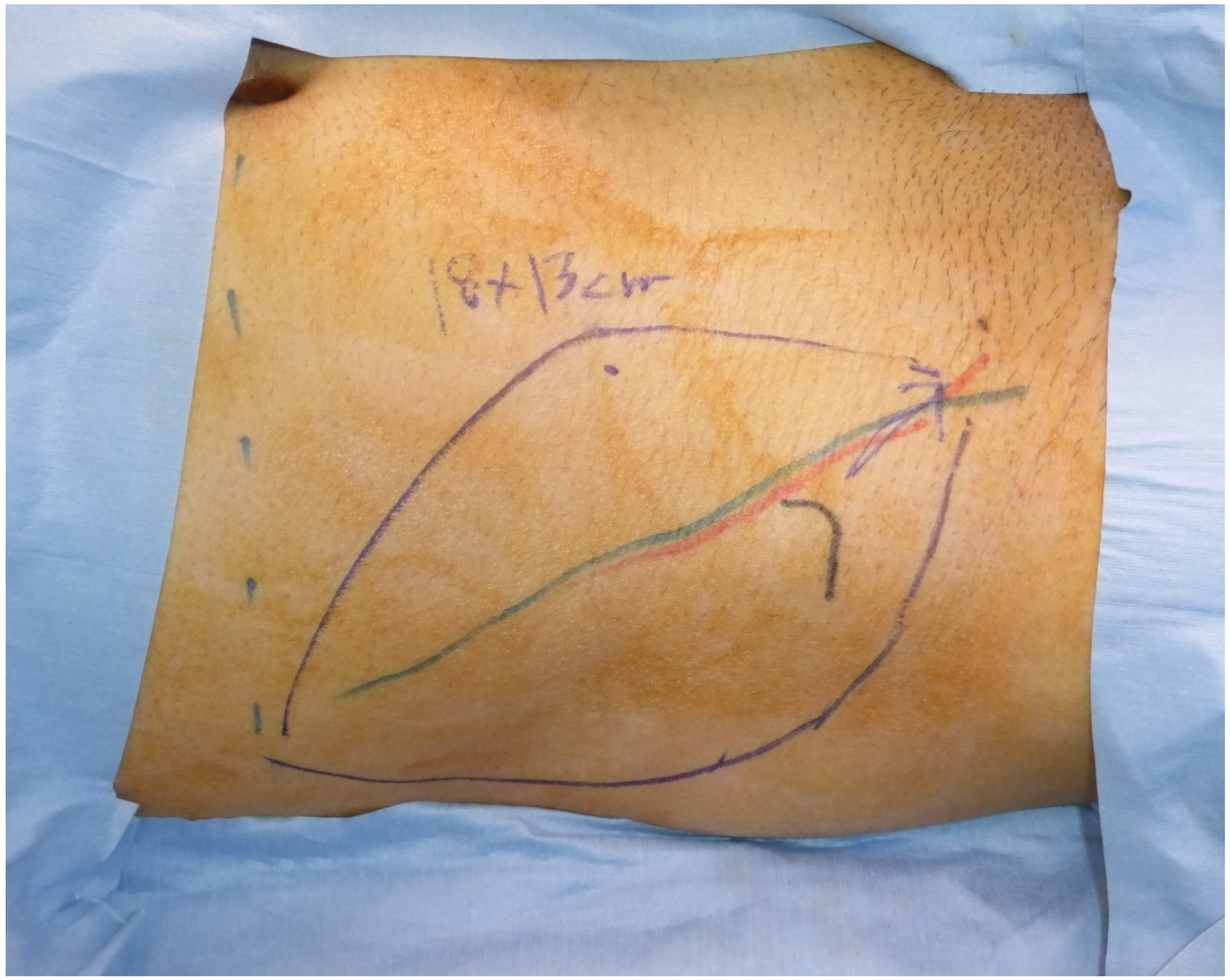
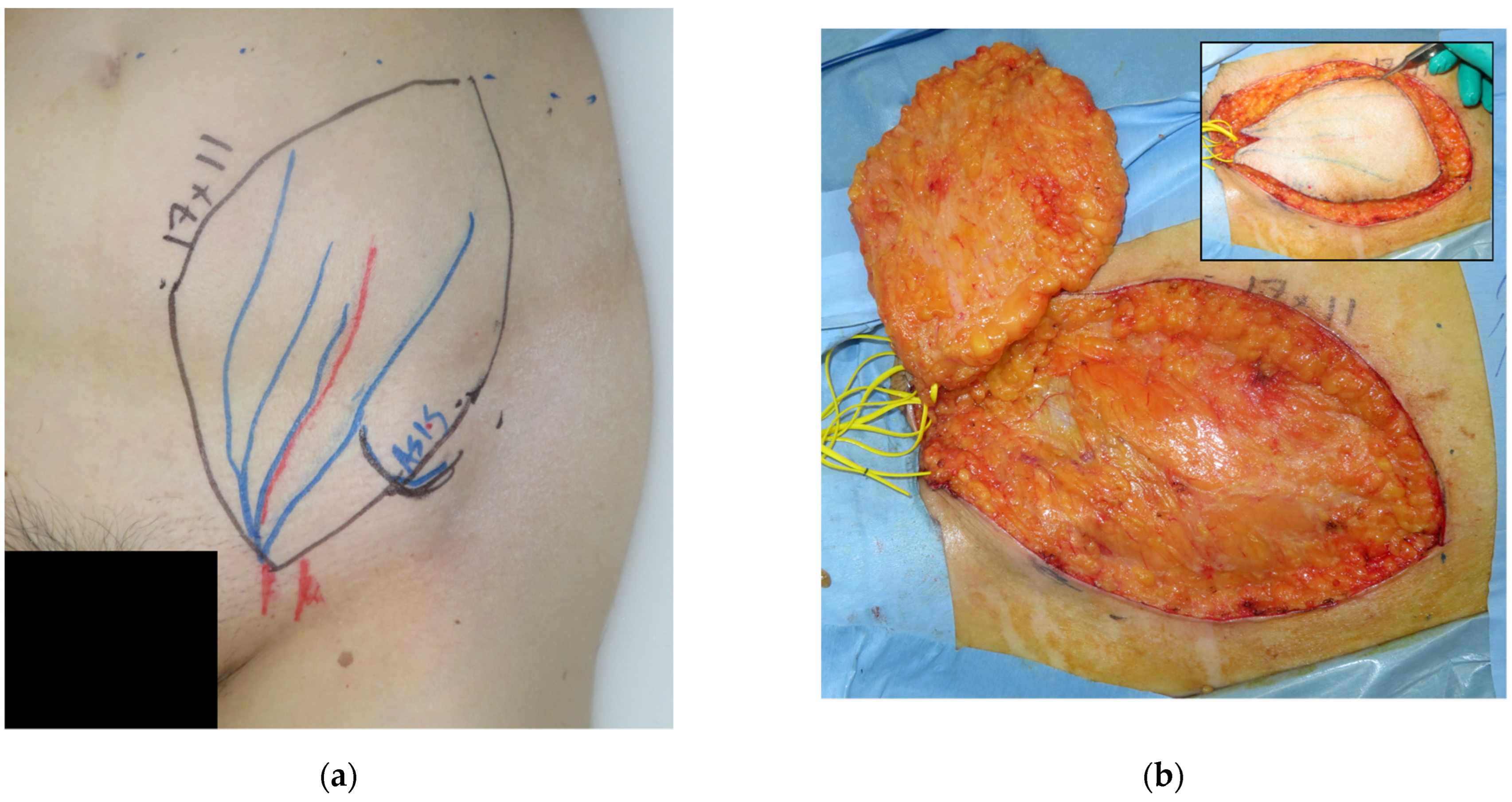
A forty-one-year-old man had wide excision of a soft tissue tumor in the left groin. An SCIP flap of 18 × 13 cm based on the superficial branch of the SCIA was harvested in the contralateral groin region (
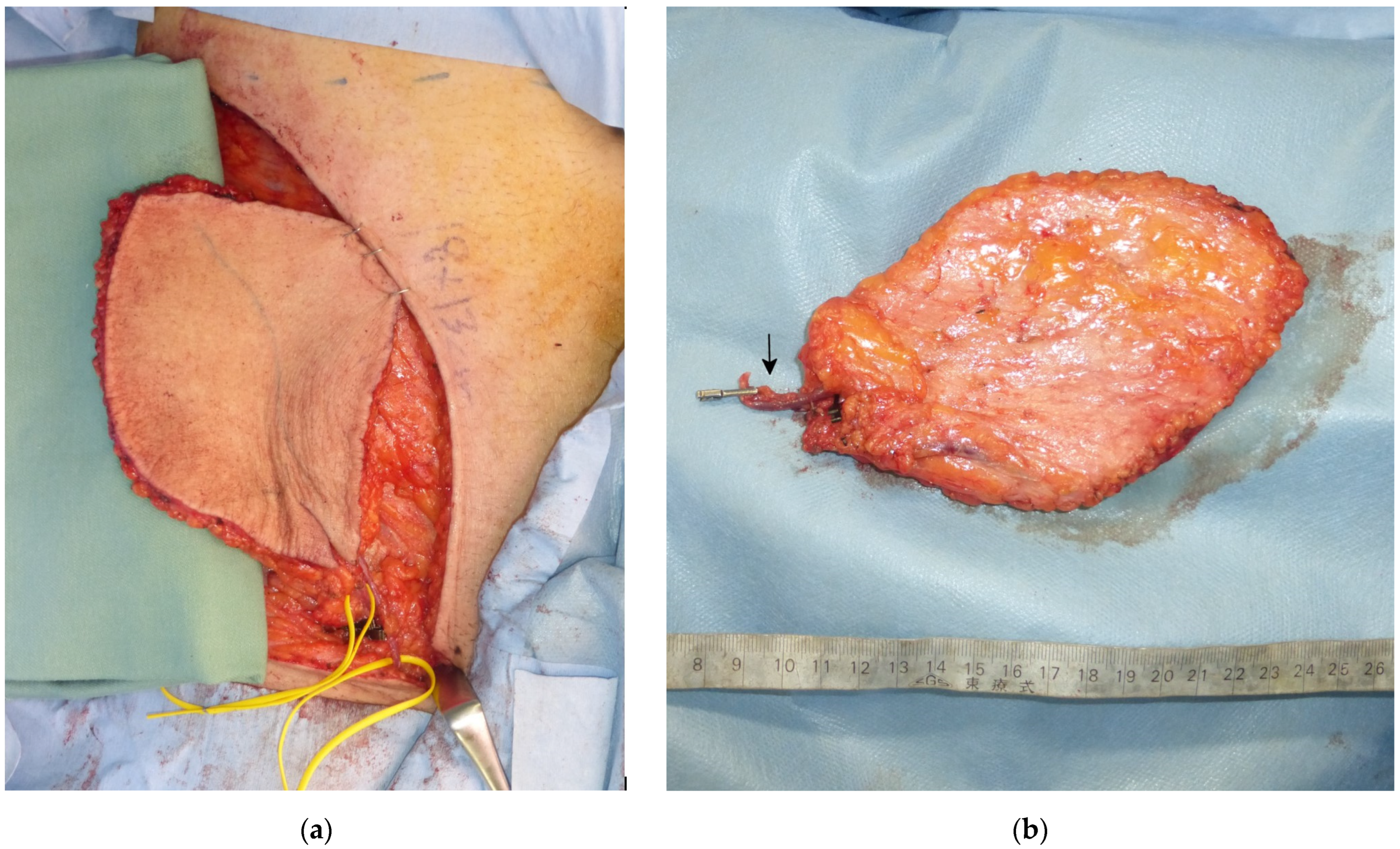
Figure 2). The skin flap was elevated saving the deep soft tissue (
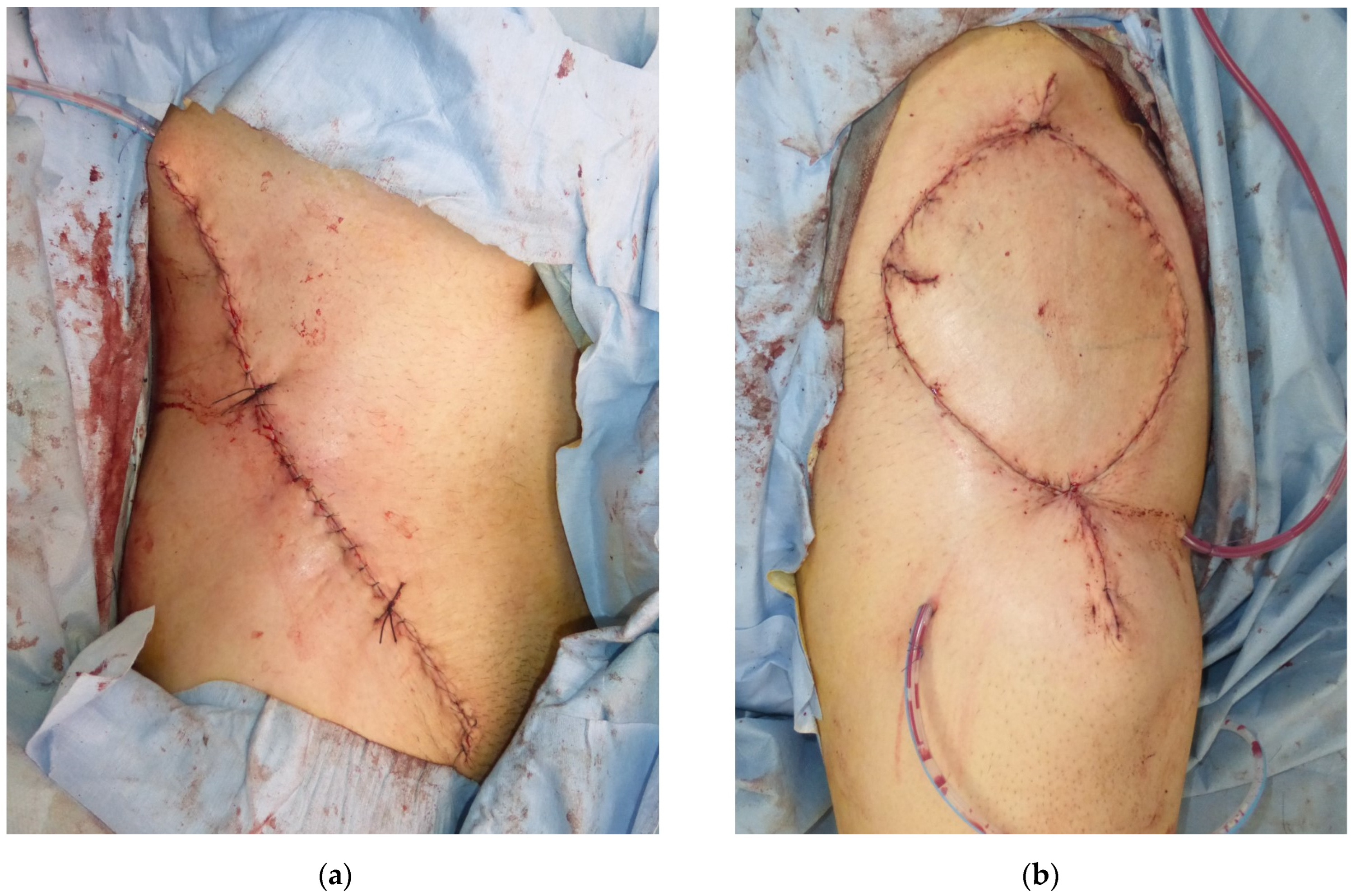
Figure 3) and transferred to the defect. The flap survived completely (
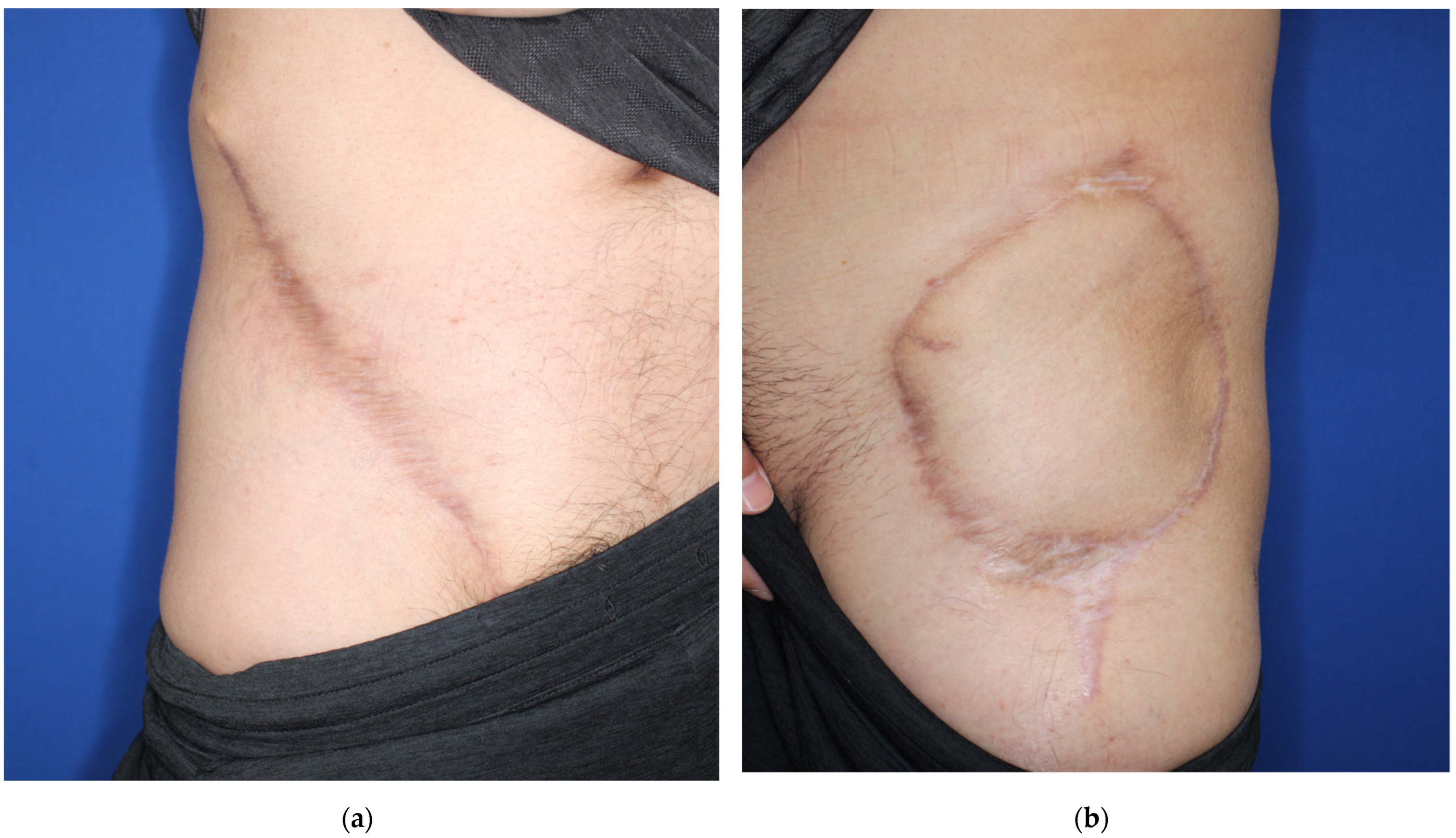
Figure 4). A suction drain was removed on postoperative day seven. No donor-site morbidity developed (
Figure 5).
3.2.2. Case 2
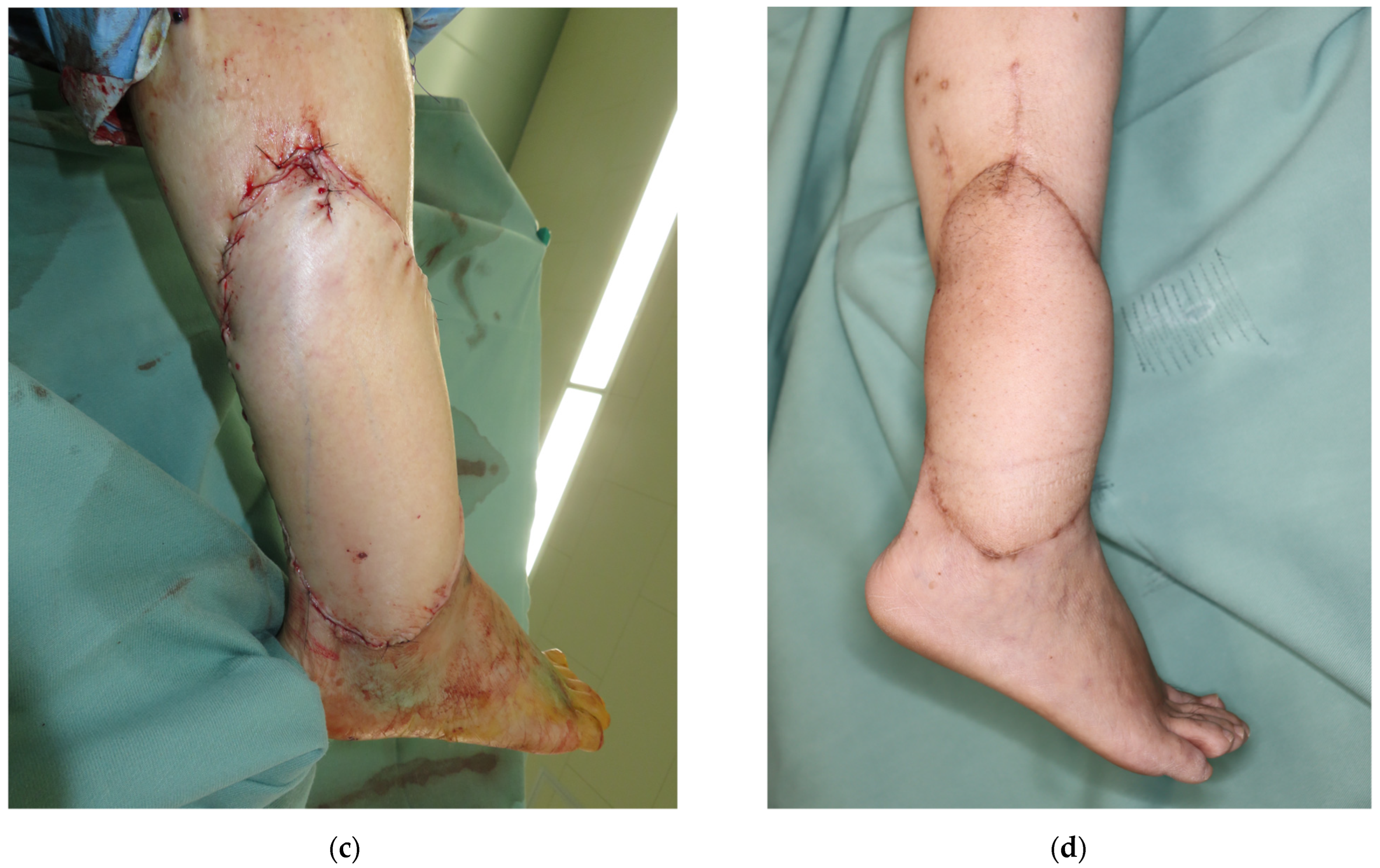
A 59-year-old woman was diagnosed with undifferentiated pleomorphic sarcoma in the lower leg. After wide excision, a 15 × 10 cm defect developed. We harvested an SCIP flap of 17 × 11 cm based on the superficial branch using the DFS technique (
Figure 6). The flap was transplanted, and the superficial branch and the superficial circumflex iliac vein were anastomosed to the peroneal artery and vein, respectively. The flap and the donor site healed without complications.
4. Discussion
We demonstrated a novel elevation technique of the SCIP flap, the Deep Fat Saving technique, in which the deeper fat tissue is saved. Reconstruction results were similar to the conventional SCIP flap elevation. By contrast, the duration of drain stay in the groin donor site was significantly shorter in the DFS group.
An elevation layer of the SCIP flap has been discussed in the pursuit of an ideal reconstruction resource [
10,
13,
14,
22]. In this context, the literature has mainly discussed how an SCIP flap is harvested for a thin defect with a skin flap elevated above the superficial fascia or below the dermis. Thin or ultrathin flap transplant can achieve aesthetically favorable reconstruction but requires well-experienced skills. Some surgeons advocated a safer way of thin flap elevation [
23].
By contrast, the present study shows a modification of the conventional SCIP flap elevation. An SCIP flap is conventionally elevated above the Scarpa fascia, including the whole layer of the fat tissue. This technique is simple and safe, but prolonged drain stay and lymphatic leakage at the donor site are often problems. In our population, one case of the conventional group developed lymphocyst, and aspiration was necessary. This results from the injury of the lymphatic vessels in the deep fat tissue, and it was alluded that the superficial fascia elevation of the ultrathin flap is less invasive with the lymphatic tissue saved [
12]. Considering this speculation, in our novel technique, damage to the lymphatic vessels can be minimized by leaving the deeper fat tissue. However, since the previously reported incidence of lymphorrhea after the SCIP flap elevation was low (<0.5%), the number of patients of the present study was so small that we cannot clearly conclude that the DFS technique offers the same results as the conventional technique.
The “superficial fascia” is the most superficial structure on which the thin flap is elevated [
10]. By this fascia, the fat tissue is divided into two layers: superficial and deep. The Camper fascia, which is located above the thin deepest fat [
17], is often equated with this superficial fascia. However, based on our accumulated experience, at least two fasciae are distinct in the abdominal and groin fat. Hereby, we advocate an idea that the superficial fascia and the Camper fascia should be considered different structures. By saving the thin fat below the Camper fascia, a relatively thick skin flap is harvested above the Camper fascia. Two patients underwent a revision to correct the bulky flap after the conventional flap elevation. This may be attributed to the patients’ body habitus, not to the elevation layer, since the thin deepest fat hardly affects the thickness of the flap.
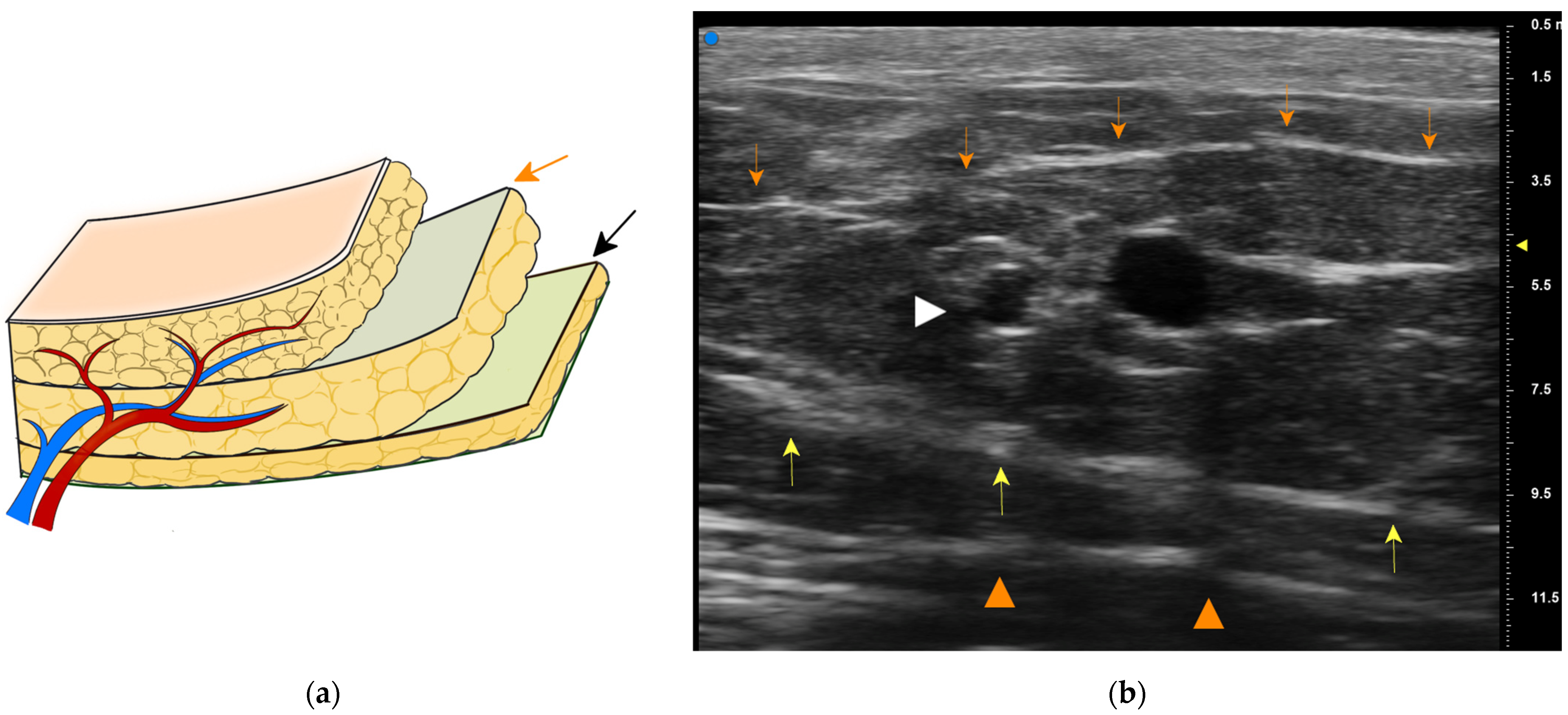
We routinely employ elevation in a proximal-to-distal fashion [
9]. A superficial branch of the SCIA is first identified in the proximal region, which is usually between the superficial and the Camper fasciae (
Figure 7). The pedicle is rather large and easy to be found with an aid of high-resolution ultrasonography [
16]. We then make a circumferential skin incision and dissect toward the Camper fascia. Thus, the pedicle above the Camper fascia is included safely. Furthermore, most of the pedicle is covered by the fat between two fasciae (
Figure 3b), contributing to safer transplant with a less possibility of kinking of the pedicle.
The covariates were well balanced through IPW by minimizing the effects of the confounders. Propensity score matching is the most prevailing method to balance the baseline confounders, but this would exclude large proportions of patients. Since the population in the present study is small, the loss of non-matched patients may distort the statistical inference. In the unweighted population, the flap dimension was rather small in the DFS group regardless of a statistically significant difference. However, by IPW, this variable was well-balanced, and confounding was minimized.
Limitations
The present study is limited by the small number of patients included. The results might be biased due to ethnicity: only Asian patients were enrolled. We did not measure the time of flap elevation. Instead, we employed the total operative time as a surrogate variable. Although we balanced the observed baseline demographics using IPW, unobserved confounders cannot be excluded without a randomized control study.
5. Conclusions
The present study demonstrated a novel elevation of the SCIP flap: Deep Fat Saving technique. Inverse probability weighing analysis indicated that drain stay at the donor site was shorter compared to the conventional group, while the rates of flap survival and donor site complications were similar. For patients with indications for the conventional SCIP flap transplant, the DFS technique may be a safe and reliable option.
Author Contributions
Conceptualization, Y.F.; methodology, Y.F.; software, Y.F.; validation, R.K.; formal analysis, Y.F.; investigation, Y.F.; resources, T.Y.; data curation, Y.F.; writing—original draft preparation, Y.F.; writing—review and editing, Y.F.; visualization, Y.F.; supervision, H.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Cancer Institute Hospital of the Japanese Foundation for Cancer Research on 25 February 2022 (Approval number: 2021-GB-101).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Y.F., upon reasonable request.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Altiparmak, M.; Cha, H.G.; Hong, J.P.; Suh, H.P. Superficial Circumflex Iliac Artery Perforator Flap as a Workhorse Flap: Systematic Review and Meta-analysis. J. Reconstr. Microsurg. 2020, 36, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Fuse, Y.; Yoshimatsu, H.; Karakawa, R.; Yano, T. Novel Classification of the Branching Patterns of the Superficial Branch and the Deep Branch of the Superficial Circumflex Iliac Artery and the Superficial Inferior Epigastric Artery on Computed Tomographic Angiography. J. Reconstr. Microsurg. 2021. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Jin, S.; Tian, Z.; Fang, Z.; Ma, C.; Tao, X.; Zhang, Y.; Qiu, W.; Zhang, Z.; Zhang, C. Superficial circumflex iliac artery perforator flap’s imaging, anatomy and clinical applications in oral maxillofacial reconstruction. J. Cranio-Maxillofac. Surg. 2016, 44, 242–248. [Google Scholar] [CrossRef]
- Yoshimatsu, H.; Steinbacher, J.; Meng, S.; Hamscha, U.M.; Weninger, W.J.; Tinhofer, I.E.; Harima, M.; Fuse, Y.; Yamamoto, T.; Tzou, C.H.J. Superficial Circumflex Iliac Artery Perforator Flap: An Anatomical Study of the Correlation of the Superficial and the Deep Branches of the Artery and Evaluation of Perfusion from the Deep Branch to the Sartorius Muscle and the Iliac Bone. Plast. Reconstr. Surg. 2019, 143, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Suh, H.S.P.; Jeong, H.H.; Choi, D.H.; Hong, J.P.J.P. Study of the Medial Superficial Perforator of the Superficial Circumflex Iliac Artery Perforator Flap Using Computed Tomographic Angiography and Surgical Anatomy in 142 Patients. Plast. Reconstr. Surg. 2017, 139, 738–748. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Meroni, M.; Fritsche, E.; Rajan, G. Superficial Circumflex Iliac Artery Perforator Flap in Advanced Head and Neck Reconstruction: From Simple to Its Chimeric Patterns and Clinical Experience with 22 Cases. Plast. Reconstr. Surg. 2022, 149, 721–730. [Google Scholar] [CrossRef]
- Yano, T.; Yoshimatsu, H.; Karakawa, R.; Fuse, Y.; Kuramoto, Y.; Shibata, T.; Suesada, N.; Miyashita, H. Use of a combined SIEA and SCIP based double pedicled abdominal flap for breast reconstruction. Microsurgery 2021, 41, 319–326. [Google Scholar] [CrossRef]
- Fuse, Y.; Yamamoto, T.; Kageyama, T.; Sakai, H.; Tsukuura, R.; Yoshimatsu, H.; Yamamoto, N. Domino Free Flap Transfer Using a Superficial Circumflex Iliac Artery Perforator Flap for the Toe Flap Donor Site. Ann. Plast. Surg. 2022, 88, 293–297. [Google Scholar] [CrossRef]
- Yoshimatsu, H.; Yamamoto, T.; Hayashi, A.; Iida, T. Proximal-to-Distally Elevated Superficial Circumflex Iliac Artery Perforator Flap Enabling Hybrid Reconstruction. Plast. Reconstr. Surg. 2016, 138, 910–922. [Google Scholar] [CrossRef] [Green Version]
- Goh, T.L.H.; Park, S.W.; Cho, J.Y.; Choi, J.W.; Hong, J.P. The Search for the Ideal Thin Skin Flap: Superficial Circumflex Iliac Artery Perforator Flap—A Review of 210 Cases. Plast. Reconstr. Surg. 2015, 135, 592–601. [Google Scholar] [CrossRef]
- Choi, D.H.; Suh, H.; Mukarramah, D.A.; Tashti, T.; Lee, K.; Yoon, C.; Hong, J.P. A New Plane of Elevation: The Superficial Fascial Plane for Perforator Flap Elevation. J. Reconstr. Microsurg. 2014, 30, 491–496. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.W.; Kim, Y.C.; Oh, T.S.; Koh, K.S.; Jeong, W.S. The versatile use of revisited de-epithelialization concept in superficial circumflex iliac and anterolateral thigh perforator free flap for head and neck reconstructions. J. Cranio-Maxillofac. Surg. 2017, 45, 872–880. [Google Scholar] [CrossRef]
- Lee, K.-T.; Park, B.Y.; Kim, E.-J.; Kim, J.-H.; Jang, K.-T.; Choi, S.-H.; Lee, D.-Y.; Mun, G.-H. Superthin SCIP Flap for Reconstruction of Subungual Melanoma: Aesthetic Functional Surgery. Plast. Reconstr. Surg. 2017, 140, 1278–1289. [Google Scholar] [CrossRef] [PubMed]
- Narushima, M.; Yamasoba, T.; Iida, T.; Matsumoto, Y.; Yamamoto, T.; Yoshimatsu, H.; Timothy, S.; Pafitanis, G.; Yamashita, S.; Koshima, I. Pure Skin Perforator Flaps: The Anatomical Vascularity of the Superthin Flap. Plast. Reconstr. Surg. 2018, 142, 351e–360e. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Yamamoto, N.; Fuse, Y.; Kageyama, T.; Sakai, H.; Tsukuura, R. Subdermal Dissection for Elevation of Pure Skin Perforator Flaps and Superthin Flaps: The Dermis as a Landmark for the Most Superficial Dissection Plane. Plast. Reconstr. Surg. 2021, 147, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Yoshimatsu, H.; Karakawa, R.; Fuse, Y.; Okada, A.; Hayashi, A.; Yano, T. Use of Preoperative High-Resolution Ultrasound System to Facilitate Elevation of the Superficial Circumflex Iliac Artery Perforator Flap. J. Reconstr. Microsurg. 2021, 37, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Lancerotto, L.; Stecco, C.; Macchi, V.; Porzionato, A.; Stecco, A.; De Caro, R. Layers of the abdominal wall: Anatomical investigation of subcutaneous tissue and superficial fascia. Surg. Radiol. Anat. 2011, 33, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Yoshimatsu, H.; Karakawa, R.; Scaglioni, M.F.; Fuse, Y.; Tanakura, K.; Yano, T. Application of intraoperative indocyanine green angiography for detecting flap congestion in the use of free deep inferior epigastric perforator flaps for breast reconstruction. Microsurgery 2021, 41, 522–526. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Holt, D.R.; Kirk, S.J.; Regan, M.C.; Hurson, M.; Lindblad, W.J.; Barbul, A. Effect of age on wound healing in healthy human beings. Surgery 1992, 112, 293–297; discussion 297–298. [Google Scholar]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut off Points. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 6 May 2022).
- Visconti, G.; Bianchi, A.; Hayashi, A.; Cina, A.; Maccauro, G.; Almadori, G.; Salgarello, M. Thin and superthin perforator flap elevation based on preoperative planning with ultrahigh-frequency ultrasound. Arch. Plast. Surg. 2020, 47, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Innocenti, M.; Calabrese, S.; Tanini, S.; Malzone, G.; Innocenti, A. A Safer Way to Harvest a Superthin Perforator Flap. Plast. Reconstr. Surg. 2021, 147, 466–469. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}