
Association between Hip Center Position and Isokinetic Hip Muscle Performance after Anterolateral Muscle-Sparing Total Hip Arthroplasty


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessments of Muscle Strength
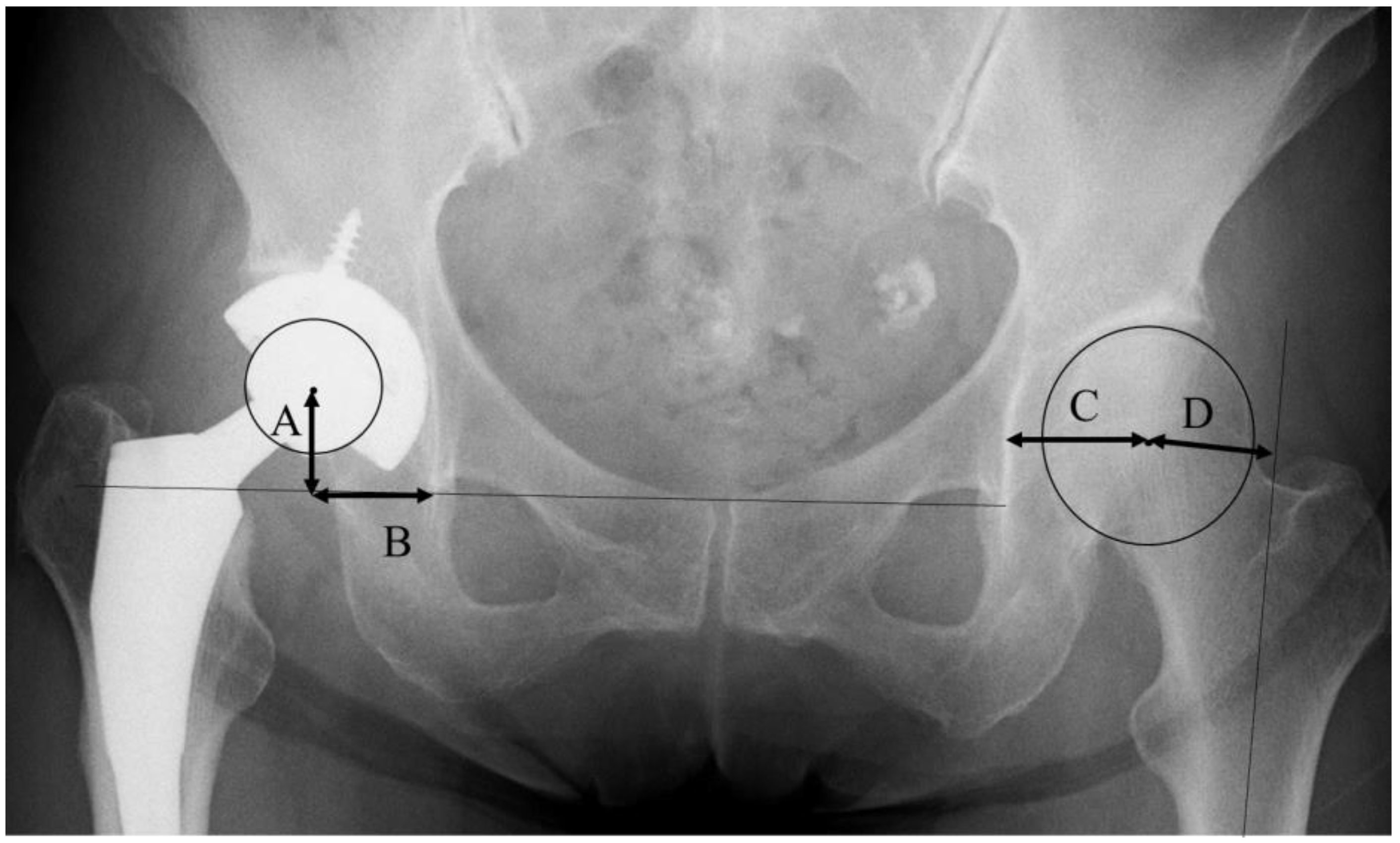
2.3. Measurements of Radiographs
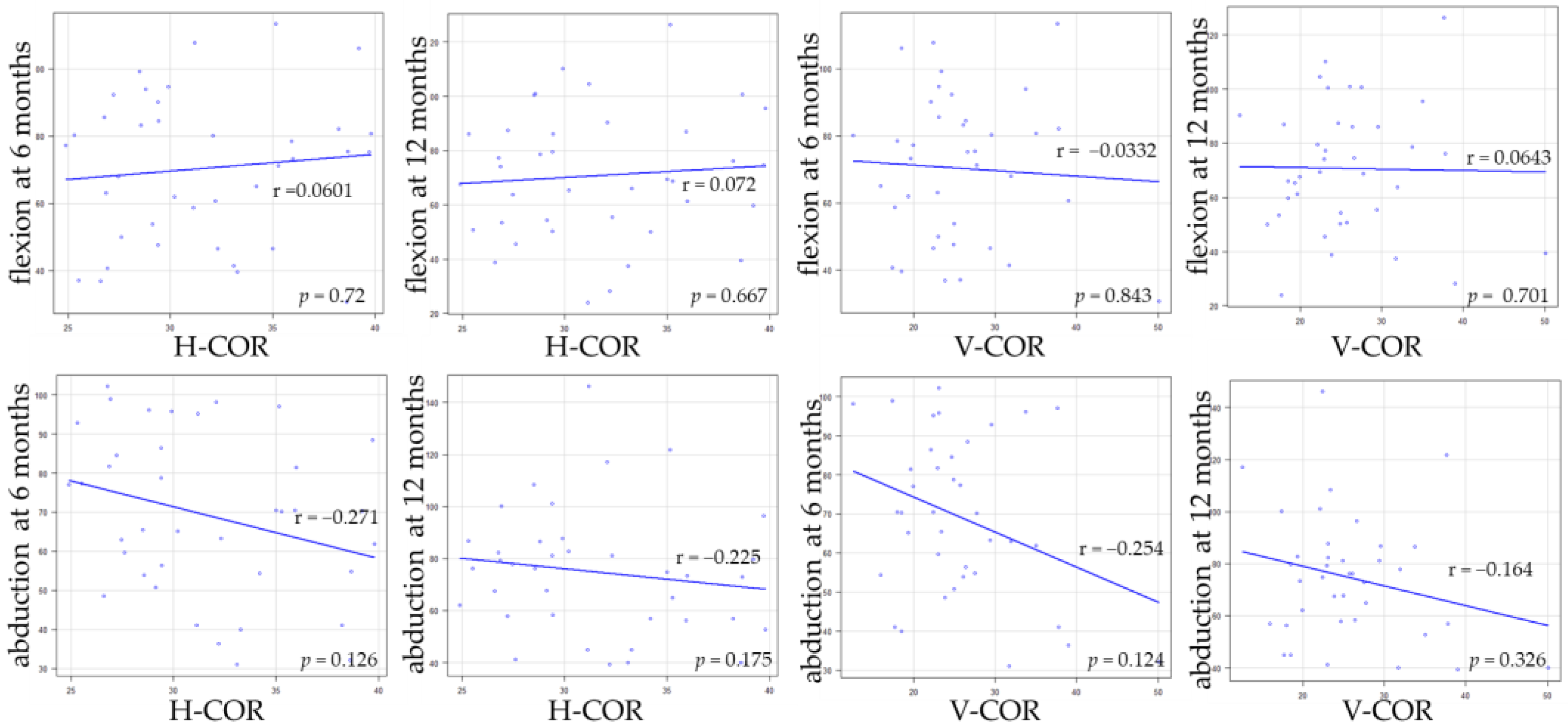
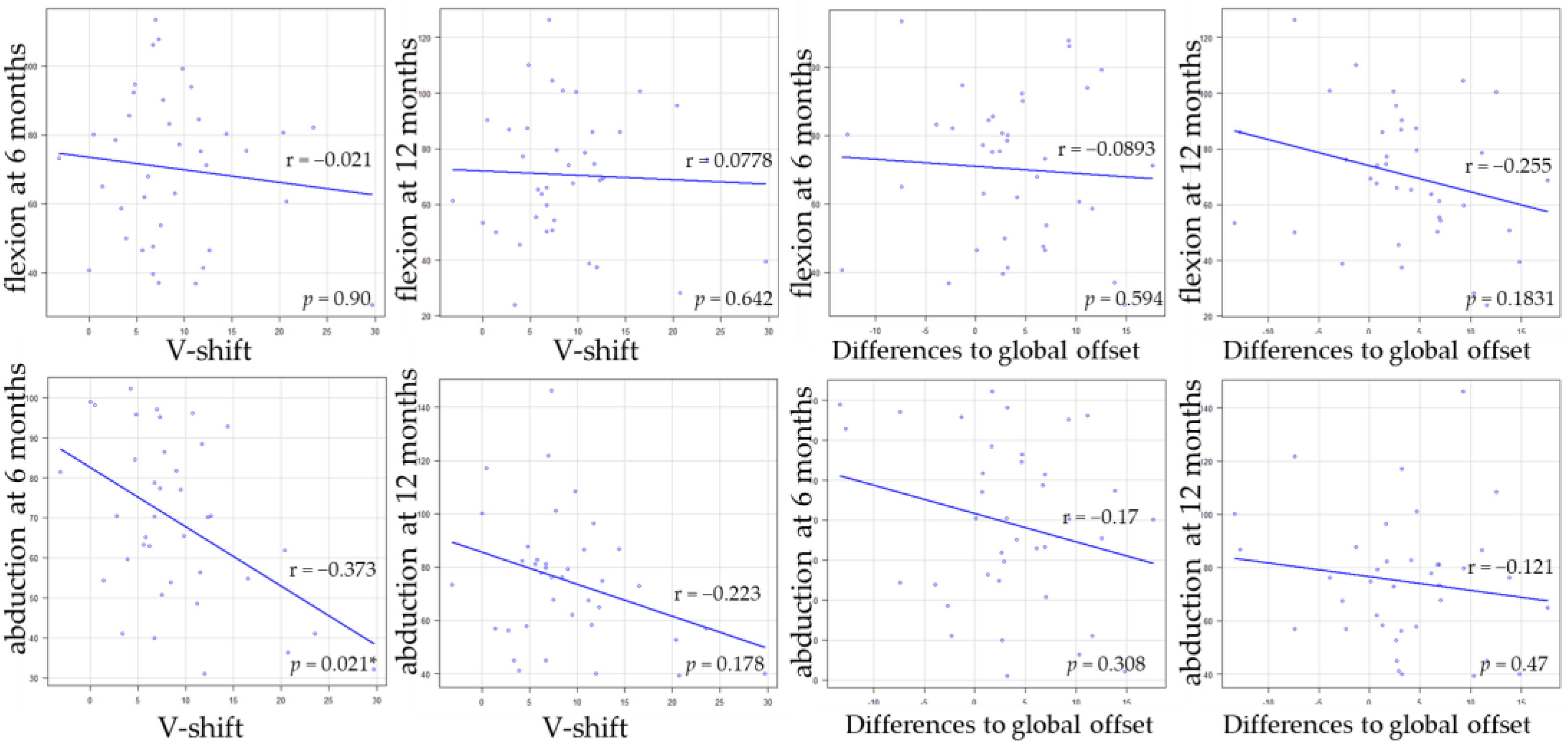
2.4. Statistical Analyses
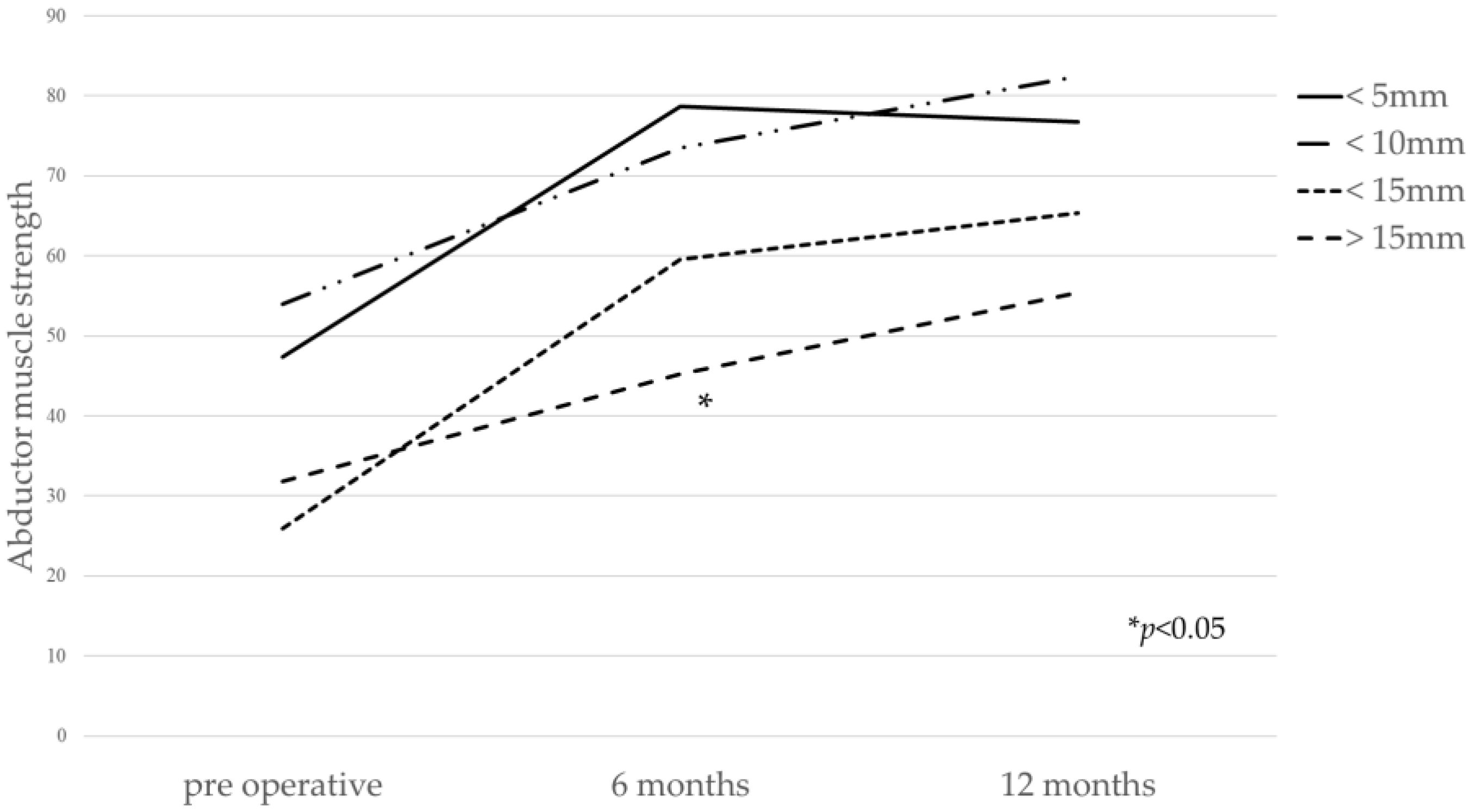
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anseth, S.D.; Pulido, P.A.; Adelson, W.S.; Patil, S.; Sandwell, J.C.; Colwell, C.W., Jr. Fifteen-year to twenty-year results of cementless Harris-Galante porous femoral and Harris-Galante porous I and II acetabular components. J. Arthroplast. 2010, 25, 687. [Google Scholar] [CrossRef] [PubMed]
- George, N.E.; Gwam, C.U.; Etcheson, J.I.; Smith, S.S.; Semenistyy, A.A.; Delanois, R.E. Short-term outcomes of the supine muscle-sparing anterolateral versus direct lateral approach to primary total hip arthroplasty. Hip. Int. 2019, 29, 504. [Google Scholar] [CrossRef] [PubMed]
- Leunig, M.; Faas, M.; von Knoch, F.; Naal, F.D. Skin crease ‘bikini’ incision for anterior approach total hip arthroplasty: Surgical technique and preliminary results. Clin. Orthop. Relat. Res. 2013, 471, 2245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Civinini, R.; Cozzi Lepri, A.; Carulli, C.; Matassi, F.; Villano, M.; Innocenti, M. The anterior-based muscle-sparing approach to the hip: The “other” anterior approach to the hip. Int. Orthop. 2019, 43, 47. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Yamada, N.; Kurishima, H.; Mori, Y.; Sakamoto, T.; Oyama, M.; Aizawa, T. Limited effects on patient outcomes of conjoint tendon release in anterolateral muscle-sparing total hip arthroplasty. J. Orthop. Surg. Res. 2021, 16, 485. [Google Scholar] [CrossRef] [PubMed]
- Rasch, A.; Dalen, N.; Berg, H.E. Muscle strength, gait, and balance in 20 patients with hip osteoarthritis followed for 2 years after THA. Acta Orthop. 2010, 81, 183. [Google Scholar] [CrossRef] [PubMed]
- Frost, K.L.; Bertocci, G.E.; Wassinger, C.A.; Munin, M.C.; Burdett, R.G.; Fitzgerald, S.G. Isometric performance following total hip arthroplasty and rehabilitation. J. Rehabil. Res. Dev. 2006, 43, 435. [Google Scholar] [CrossRef] [PubMed]
- Judd, D.L.; Dennis, D.A.; Thomas, A.C.; Wolfe, P.; Dayton, M.R.; Stevens-Lapsley, J.E. Muscle strength and functional recovery during the first year after THA. Clin. Orthop. Relat. Res. 2014, 472, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiyama, T.; Naito, M.; Shitama, H.; Maeyama, A. Effect of superior placement of the hip center on abductor muscle strength in total hip arthroplasty. J. Arthroplast. 2009, 24, 240. [Google Scholar] [CrossRef] [PubMed]
- Chulsomlee, K.; Sa-Ngasoongsong, P.; Kulachote, N.; Sirisreetreerux, N.; Tuntiyatorn, P.; Vasaruchapong, S.; Thamyongkit, S.; Jarungvittayakon, C.; Wongsak, S.; Kawinwonggowit, V. Hip muscle power recovery after hip replacement using anterior-based muscle-sparing approach in elderly femoral neck fracture: A prospective study in 40 patients. Orthop. Res. Rev. 2018, 10, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismailidis, P.; Kvarda, P.; Vach, W.; Appenzeller-Herzog, C.; Mundermann, A. Abductor muscle strength deficit in patients after total hip arthroplasty for hip osteoarthritis: A protocol for a systematic review and meta-analysis. BMJ Open 2020, 10, e035413. [Google Scholar] [CrossRef] [PubMed]
- Bertocci, G.E.; Munin, M.C.; Frost, K.L.; Burdett, R.; Wassinger, C.A.; Fitzgerald, S.G. Isokinetic performance after total hip replacement. Am. J. Phys. Med. Rehabil. 2004, 83, 1. [Google Scholar] [CrossRef] [PubMed]
- Fukushi, J.I.; Kawano, I.; Motomura, G.; Hamai, S.; Kawaguchi, K.I.; Nakashima, Y. Does hip center location affect the recovery of abductor moment after total hip arthroplasty? Orthop. Traumatol. Surg. Res. 2018, 104, 1149. [Google Scholar] [CrossRef]
- Mahmood, S.S.; Mukka, S.S.; Crnalic, S.; Wretenberg, P.; Sayed-Noor, A.S. Association between changes in global femoral offset after total hip arthroplasty and function, quality of life, and abductor muscle strength. A prospective cohort study of 222 patients. Acta Orthop. 2016, 87, 36. [Google Scholar] [CrossRef] [PubMed]
- Crowe, J.F.; Mani, V.J.; Ranawat, C.S. Total hip replacement in congenital dislocation and dysplasia of the hip. J. Bone Jt. Surg. Am. 1979, 61, 15. [Google Scholar] [CrossRef] [Green Version]
- Pesce, V.; Maccagnano, G.; Vicenti, G.; Notarnicola, A.; Lovreglio, P.; Soleo, L.; Pantalone, A.; Salini, V.; Moretti, B. First case report of vanadium metallosis after ceramic-on-ceramic total hip arthroplasty. J. Biol. Regul. Homeost. Agents 2013, 27, 1063. [Google Scholar] [PubMed]
- Drouin, J.M.; Valovich-mcLeod, T.C.; Shultz, S.J.; Gansneder, B.M.; Perrin, D.H. Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. Eur. J. Appl. Physiol. 2004, 91, 22. [Google Scholar] [PubMed]
- Komiyama, K.; Nakashima, Y.; Hirata, M.; Hara, D.; Kohno, Y.; Iwamoto, Y. Does High Hip Center Decrease Range of Motion in Total Hip Arthroplasty? A Computer Simulation Study. J. Arthroplast. 2016, 31, 2342. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452. [Google Scholar] [CrossRef] [Green Version]
- Fujii, M.; Nakamura, T.; Hara, T.; Nakashima, Y.; Iwamoto, Y. Does radiographic coxa profunda indicate increased acetabular coverage or depth in hip dysplasia? Clin. Orthop. Relat. Res. 2015, 473, 2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of patients | 38 |
| Age at time of operation, mean ± SD (range) | 66.5 ± 7.9 (52–87) |
| Gender Female:Male, no. of patients (%) | 32 (84.2):6 (15.8) |
| Body mass index | 24.9 ± 3.5 |
| Diagnosis | |
| Osteoarthritis | 38 |
| Crowe classification | |
| 1 | 25 |
| 2 | 13 |
| 3 | 0 |
| 4 | 0 |
| Pre-Operation | At 6 Months | p-Value | At 12 Months | p-Value (for Pre-Operation) | p-Value (for Six Months) | |
|---|---|---|---|---|---|---|
| flexion | 42.3 ± 22.0 | 70.3 ± 21.6 | 0.000 * | 70.7 ± 23.4 | 0.000 * | 0.556 |
| abduction | 44.0 ± 27.0 | 69.3 ± 20.4 | 0.000 * | 74.8 ± 23.9 | 0.000 * | 0.0651 |
| Crowe Classification | Value | p-Value | |
|---|---|---|---|
| pre-operative leg length discrepancy (mm) | 1 | −5.6 ± 4.9 (−19.4~−3.3) | |
| 2 | −17.1 ± 9.8 (−31.3~−4.1) | 0.000 * | |
| post-operative leg length discrepancy (mm) | 1 | 0.7 ± 3.8 (−10.5~7.6) | |
| 2 | 0.4 ± 9.1 (−14.3~8.8) | 0.925 | |
| pre-operative global FO (mm) | 1 | 77.8 ± 7.2 (63.0~92.4) | |
| 2 | 74.8 ± 5.6 (62.3 ~83.5) | 0.275 | |
| post-operative global FO (mm) | 1 | 79.4 ± 7.8 (64.3~102.1) | |
| 2 | 77.9 ± 7.6 (65.8~90.4) | 0.236 | |
| V-COR (mm) | 1 | 23.0 ± 4.4 (12.6~31.9) | |
| 2 | 31.7 ± 8.2 (18.5 ~45.1) | 0.000 * | |
| H-COR (mm) | 1 | 29.9 ± 4.2 (24.9~39.7) | |
| 2 | 33.1 ± 4.7 (25.3~39.8) | 0.484 | |
| V-shift (mm) | 1 | 6.2 ± 4.3 (−3.1~16.5) | |
| 2 | 12.0 ± 7.0 (6.7~22.7) | 0.000 * |
| Crowe Classification | Pre-Operation | p-Value | At 6 Months | p-Value | At 12 Months | p-Value | |
|---|---|---|---|---|---|---|---|
| flexion | 1 | 42.2 ± 21.0 | 73.3 ± 18.9 | 67.6 ± 20.6 | |||
| 2 | 36.8 ± 21.0 | 0.498 | 80.3 ± 26.1 | 0.841 | 76.2 ± 27.8 | 0.633 | |
| abduction | 1 | 57.4 ± 23.9 | 70.5 ± 17.2 | 77.8 ± 22.4 | |||
| 2 | 32.8 ± 22.8 | 0.0157 * | 61.9 ± 23.4 | 0.113 | 72.8 ± 25.8 | 0.295 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, H.; Yamada, N.; Kurishima, H.; Mori, Y.; Aizawa, T. Association between Hip Center Position and Isokinetic Hip Muscle Performance after Anterolateral Muscle-Sparing Total Hip Arthroplasty. Medicina 2022, 58, 538. https://doi.org/10.3390/medicina58040538
Tanaka H, Yamada N, Kurishima H, Mori Y, Aizawa T. Association between Hip Center Position and Isokinetic Hip Muscle Performance after Anterolateral Muscle-Sparing Total Hip Arthroplasty. Medicina. 2022; 58(4):538. https://doi.org/10.3390/medicina58040538
Chicago/Turabian StyleTanaka, Hidetatsu, Norikazu Yamada, Hiroaki Kurishima, Yu Mori, and Toshimi Aizawa. 2022. "Association between Hip Center Position and Isokinetic Hip Muscle Performance after Anterolateral Muscle-Sparing Total Hip Arthroplasty" Medicina 58, no. 4: 538. https://doi.org/10.3390/medicina58040538