
New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress

 , , , , , ,
, , , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinical Profile and Mortality Rate of the Study Population
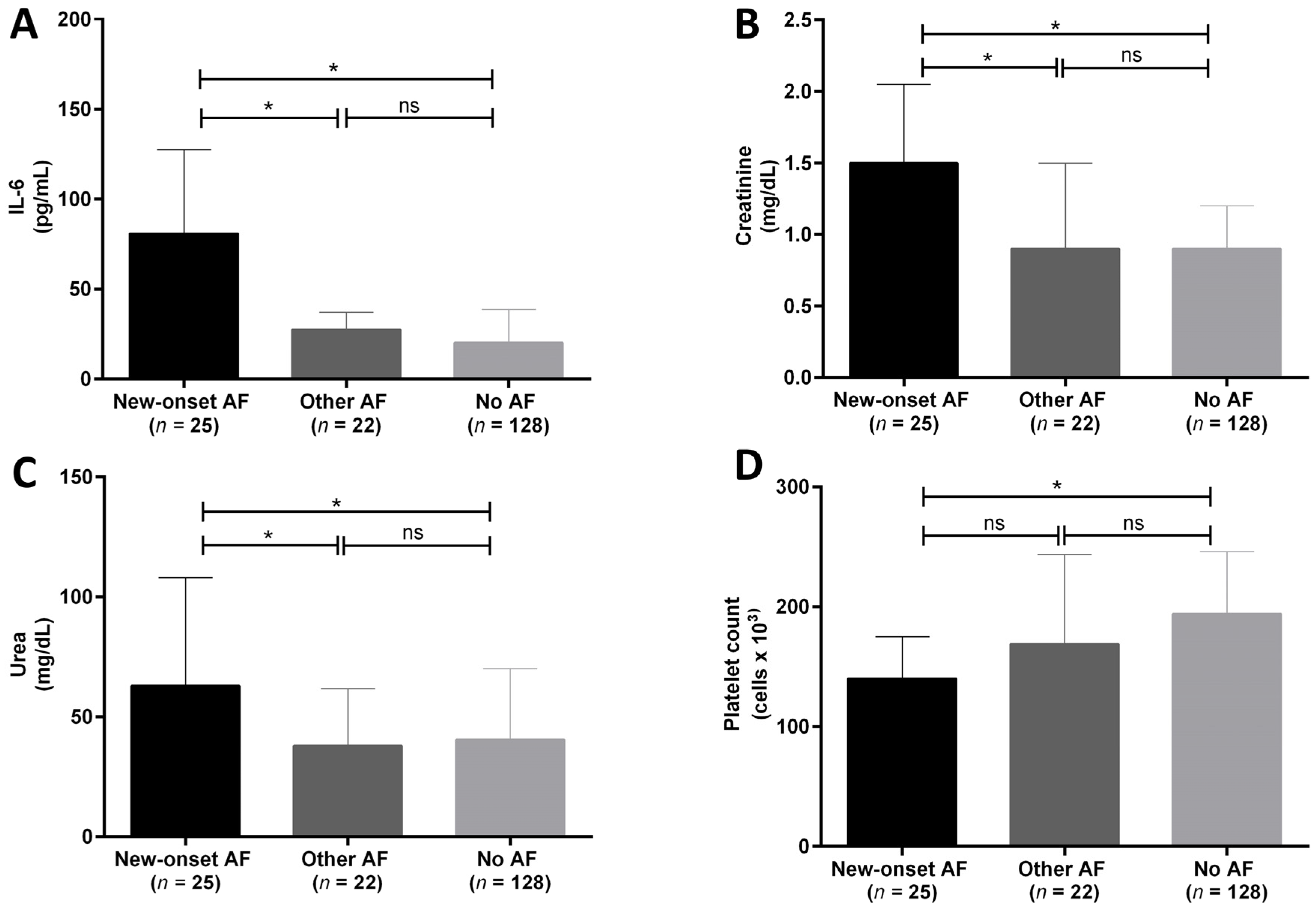
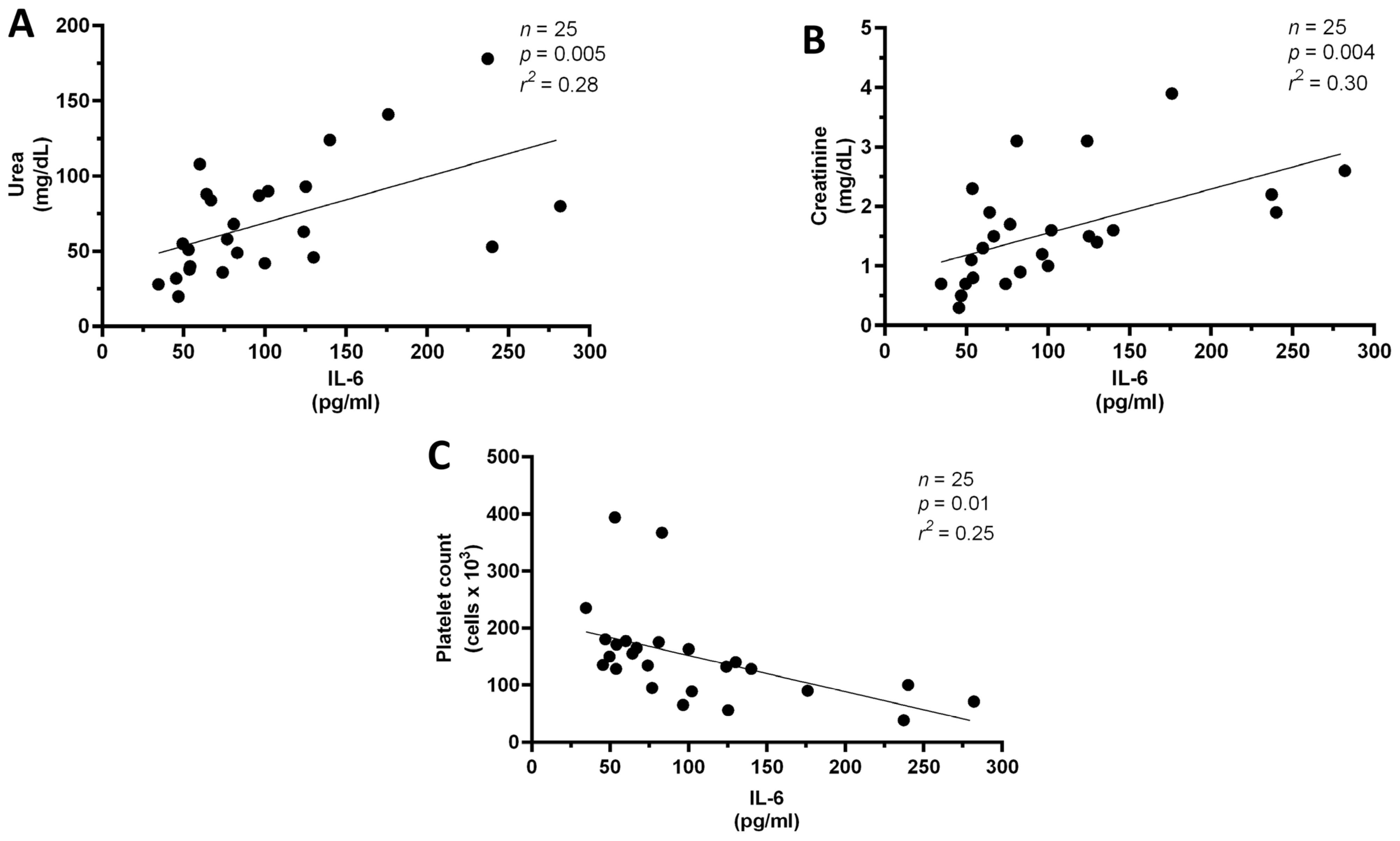
3.2. IL-6 Is Increased in New Onset AF and Is Associated with Specific Laboratory Parameters
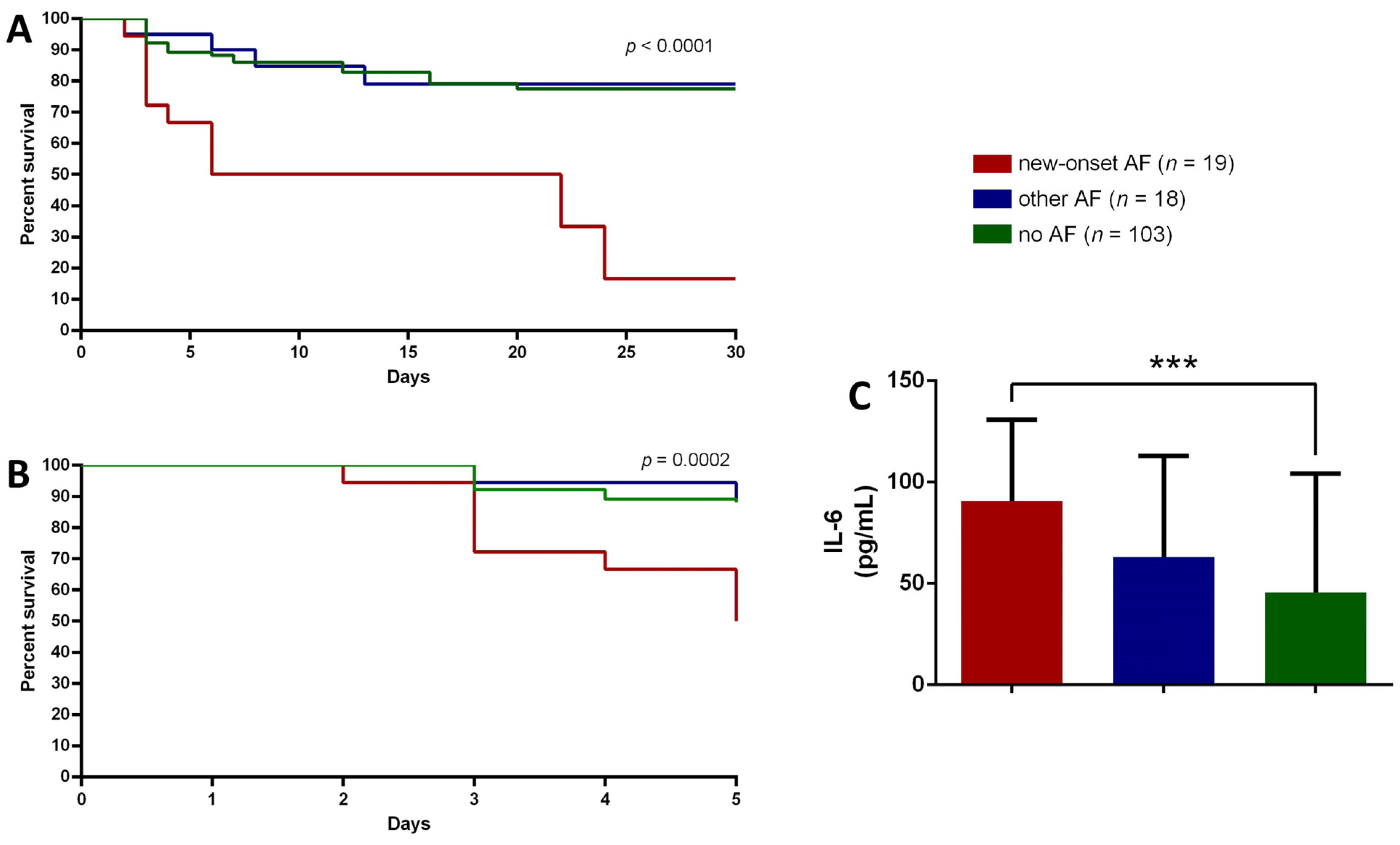
3.3. PaO2/FiO2 Stratification and Mortality
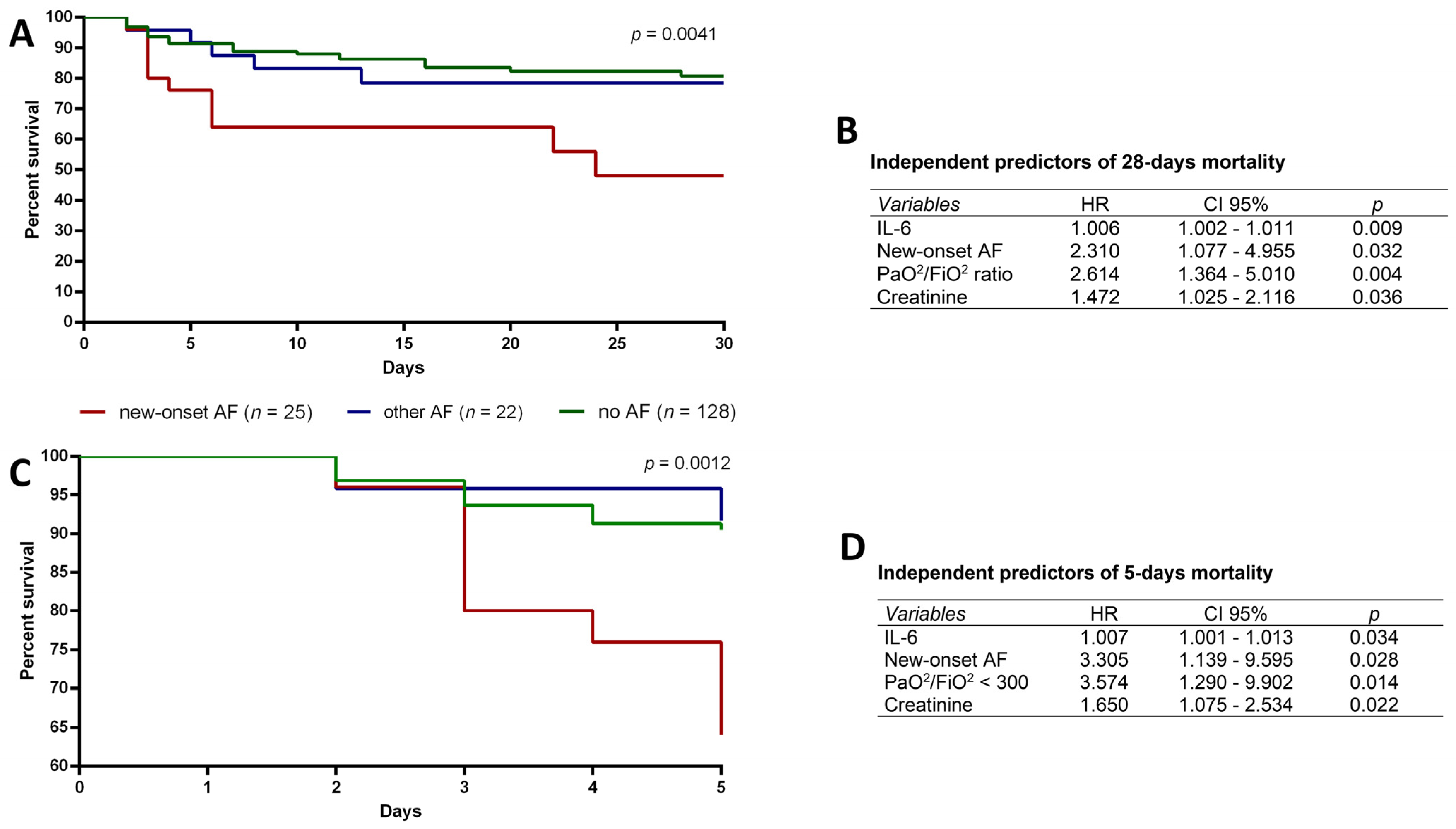
3.4. New Onset AF, IL-6, Creatinine and PaO2/FiO2 < 300 Are Independent Predictors of Mortality in COVID-19 Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections-More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Bagnato, G.; La Rosa, D.; Ioppolo, C.; De Gaetano, A.; Chiappalone, M.; Zirilli, N.; Viapiana, V.; Tringali, M.C.; Tomeo, S.; Aragona, C.O.; et al. The COVID-19 Assessment for Survival at Admission (CASA) Index: A 12 Months Observational Study. Front. Med. 2021, 8, 719976. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- Mann, C.Z.; Abshire, C.; Yost, M.; Kaatz, S.; Swaminathan, L.; Flanders, S.A.; Prescott, H.C.; Gagnon-Bartsch, J.A. Derivation and external validation of a simple risk score to predict in-hospital mortality in patients hospitalized for COVID-19: A multicenter retrospective cohort study. Medicine 2021, 100, e27422. [Google Scholar] [CrossRef]
- Bartoletti, M.; Giannella, M.; Scudeller, L.; Tedeschi, S.; Rinaldi, M.; Bussini, L.; Fornaro, G.; Pascale, R.; Pancaldi, L.; Pasquini, Z.; et al. Development and validation of a prediction model for severe respiratory failure in hospitalized patients with SARS-CoV-2 infection: A multicentre cohort study (PREDI-CO study). Clin. Microbiol. Infect. 2020, 26, 1545–1553. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Kang, Y.; Chen, T.; Mui, D.; Ferrari, V.; Jagasia, D.; Scherrer-Crosbie, M.; Chen, Y.; Han, Y. Cardiovascular manifestations and treatment considerations in COVID-19. Heart 2020, 106, 1132–1141. [Google Scholar] [CrossRef]
- Zylla, M.M.; Merle, U.; Vey, J.A.; Korosoglou, G.; Hofmann, E.; Muller, M.; Herth, F.; Schmidt, W.; Blessing, E.; Goggelmann, C.; et al. Predictors and Prognostic Implications of Cardiac Arrhythmias in Patients Hospitalized for COVID-19. J. Clin. Med. 2021, 10, 133. [Google Scholar] [CrossRef]
- Colon, C.M.; Barrios, J.G.; Chiles, J.W.; McElwee, S.K.; Russell, D.W.; Maddox, W.R.; Kay, G.N. Atrial Arrhythmias in COVID-19 Patients. JACC Clin. Electrophysiol. 2020, 6, 1189–1190. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Spanevello, A.; De Ponti, R.; Visca, D.; Marazzato, J.; Zappa, M.; Trapasso, M.; Masnaghetti, S.; Fabbri, L.M.; et al. Electrocardiographic features of patients with COVID-19: One year of unexpected manifestations. Eur. J. Intern. Med. 2021, 95, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Silverio, A.; Scudiero, F.; Micco, P.D.; Maio, M.D. Pre-admission atrial fibrillation in COVID-19 patients: Prevalence and clinical impact. Eur. J. Intern. Med. 2021, 88, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Angeli, F.; Spanevello, A.; De Ponti, R.; Visca, D.; Marazzato, J.; Palmiotto, G.; Feci, D.; Reboldi, G.; Fabbri, L.M.; Verdecchia, P. Electrocardiographic features of patients with COVID-19 pneumonia. Eur. J. Intern. Med. 2020, 78, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Genaidy, A.; Tran, G.; Marroquin, P.; Estes, C. Incident atrial fibrillation and its risk prediction in patients developing COVID-19: A machine learning based algorithm approach. Eur. J. Intern. Med. 2021, 91, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Harhay, J.; Khan, M.; Shah, S.; Malhotra, A. SARS-COV-2 Presenting as New Onset Atrial Fibrillation: A Case Report. Cureus 2020, 12, e8054. [Google Scholar] [CrossRef] [PubMed]
- Al-Abbas, O.; Alshaikhli, A.; Amran, H.A. New-Onset Atrial Fibrillation and Multiple Systemic Emboli in a COVID-19 Patient. Cureus 2021, 13, e12917. [Google Scholar] [CrossRef] [PubMed]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19. Cochrane Database Syst. Rev. 2021, 2, CD013665. [Google Scholar] [CrossRef]
- Musikantow, D.R.; Turagam, M.K.; Sartori, S.; Chu, E.; Kawamura, I.; Shivamurthy, P.; Bokhari, M.; Oates, C.; Zhang, C.; Pumill, C.; et al. Atrial Fibrillation in Patients Hospitalized With COVID-19: Incidence, Predictors, Outcomes, and Comparison to Influenza. JACC Clin. Electrophysiol. 2021, 7, 1120–1130. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19). Available online: Https://www.who.Int/emergencies/diseases/novel-coronavirus-2019?Gclid=cjwkcajwh5qlbhaleiwaioods84f_s9kgtvruxlozcy11ojpc6goks7opwpxawag4exjvskmagj0ohocfruqavd_bwe. (accessed on 10 April 2022).
- Vadakken, M.E.; Belley-Cote, E.P.; McIntyre, W.F. COVID-19 and AF: What About the Long Game? JACC Clin. Electrophysiol. 2021, 7, 1196–1197. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, D.; Carmo, P.; Cabanelas, N.; Santos, N.; Martins, V.; Sanfins, V.; Costa, H.C.; Fontes, J.P.; Fonseca, P.; Parreira, L.; et al. Cardiac arrhythmias in patients presenting with COVID-19 treated in Portuguese hospitals: A national registry from the Portuguese Association of Arrhythmology, Pacing and Electrophysiology. Rev. Port. Cardiol. 2021, 40, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Paris, S.; Inciardi, R.M.; Lombardi, C.M.; Tomasoni, D.; Ameri, P.; Carubelli, V.; Agostoni, P.; Canale, C.; Carugo, S.; Danzi, G.; et al. Implications of atrial fibrillation on the clinical course and outcomes of hospitalized COVID-19 patients: Results of the Cardio-COVID-Italy multicentre study. Europace 2021, 23, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Yarmohammadi, H.; Morrow, J.P.; Dizon, J.; Biviano, A.; Ehlert, F.; Saluja, D.; Waase, M.; Elias, P.; Poterucha, T.J.; Berman, J.; et al. Frequency of Atrial Arrhythmia in Hospitalized Patients With COVID-19. Am. J. Cardiol. 2021, 147, 52–57. [Google Scholar] [CrossRef]
- Iacopino, S.; Placentino, F.; Colella, J.; Pesce, F.; Pardeo, A.; Filannino, P.; Artale, P.; Desiro, D.; Sorrenti, P.; Campagna, G.; et al. New-Onset Cardiac Arrhythmias During COVID-19 Hospitalization. Circ. Arrhythmia Electrophysiol. 2020, 13, e009040. [Google Scholar] [CrossRef]
- Russo, V.; Di Maio, M.; Mottola, F.F.; Pagnano, G.; Attena, E.; Verde, N.; Di Micco, P.; Silverio, A.; Scudiero, F.; Nunziata, L.; et al. Clinical characteristics and prognosis of hospitalized COVID-19 patients with incident sustained tachyarrhythmias: A multicenter observational study. Eur. J. Clin. Investig. 2020, 50, e13387. [Google Scholar] [CrossRef]
- Yoshida, T.; Fujii, T.; Uchino, S.; Takinami, M. Epidemiology, prevention, and treatment of new-onset atrial fibrillation in critically ill: A systematic review. J. Intensive Care 2015, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Kelesoglu, S.; Yilmaz, Y.; Ozkan, E.; Calapkorur, B.; Gok, M.; Dursun, Z.B.; Kilic, A.U.; Demirelli, S.; Simsek, Z.; Elcik, D. New onset atrial fibrilation and risk faktors in COVID-19. J. Electrocardiol. 2021, 65, 76–81. [Google Scholar] [CrossRef]
- Mountantonakis, S.E.; Saleh, M.; Fishbein, J.; Gandomi, A.; Lesser, M.; Chelico, J.; Gabriels, J.; Qiu, M.; Epstein, L.M.; Northwell, C.-R.C. Atrial fibrillation is an independent predictor for in-hospital mortality in patients admitted with SARS-CoV-2 infection. Heart Rhythm 2021, 18, 501–507. [Google Scholar] [CrossRef]
- Pardo Sanz, A.; Salido Tahoces, L.; Ortega Perez, R.; Gonzalez Ferrer, E.; Sanchez Recalde, A.; Zamorano Gomez, J.L. New-onset atrial fibrillation during COVID-19 infection predicts poor prognosis. Cardiol. J. 2021, 28, 34–40. [Google Scholar] [CrossRef]
- Ruiz, L.A.; Serrano, L.; Espana, P.P.; Martinez-Indart, L.; Gomez, A.; Gonzalez, B.; Artaraz, A.; Zalacain, R. New-onset atrial fibrillation in patients with pneumococcal pneumonia. Impact of timing and duration on short- and medium-term mortality. J. Infect. 2021, 82, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Xue, B.; Chugh, K.; Bhanot, R.; Sankari, A. Septic Shock, Community-acquired Pneumonia, New-Onset Atrial Fibrillation, and Intensive Care Unit Outcomes. Am. J. Respir. Crit. Care Med. 2015, 192, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.H.; Chiang, H.J.; Yip, H.K.; Chen, K.J.; Chiang, J.Y.; Lee, M.S.; Sung, P.H. Risk of New-Onset Atrial Fibrillation Among Asian Chronic Hepatitis C Virus Carriers: A Nationwide Population-Based Cohort Study. J. Am. Heart Assoc. 2019, 8, e012914. [Google Scholar] [CrossRef] [PubMed]
- Moss, T.J.; Calland, J.F.; Enfield, K.B.; Gomez-Manjarres, D.C.; Ruminski, C.; DiMarco, J.P.; Lake, D.E.; Moorman, J.R. New-Onset Atrial Fibrillation in the Critically Ill. Crit. Care Med. 2017, 45, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Ambrus, D.B.; Benjamin, E.J.; Bajwa, E.K.; Hibbert, K.A.; Walkey, A.J. Risk factors and outcomes associated with new-onset atrial fibrillation during acute respiratory distress syndrome. J. Crit. Care 2015, 30, 994–997. [Google Scholar] [CrossRef] [Green Version]
- Manjili, R.H.; Zarei, M.; Habibi, M.; Manjili, M.H. COVID-19 as an Acute Inflammatory Disease. J. Immunol. 2020, 205, 12–19. [Google Scholar] [CrossRef]
- Boos, C.J. Infection and atrial fibrillation: Inflammation begets AF. Eur. Heart J. 2020, 41, 1120–1122. [Google Scholar] [CrossRef]
- Heijman, J.; Muna, A.P.; Veleva, T.; Molina, C.E.; Sutanto, H.; Tekook, M.; Wang, Q.; Abu-Taha, I.H.; Gorka, M.; Kunzel, S.; et al. Atrial Myocyte NLRP3/CaMKII Nexus Forms a Substrate for Postoperative Atrial Fibrillation. Circ. Res. 2020, 127, 1036–1055. [Google Scholar] [CrossRef]
- Deng, Q.W.; Huang, S.; Li, S.; Zhai, Q.; Zhang, Q.; Wang, Z.J.; Chen, W.X.; Sun, H.; Lu, M.; Zhou, J. Inflammatory Factors as Potential Markers of Early Neurological Deterioration in Acute Ischemic Stroke Patients Receiving Endovascular Therapy—The AISRNA Study. J. Inflamm. Res. 2021, 14, 4399–4407. [Google Scholar] [CrossRef]
- Ziegler, L.; Wallen, H.; Aspberg, S.; de Faire, U.; Gigante, B. IL6 trans-signaling associates with ischemic stroke but not with atrial fibrillation. BMC Neurol. 2021, 21, 306. [Google Scholar] [CrossRef]
- Ding, W.Y.; Harrison, S.; Gupta, D.; Lip, G.Y.H.; Lane, D.A. Stroke and Bleeding Risk Assessments in Patients With Atrial Fibrillation: Concepts and Controversies. Front. Med. 2020, 7, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, E.; Kiat, H.; McLachlan, C.S. Atrial fibrillation in COVID-19: A review of possible mechanisms. FASEB J. 2020, 34, 11347–11354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, Y.; Wang, X.; Yang, L.; Li, H.; Wang, Y.; Liu, M.; Zhao, X.; Xie, Y.; Yang, Y.; et al. SARS-CoV-2 binds platelet ACE2 to enhance thrombosis in COVID-19. J. Hematol. Oncol. 2020, 13, 120. [Google Scholar] [CrossRef]
- Angeli, F.; Zappa, M.; Reboldi, G.; Trapasso, M.; Cavallini, C.; Spanevello, A.; Verdecchia, P. The pivotal link between ACE2 deficiency and SARS-CoV-2 infection: One year later. Eur. J. Intern. Med. 2021, 93, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Gawalko, M.; Kaplon-Cieslicka, A.; Hohl, M.; Dobrev, D.; Linz, D. COVID-19 associated atrial fibrillation: Incidence, putative mechanisms and potential clinical implications. Int. J. Cardiol. Heart Vasc. 2020, 30, 100631. [Google Scholar] [CrossRef]
- Bautista-Vargas, M.; Bonilla-Abadia, F.; Canas, C.A. Potential role for tissue factor in the pathogenesis of hypercoagulability associated with in COVID-19. J. Thromb. Thrombolysis 2020, 50, 479–483. [Google Scholar] [CrossRef]
- Dorjee, K.; Kim, H.; Bonomo, E.; Dolma, R. Prevalence and predictors of death and severe disease in patients hospitalized due to COVID-19: A comprehensive systematic review and meta-analysis of 77 studies and 38,000 patients. PLoS ONE 2020, 15, e0243191. [Google Scholar] [CrossRef]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [Green Version]
- Genovesi, S.; Rebora, P.; Occhino, G.; Rossi, E.; Maloberti, A.; Belli, M.; Bonfanti, P.; Giannattasio, C.; Rossetti, C.; Epis, O.M.; et al. Atrial Fibrillation and Clinical Outcomes in a Cohort of Hospitalized Patients with Sars-Cov-2 Infection and Chronic Kidney Disease. J. Clin. Med. 2021, 10, 4108. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| New Onset AF (n = 25) | Other AF (n = 22) | No AF (n = 128) | p | |
|---|---|---|---|---|
| Demographics | ||||
| Age, median (IQR) | 81 (73.6–84) | 80.5 (70.8–84) | 71.5 (57.5–83.9) | <0.005 |
| BMI, median (IQR) | 25.4 (22.8–27.7) | 24.1 (21.7–30.6) | 25.1 (22.5–27) | 0.712 |
| Smoking, current, n (%) | 3 (12) | 2 (9) | 21 (16.4) | 0.138 |
| Smoking, past, n (%) | 2 (8) | 3 (13.6) | 10 (7.8) | 0.744 |
| Gender, male, n (%) | 12 (48) | 12 (54.5) | 67 (52.3) | 0.571 |
| Hospital stay (days), median, (IQR) | 12 (5–27) | 22 (13–40.5) | 21 (13–36) | 0.111 |
| Comorbidities | ||||
| Diabetes, n (%) | 5 (20) | 4 (18.1) | 33 (25.7) | 0.629 |
| Coronary artery disease, n (%) | 6 (24) | 6 (27.2) | 21 (16.4) | 0.228 |
| COPD, n (%) | 3 (12) | 4 (18.1) | 12 (9.3) | 0.463 |
| Heart failure, n (%) | 5 (20) | 9 (40.9) | 17 (13.2) | <0.005 |
| Hypertension, n (%) | 16 (64) | 15 (68.1) | 78 (60.9) | 0.139 |
| Chronic kidney disease, n (%) | 11 (44) | 11 (50) | 22 (17.1) | <0.001 |
| Cerebrovascular disease, n (%) | 4 (16) | 5 (22.7) | 29 (22.6) | 0.449 |
| Respiratory failure, n (%) | 1 (4) | 0 (0) | 4 (3) | 0.575 |
| Vital and clinical parameters | ||||
| Heart rate, median (IQR) | 80 (77.5–95) | 80 (72.5–95.5) | 80 (76–90) | 0.068 |
| DBP mmHg, median (IQR) | 70 (60–80) | 70 (66-82) | 70 (60–78) | 0,355 |
| SBP mmHg, median (IQR) | 130 (110–150) | 125 (120–140) | 130 (115–145) | 0.541 |
| MBP mmHg, median (IQR) | 90 (76–103) | 88 (84–99) | 91 (80–102) | 0.402 |
| Respiratory rate, median (IQR) | 23 (18–28) | 19 (18–25) | 18 (17–22) | <0.001 |
| Fever, n (%) | 4 (16) | 6 (22.7) | 56 (43) | <0.05 |
| PaO2/FiO2 ratio, median (IQR) | 286 (147–366) | 320 (197–388) | 309 (214–357) | 0.665 |
| CHA2DS2-VASc, median (IQR) | 3 (2–4) | 3 (2–4) | - | 0.4 |
| HAS-BLED, median (IQR) | 1 (1–2) | 1 (1–2) | - | 0.94 |
| Therapy | ||||
| Corticosteroid, n (%) | 23 (92) | 19 (86) | 109 (85) | 0.66 |
| COT, n (%) | 13 | 10 | 73 | 0.59 |
| HFNO, n (%) | 5 | 5 | 26 | 0.96 |
| c-PAP, n (%) | 6 | 3 | 24 | 0.67 |
| NIMV, n (%) | 1 | 1 | 5 | 0.97 |
| New-Onset AF (n = 25) | Other AF (n = 22) | No AF (n = 128) | p | |
|---|---|---|---|---|
| Laboratory findings | ||||
| Albumin, g/dL | 2.93 (2.7–3.23) | 3 (2.72–3.35) | 3.17 (2.8–3.55) | 0.18 |
| ALT, UI/L | 33 (13–38) | 26 (13–25.5) | 18.5 (13–34) | 0.508 |
| AST, UI/L | 30 (27–50) | 28 (19.25–35.25) | 24 (17–36.5) | 0.660 |
| CK, U/L | 63 (38–126) | 76 (37–324.5) | 103 (46–243.5) | 0.369 |
| Creatinine, mg/dL | 1.5 (0.9–2.3) | 0.9 (0.7–1.5) | 0.9 (0.7–1.2) | 0.005 |
| D-DIMER, mcg/mL | 1.44 (0.48–4) | 1 (0.6–1-6) | 1 (0.485–1.88) | 0.32 |
| Fibrinogen, mg/dL | 503 (320–660) | 476.5 (345–564) | 527 (418–637) | 0.16 |
| Hb, gr/dL | 12.4 (10.7–13.7) | 12.2 (10.5–13.9) | 13 (11–14.5) | 0.142 |
| IL-6, pg/mL | 80.9 (54–130) | 27.5 (12.9–40.4) | 20.3 (8.4–38.8) | 0.001 |
| LDH, U/L | 654 (331–516) | 422,5 (476–806) | 383 (323–533) | 0.478 |
| Lymphocyte count, cells | 816 (600–1503) | 1308 (1143–1576) | 1376.5 (842–1815.5) | 0.173 |
| NT-PRO-BNP, pg/mL | 1939 (488.75–2946) | 1972 (1402–4907) | 196 (75–996) | 0.197 |
| PCR, mg/dL | 6.9 (0.96–13.6) | 2.95 (1.18–6.55) | 3.5 (0.7–7.9) | 0.712 |
| PCT, ng/mL | 0.2 (0.09–0.31) | 0.09 (0.04–0.16) | 0.09 (0.05–0.21) | 0.654 |
| PLT, cells × 104 | 155 (90–172) | 166 (136–242) | 206 (155–252) | 0.017 |
| Troponin, pg/mL | 121 (98–259) | 200 (41–536) | 34.57 (11–137) | 0.616 |
| Urea, mg/dL | 63 (42–108) | 38 (27.25–61.75) | 40.5 (28.25–70) | 0.01 |
| WBC, cells | 9700 (4400–14940) | 6000 (4725–11325) | 6850 (4900–9975) | 0.365 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagnato, G.; Imbalzano, E.; Aragona, C.O.; Ioppolo, C.; Di Micco, P.; La Rosa, D.; Costa, F.; Micari, A.; Tomeo, S.; Zirilli, N.; et al. New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress. Medicina 2022, 58, 530. https://doi.org/10.3390/medicina58040530
Bagnato G, Imbalzano E, Aragona CO, Ioppolo C, Di Micco P, La Rosa D, Costa F, Micari A, Tomeo S, Zirilli N, et al. New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress. Medicina. 2022; 58(4):530. https://doi.org/10.3390/medicina58040530
Chicago/Turabian StyleBagnato, Gianluca, Egidio Imbalzano, Caterina Oriana Aragona, Carmelo Ioppolo, Pierpaolo Di Micco, Daniela La Rosa, Francesco Costa, Antonio Micari, Simona Tomeo, Natalia Zirilli, and et al. 2022. "New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress" Medicina 58, no. 4: 530. https://doi.org/10.3390/medicina58040530