
Comparative Efficacy of Tocilizumab and Baricitinib Administration in COVID-19 Treatment: A Retrospective Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Consent Statement
2.2. Patients
2.3. Data Collection
2.4. Statistical Analysis
3. Results
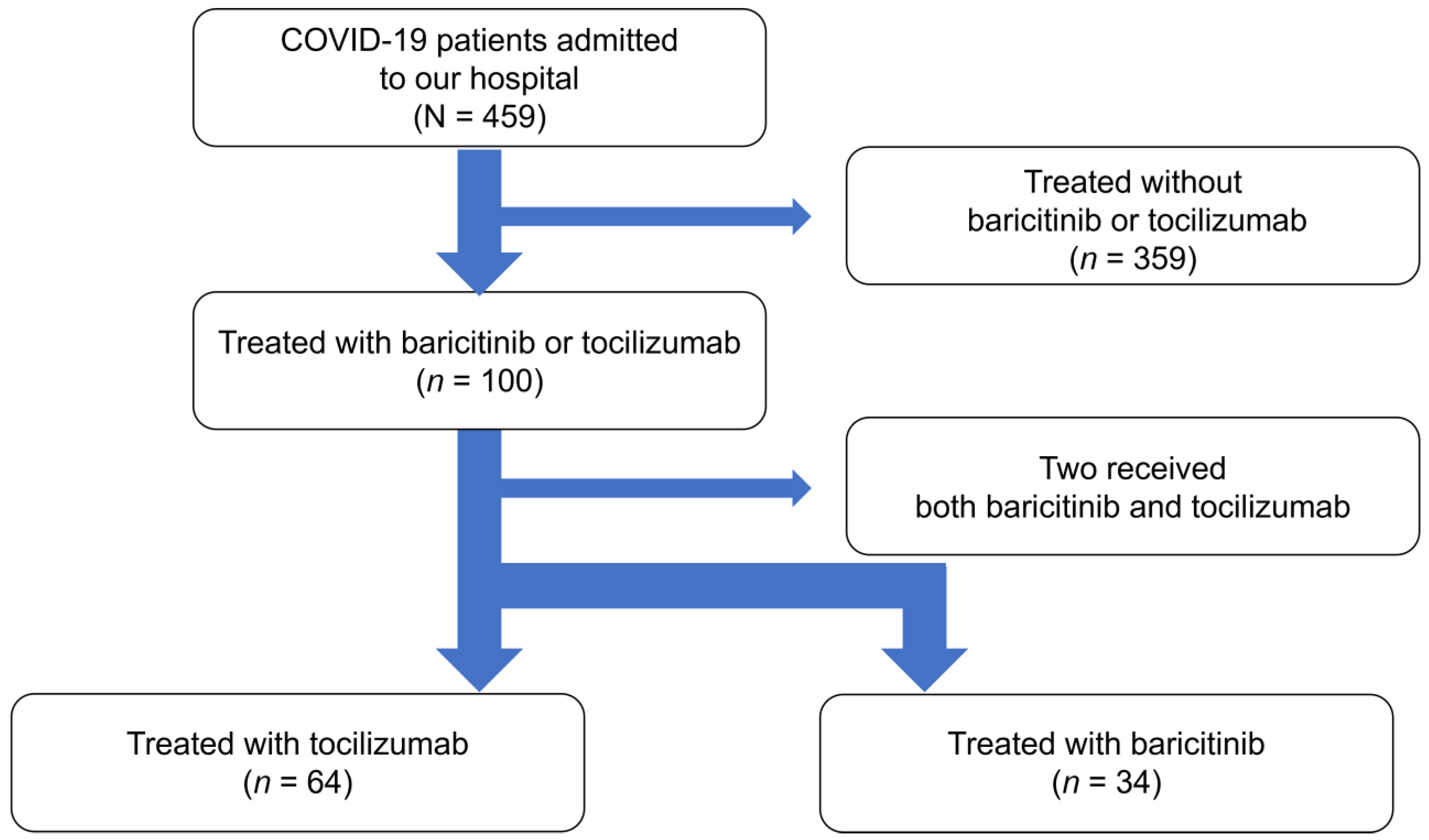
3.1. Study Population
3.2. Baseline Characteristics
3.3. Risk Factors for Death within 28 Days from Initiating TCZ or BRT Treatment
3.4. Factors Contributing to Improvement in Respiratory Status
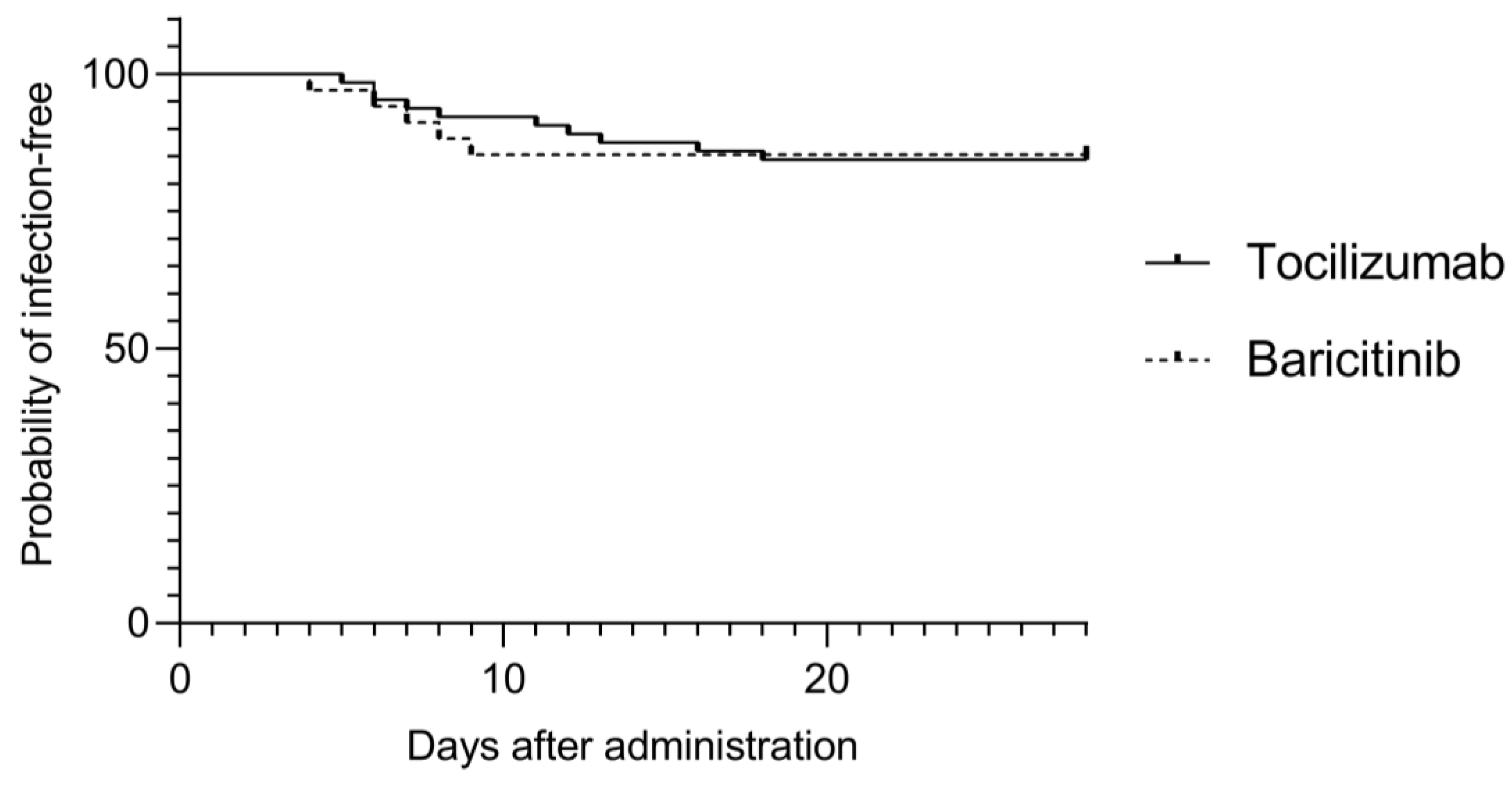
3.5. Development of Secondary Infections
3.6. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; François, B.; Sève, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [PubMed]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: The CoDEX randomized clinical trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Kaly, L.; Rosner, I. Tocilizumab—A novel therapy for non-organ-specific autoimmune diseases. Best Pract. Res. Clin. Rheumatol. 2012, 26, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.J. Correction to: Tocilizumab: A Review in Rheumatoid Arthritis. Drugs 2018, 78, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; van Bentum-Puijk, W.; Berry, Z.; et al. Interleukin-6 receptor antagonists in critically Ill patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [PubMed]
- RECOVERY Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Emery, P.; Durez, P.; Hueber, A.J.; de la Torre, I.; Larsson, E.; Holzkämper, T.; Tanaka, Y. Baricitinib inhibits structural joint damage progression in patients with rheumatoid arthritis-a comprehensive review. Arthritis Res. Ther. 2021, 23, 3. [Google Scholar] [CrossRef] [PubMed]
- Jamilloux, Y.; El Jammal, T.; Vuitton, L.; Gerfaud-Valentin, M.; Kerever, S.; Sève, P. JAK inhibitors for the treatment of autoimmune and inflammatory diseases. Autoimmun. Rev. 2019, 18, 102390. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus remdesivir for hospitalized adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R.; et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir. Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Infectious Diseases Society of America 2021; Version 5.6.0. COVID-19 Guideline, Part 1: Treatment and Management. 2021. Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/ (accessed on 1 February 2021).
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 1 February 2021).
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda, A.; Suzuki, K.; Endo, M.; et al. Clinical epidemiology of hospitalized patients with COVID-19 in Japan: Report of the COVID-19 registry Japan. Clin. Infect. Dis. 2021, 73, e3677–e3689. [Google Scholar] [CrossRef] [PubMed]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Cameron, C.; Noorbaloochi, S.; Cullis, T.; Tucker, M.; Christensen, R.; Ghogomu, E.T.; Coyle, D.; Clifford, T.; Tugwell, P.; et al. Risk of serious infection in biological treatment of patients with rheumatoid arthritis: A systematic review and meta-analysis. Lancet 2015, 386, 258–265. [Google Scholar] [CrossRef] [Green Version]
- Badr, M.; De Oliveira, B.; Abdallah, K.; Nadeem, A.; Varghese, Y.; Munde, D.; Salam, S.; Abduljawad, B.; Saleh, K.; Elkambergy, H.; et al. Effects of methylprednisolone on ventilator-free days in mechanically ventilated patients with acute respiratory distress syndrome and COVID-19: A retrospective study. J. Clin. Med. 2021, 10, 760. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the treatment of COVID-19—Final report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium; Pan, H.; Peto, R.; Henao-Restrepo, A.M.; Preziosi, M.P.; Sathiyamoorthy, V.; Karim, Q.A.; Alejandria, M.M.; García, C.H.; Kieny, M.P.; et al. Repurposed antiviral drugs for Covid-19—Interim WHO solidarity trial results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomized, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 98) | Tocilizumab (n = 64) | Baricitinib (n = 34) | p-Value | |
|---|---|---|---|---|
| Characteristics | ||||
| Age (years) | 60.5 (54.0, 70.3) | 65.5 (54.3, 72.8) | 58.5 (53.8, 64.3) | 0.03 |
| Sex (male) | 73 (74.5) | 46 (71.9) | 27 (79.4) | 0.42 |
| Current smoker | 16 (16.3) | 9 (16.5) | 7 (20.6) | 0.41 |
| BMI ≥ 30 (kg/m2) * | 25 (27.2) | 18 (30.0) | 7 (20.6) | 0.40 |
| Chronic heart disease | 17 (17.4) | 15 (23.4) | 2 (5.9) | 0.03 |
| Chronic kidney disease | 6 (6.1) | 4 (6.3) | 2 (5.9) | 0.94 |
| Diabetes mellitus | 36 (36.7) | 23 (35.9) | 13 (38.2) | 0.82 |
| Any collagen disease | 3 (3.1) | 3 (4.7) | 0 (0) | 0.20 |
| Hypertension | 46 (46.9) | 34 (53.1) | 12 (35.3) | 0.09 |
| Any respiratory disease | 8 (8.1) | 6 (9.4) | 2 (5.9) | 0.55 |
| Immunosuppressive Drug regular use | 3 (3.1) | 2(3.1) | 1 (2.9) | 0.96 |
| Fully vaccinated | 1 (1.0) | 0 (0) | 1 (1.0) | 0.14 |
| Time from symptom onset to administration | 9 (7, 12) | 10 (7, 13) | 9 (7, 11) | 0.50 |
| Time from onset to administration ≤ 7 days | 29 (29.6) | 19 (29.7) | 10 (29.4) | 0.98 |
| Treatment | ||||
| Steroid | 96 (98.0) | 63 (98.4) | 33 (97.1) | 0.65 |
| Heparin | 78 (79.6) | 55 (86.0) | 23 (67.7) | 0.03 |
| Any anti-viral drug | 75 (76.5) | 45 (70.3) | 30 (88.2) | 0.046 |
| Antibody cocktail therapy | 1 (1.0) | 0 (0) | 1 (1.0) | 0.14 |
| Blood test at administration | ||||
| White blood cell (/μL) | 7900 (5550, 10825) | 8000 (5400, 11075) | 7700 (5600, 10525) | 0.64 |
| Neutrophils (/μL) ** | 6991 (4465, 9755) | 7173 (4716, 10027) | 6780 (4418, 9280) | 0.53 |
| Lymphocytes (/μL) ** | 611 (476, 908) | 648 (440, 911) | 608 (528, 852) | 0.65 |
| Eosinophil (/μL) ** | 0 (0, 0) | 0 (0, 0) | 0 (0, 8.3) | 0.047 |
| Hemoglobin (g/dL) | 14.2 (12.9, 15.0) | 13.8 (12.8, 15.0) | 14.5 (13.9, 15.6) | 0.04 |
| Platelet (×104/μL) | 19.0 (13.4, 25.9) | 18.5 (12.7, 25.8) | 20.7 (14.8, 26.4) | 0.51 |
| LDH (U/L) | 512.5 (419.8, 647.5) | 540 (438.8, 716.0) | 470.5 (386.5, 603.5) | 0.02 |
| CRP (mg/mL) | 7.1 (3.6, 11.2) | 7.8 (3.9, 12.1) | 5.8 (3.1, 9.4) | 0.12 |
| KL-6 (U/mL) *** | 402 (289.5, 617.5) | 444 (337, 705) | 319 (240.3, 481.5) | 0.03 |
| Procalcitonin (ng/mL) **** | 0.08 (0.05, 0.15) | 0.08 (0.06, 0.12) | 0.08 (0.05, 0.18) | 0.97 |
| Ferritin (ng/mL) ***** | 1125.5 (693.8, 1924.5) | 1242.5 (745.3, 1966.3) | 1080 (631.8, 1901) | 0.44 |
| D-dimer (μg/mL) ****** | 1.4 (1.0, 2.5) | 1.5 (1.3, 3.1) | 1.0 (0.8, 1.4) | <0.001 |
| Severity | ||||
| 1 | 1 (1) | 1 (1.6) | 0 (0) | |
| 2 | 9 (9.2) | 4 (6.3) | 5 (14.7) | |
| 3 | 76 (77.6) | 49 (76.6) | 27 (79.4) | |
| 4 | 12 (12.2) | 10 (15.6) | 2 (5.9) | 0.26 |
| Outcomes | ||||
| Death within 28 days | 14 (14.3) | 13 (20.3) | 1 (2.94) | |
| Improvement in respiratory status within 28 days | 73 (74.5) | 43 (67.2) | 33 (88.2) | |
| Development of secondary infections | 15 (15.3) | 10 (15.6) | 5 (14.7) | |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Characteristic | ||||
| Tocilizumab use * | 8.41 (1.05–67.37) | 0.045 | 13.28 (0.45–392.92) | 0.13 |
| Age (year) | 1.10 (1.03–1.18) | 0.004 | 1.10 (1.00–1.21) | 0.04 |
| Sex (male) | 0.38 (0.12–1.26) | 0.12 | ||
| Current smoker | 0.35 (0.04–2.92) | 0.33 | ||
| BMI ≥ 30 (kg/m2) | 0.94 (0.27–3.30) | 0.93 | ||
| Chronic heart disease | 2.18 (0.59–8.03) | 0.24 | ||
| Chronic kidney disease | 16.40 (2.66–101.21) | 0.003 | 43.10 (2.71–686.04) | 0.008 |
| Diabetes mellitus | 1.35 (0.43–4.26) | 0.61 | ||
| Any collagen disease | 3.15 (0.27–37.31) | 0.36 | ||
| Hypertension | 2.29 (0.70–7.40) | 0.17 | ||
| Any respiratory disease | 4.31 (0.90–20.59) | 0.07 | 1.85 (0.22–15.76) | 0.57 |
| Immunosuppressive drug regular use | 3.15 (0.27–37.31) | 0.36 | ||
| Time from onset to administration ≤ 7 days | 5.76 (1.73–19.18) | 0.004 | 18.09 (1.70–192.47) | 0.02 |
| Treatment | ||||
| Heparin | 1.64 (0.34–7.98) | 0.54 | ||
| Any anti-viral drug | 0.34 (0.10–1.11) | 0.07 | 0.16 (0.01–1.96) | 0.15 |
| Blood test at administration | ||||
| Lymphocytes (×103/μL) | 0.36 (0.01–13.81) | 0.58 | ||
| Platelet (×105/μL) | 0.66 (0.35–1.24) | 0.20 | ||
| LDH (×102 U/L) | 1.18 (0.88–1.59) | 0.27 | ||
| CRP (mg/mL) | 1.02 (0.92–1.13) | 0.68 | ||
| KL–6 (×102 U/mL) | 1.06 (0.87–1.30) | 0.57 | ||
| Procalcitonin (ng/mL) | 1.36 (0.18–9.97) | 0.76 | ||
| Ferritin (×103 ng/mL) | 0.37 (0.10–1.47) | 0.16 | ||
| D-dimer (μg/mL) | 0.10 (0.96–1.03) | 0.82 | ||
| Severity | ||||
| 1 or 2 | (reference) | (reference) | ||
| 3 | 1.52 (0.18–13.24) | 0.70 | ||
| 4 | 1.80 (0.14–23.37) | 0.65 | ||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Characteristics | ||||
| Baricitinib use * | 3.66 (1.14–11.76) | 0.03 | 1.75 (0.35–8.67) | 0.50 |
| Age (year) | 0.94 (0.89–0.98) | 0.004 | 0.94 (0.88–1.01) | 0.07 |
| Sex (male) | 1.55 (0.57–4.22) | 0.39 | ||
| Current smoker | 6.21 (0.78–49.65) | 0.09 | 4.14 (0.28–60.37) | 0.29 |
| BMI ≥ 30 (kg/m2) | 1.46 (0.47–4.49) | 0.50 | ||
| Chronic heart disease | 0.27 (0.09–0.80) | 0.03 | 0.40 (0.09–1.89) | 0.25 |
| Chronic kidney disease | 0.15 (0.03–0.86) | 0.03 | 0.12 (0.01–1.80) | 0.13 |
| Diabetes mellitus | 1.04 (0.40–2.68) | 0.93 | ||
| Any collagen disease | 0.68 (0.07–9.12) | 0.75 | ||
| Hypertension | 0.39 (0.15–1.01) | 0.047 | 0.84 (0.20–3.59) | 0.82 |
| Any respiratory disease | 0.54 (0.12–2.44) | 0.42 | ||
| Immunosuppressive drug regular use | 0.67 (0.05–7.79) | 0.75 | ||
| Time from onset to administration ≤ 7 days | 0.26 (0.10–0.68) | 0.006 | 0.82 (0.02–0.40) | 0.002 |
| Treatment | ||||
| Heparin | 0.97 (0.31–3.00) | 0.95 | ||
| Any anti-viral drug | 3.99 (1.46–10.89) | 0.007 | 6.5 (1.13–37.56) | 0.04 |
| Blood test at administration | ||||
| Lymphocytes (×103/μL) | 1.07 (0.92–1.24) | 0.37 | ||
| Platelet (×105/μL) | 1.37 (0.84–2.24) | 0.20 | ||
| LDH (×102 U/L) | 0.85 (0.66–1.09) | 0.19 | ||
| CRP (mg/mL) | 1.01 (0.92–1.09) | 0.91 | ||
| KL–6 (×102 U/mL) | 0.91 (0.78–1.06) | 0.25 | ||
| Procalcitonin (ng/mL) | 1.08 (0.13–12.74) | 0.83 | ||
| Ferritin (ng/mL) | 1.15 (0.65–2.03) | 0.64 | ||
| D–dimer (μg/mL) | 0.98 (0.95–1.00) | 0.09 | 0.98 (0.96–1.01) | 0.25 |
| Severity | ||||
| 1 or 2 | (reference) | (reference) | (reference) | (reference) |
| 3 | 0.36 (0.04–3.02) | 0.35 | ||
| 4 | 0.11 (0.01–1.17) | 0.07 | 0.04 (0.002–1.01) | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kojima, Y.; Nakakubo, S.; Takei, N.; Kamada, K.; Yamashita, Y.; Nakamura, J.; Matsumoto, M.; Horii, H.; Sato, K.; Shima, H.; et al. Comparative Efficacy of Tocilizumab and Baricitinib Administration in COVID-19 Treatment: A Retrospective Cohort Study. Medicina 2022, 58, 513. https://doi.org/10.3390/medicina58040513
Kojima Y, Nakakubo S, Takei N, Kamada K, Yamashita Y, Nakamura J, Matsumoto M, Horii H, Sato K, Shima H, et al. Comparative Efficacy of Tocilizumab and Baricitinib Administration in COVID-19 Treatment: A Retrospective Cohort Study. Medicina. 2022; 58(4):513. https://doi.org/10.3390/medicina58040513
Chicago/Turabian StyleKojima, Yuichi, Sho Nakakubo, Nozomu Takei, Keisuke Kamada, Yu Yamashita, Junichi Nakamura, Munehiro Matsumoto, Hiroshi Horii, Kazuki Sato, Hideki Shima, and et al. 2022. "Comparative Efficacy of Tocilizumab and Baricitinib Administration in COVID-19 Treatment: A Retrospective Cohort Study" Medicina 58, no. 4: 513. https://doi.org/10.3390/medicina58040513