
A New Treatment Algorithm That Incorporates Minimally Invasive Surgery for Pyogenic Spondylodiscitis in the Thoracic and Lumbar Spines: The Results of Its Clinical Application to a Series of 34 Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Presentation
2.3. Diagnostic Workup
2.4. Algorithmic Treatment Selections
2.5. Conservative Treatment
2.6. Surgical Treatment
2.6.1. Isolated PPS–Rod Fixation
2.6.2. PPS–Rod Fixation + Posterior Decompression and Debridement + Surgical Sampling
2.6.3. LLIF Procedure for Anterior Debridement with Iliac Bone Grafting
2.7. Statistical Analysis
3. Results
3.1. Algorithmic Treatment Selections in 34 Consecutive Patients
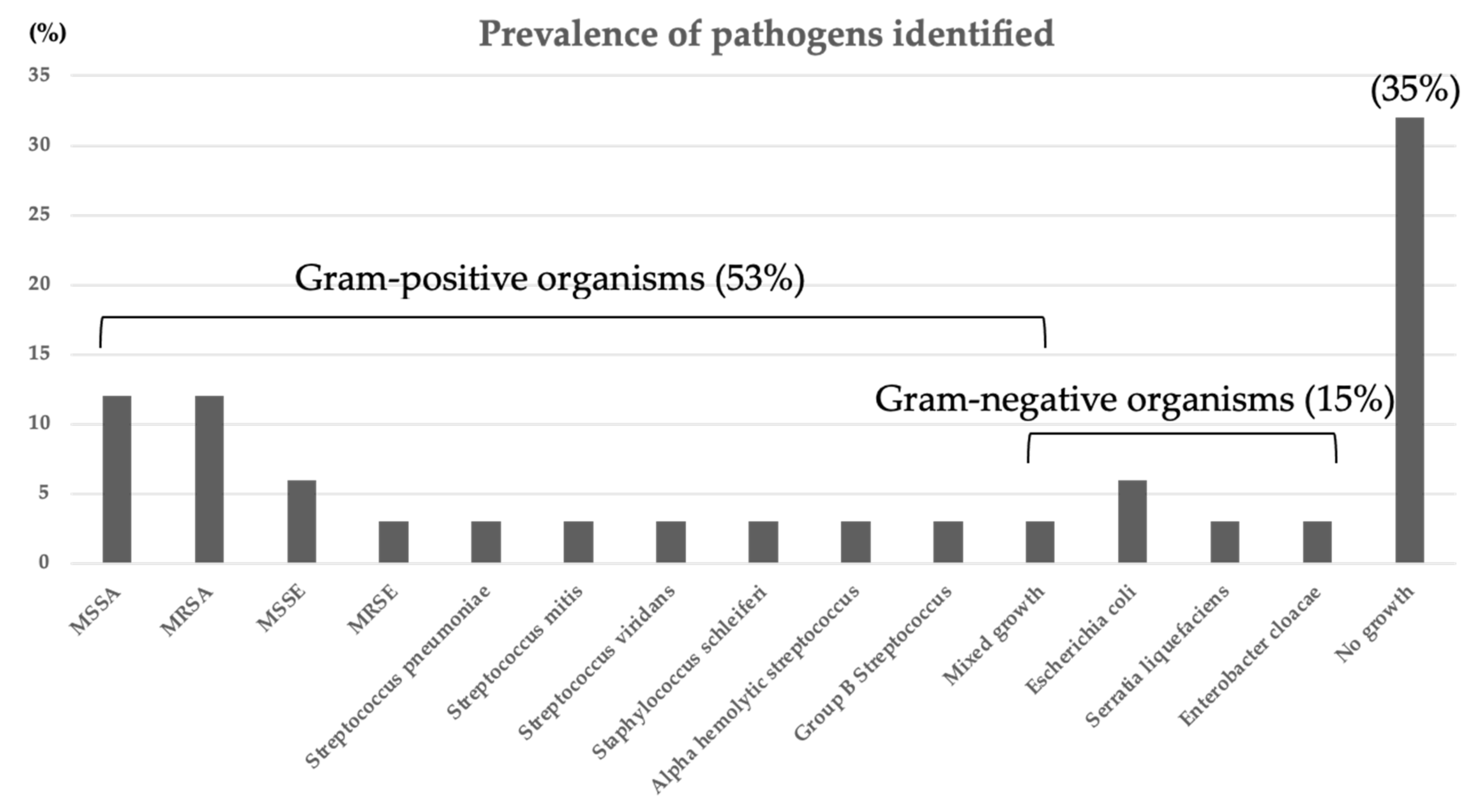
3.2. Bacteriology Results
3.3. Risk Factors That Necessitated More Complicated Treatment Options
3.4. Follow up and Outcomes
3.4.1. Follow Up
3.4.2. Clinical, Laboratory, and Radiologic Imaging Results
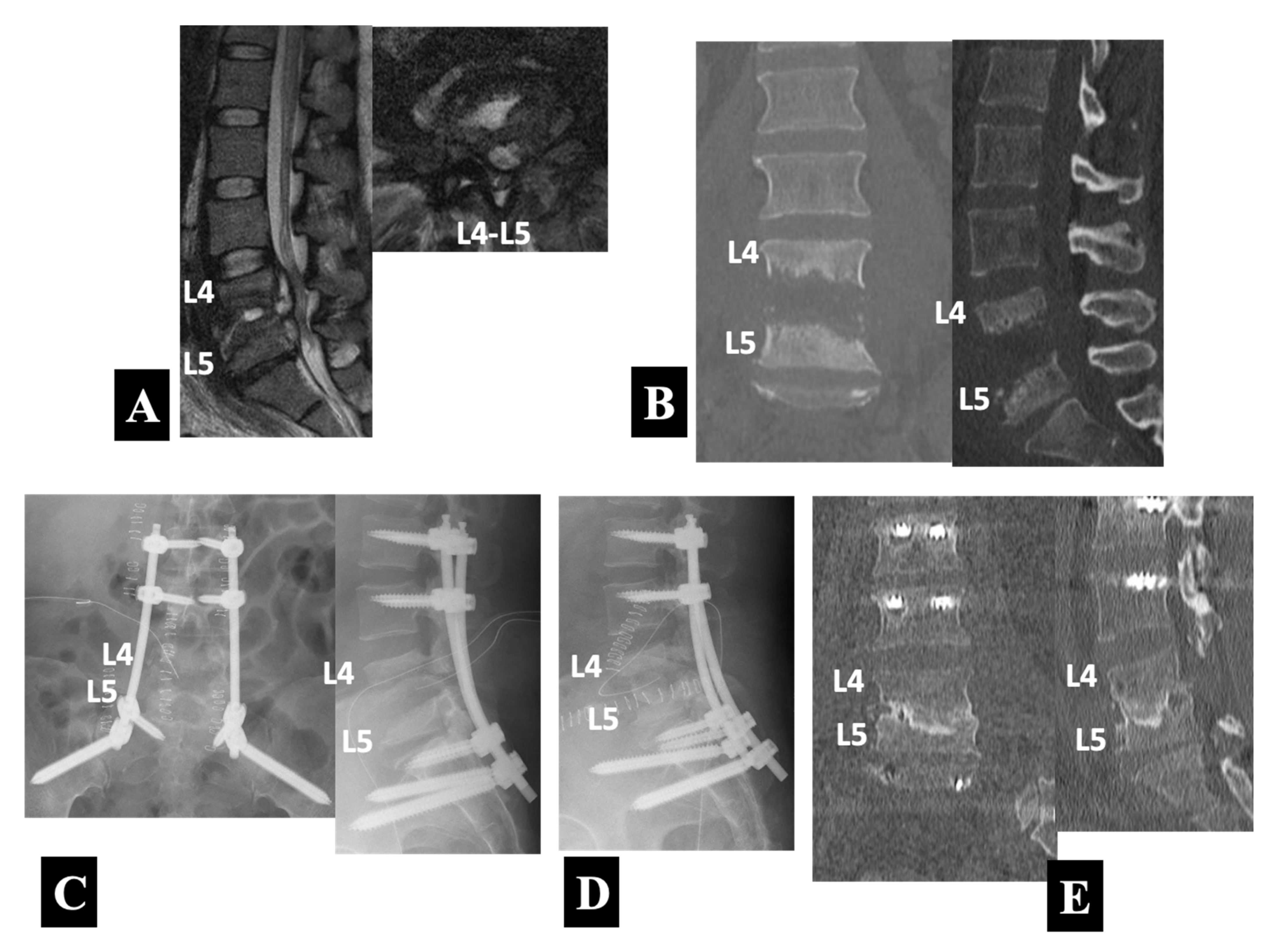
3.5. Case Presentation
- Case 1 in Group 1-B (Figure 3):
- Case 2 in Group 2-A (Figure 4):
- Case 3 in Group 2-B (Figure 5):
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krogsgaard, M.R.; Wagn, P.; Bengtsson, J. Epidemiology of acute vertebral osteomyelitis in Denmark: 137 cases in Denmark 1978–1982, compared to cases reported to the National patient register 1991–1993. Acta Orthop. Scand. 1998, 69, 513–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHenry, M.C.; Easley, K.A.; Locker, G.A. Vertebral osteomyelitis: Long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin. Infect. Dis. 2002, 34, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.S.; Shelly, M.J.; Timlin, M.; Powderly, W.G.; O’Byrne, J.M. Nontuberculous pyogenic spinal infection in adults: A 12-year experience from a tertiary referral center. Spine 2006, 31, 2695–2700. [Google Scholar] [CrossRef] [PubMed]
- Emery, S.E.; Gocke, R.T. Spinal infection/Osteomyelitis. In The Textbook of Spinal Surgery, 3rd ed.; Bridwell, K.H., DeWald, R.L., Eds.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; Volume 2, pp. 1553–1559. [Google Scholar]
- Foley, K.T.; Gupta, S.K.; Justis, J.R.; Sherman, M.C. Percutaneous screw fixation of the lumbar spine. Neurosurg. Focus 2001, 10, E10. [Google Scholar] [CrossRef]
- Bergey, D.L.; Villavicencio, A.T.; Goldstein, T.; Regan, J.J. Endoscopic lateral transpsoas approach to the lumbar spine. Spine 2004, 29, 1681–1688. [Google Scholar] [CrossRef]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme lateral interbody fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef]
- Deininger, M.H.; Unfried, M.I.; Vougioukas, V.I.; Hubbe, U. Minimally invasive dorsal percutaneous spondylodesis for the treatment of adult pyogenic spondylodiscitis. Acta Neurochir. 2009, 151, 1451–1457. [Google Scholar] [CrossRef]
- Ha, K.Y.; Kim, Y.H.; Seo, J.Y.; Bae, S.H. Percutaneous posterior instrumentation followed by direct lateral interbody fusion for lumbar infectious spondylitis. J. Spinal Disord. Tech. 2013, 26, E95–E100. [Google Scholar] [CrossRef]
- Nasto, L.A.; Colangelo, D.; Mazzotta, V.; Meco, E.D.; Neri, V.; Nasto, R.A.; Fantoni, M.; Pola, E. Is posterior percutaneous screw-rod instrumentation a safe and effective alternative approach to TLSO rigid bracing for single-level pyogenic spondylodiscitis? Results of a retrospective cohort analysis. Spine J. 2014, 14, 1139–1146. [Google Scholar] [CrossRef]
- Lin, Y.; Ki, F.; Chen, W.; Zeng, H.; Chen, A.; Xiong, W. Single-level lumbar pyogenic spondylodiscitis treated with mini-open anterior debridement and fusion in combination with posterior percutaneous fixation via a modified anterior lumbar interbody fusion approach. J. Neurosug. Spine 2015, 23, 747–753. [Google Scholar] [CrossRef] [Green Version]
- Viezens, L.; Schaefer, C.; Helmers, R.; Vettorazzi, E.; Schroeder, M.; Hansen-Algenstaedt, N. Spontaneous pyogenic spondylodiscitis in the thoracic or lumbar spine: A retrospective cohort study comparing the safety and efficacy of minimally invasive and open surgery over a nine-year period. World Neurosurg. 2017, 102, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Alaid, A.; Von Eckardstein, K.; Smoll, N.R.; Solomiichuk, V.; Rohde, V.; Martinez, R.; Ascatlo, B. Robot guidance for percutaneous minimally invasive placement of pedicle screws for pyogenic spondylodiscitis is associated with lower rates of wound breakdown compared to conventional fluoroscopy-guided instrumentation. Neurosurg. Rev. 2018, 41, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Farah, K.; Peyiere, H.; Graillon, T.; Prost, S.; Dufour, H.; Blondel, B.; Fuentes, S. Minimally invasive posterior fixation and anterior debridement-fusion for thoracolumbar spondylodiscitis: A 40-case series and review of the literature. Neurochirugie 2020, 66, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, T.; Maruo, K.; Arizumi, F.; Kusuyama, K.; Kishima, K. Interbody fusion with cages for pyogenic vertebral osteomyelitis. J. Clin. Neurosci. 2020, 77, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Nojiri, H.; Okuda, T.; Miyagawa, K.; Kobayashi, N.; Sato, T.; Hara, T.; Ohara, Y.; Kaneko, K. Anterior spinal fusion autologous bone grafting via the lateral approach with posterior short-range instrumentation for lumbar pyogenic spondylitis with vertebral bone destruction enables early ambulation and prevents spinal deformity. Spine Surg. Relat. Res. 2020, 4, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Duan, K.; Ye, J.; Zhang, W.; Hu, X.; Zhou, J.; Gao, L.; Tang, Y. Percutaneous endoscopic debridement with percutaneous pedicle screw fixation for lumbar pyogenic spondylodiscitis: A preliminary study. Int. Orthop. 2020, 44, 495–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.K.; Jörger, A.-K.; Barz, M.; Sarkar, C.; Wostrack, M.; Meyer, B. Minimally invasive posterior pedicle screw fixation versus open instrumentation in patients with thoracolumbar spondylodiscitis. Acta Neurochir. 2021, 163, 1553–1560. [Google Scholar] [CrossRef]
- Madhavan, K.; Vanni, S.; Williams, S.K. Direct lateral retroperitoneal approach for the surgical treatment of lumbar discitis and osteomyelitis. Neurosurg. Focus 2014, 37, E5. [Google Scholar] [CrossRef]
- Ghobrial, G.M.; Al-Saiegh, F.; Franco, D.; Benito, D.; Heller, J. Lateral lumbar r etroperitoneal transpsoas approach in the setting of spondylodiscitis: A technical note. J. Clin. Neurosci. 2017, 39, 193–198. [Google Scholar] [CrossRef]
- Patel, N.B.; Dodd, Z.H.; Voorhies, J.; Horn, E.M. Minimally invasive lateral transpsoas approach for spinal discitis and osteomyelitis. J. Clin. Neurosci. 2015, 22, 1753–1757. [Google Scholar] [CrossRef]
- Fushimi, K.; Miyamoto, K.; Fukuta, S.; Hosoe, H.; Masuda, T.; Shimizu, K. The surgical treatment of pyogenic spondylitis using posterior instrumentation without anterior debridement. J. Bone Jt. Surg. Br. 2012, 94, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Fraimow, H.S. Systemic antimicrobial therapy in osteomyelitis. Semin. Plast. Surg. 2009, 23, 90–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tani, Y.; Saito, T.; Taniguchi, S.; Ishihara, M.; Paku, M.; Adachi, T.; Ando, M. A new technique useful for lumbosacral percutaneous pedicle screw placement without fluoroscopy or computer-aided navigation systems. J. Orthop. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tani, Y.; Saito, T.; Taniguchi, S.; Ishihara, M.; Paku, M.; Adachi, T.; Ando, M.; Kohara, N.; Kimura, J. Threshold-based monitoring of compound muscle action potentials for percutaneous pedicle screw placement in the lumbosacral spine: Can we rely on stimulation of the uninsulated screw to provide a valid safety warning? Spine 2021. [Google Scholar] [CrossRef]
- Otomo, N.; Funao, H.; Yamanouchi, K.; Isogai, N.; Ishii, K. Computed tomography-based navigation system in current spine surgery: A narrative review. Medicina 2022, 58, 241. [Google Scholar] [CrossRef]
- Fokter, S.K.; Rečnik, G. The use of porous tantalum cages in the treatment of unremitting spondylodiscitis: A case report. Slov. Med. J. 2018, 87, 41–48. [Google Scholar] [CrossRef]
- Berbari, E.F.; Kanji, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M.; Petemann, G.W.; et al. 2015 infectious disease society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin. Infect. Dis. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.C.; Merritt, K. Infection at the site of implanted materials with and without preadhered bacteria. J. Orthop. Res. 1994, 2, 526–531. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Orthopaedic biofilm infections. APMIS 2017, 125, 353–364. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.W.; Currier, B.L.; Heller, J.G.; Eismont, F.J. Cervical spinal infections. In The Cervical Spine, 5th ed.; Benzel, E.C., Ed.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 782–808. [Google Scholar]
- Lau, D.; Chou, D. Minimally invasive instrumentation without fusion during posterior thoracic corpectomies: A comparison of percutaneouly instrumented nonfused segments with open instrumented fused segments. J. Neurosurg. Spine 2017, 27, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, K.; Uchino, K.; Watanabe, S.; Misaki, K.; Iba, H. Effect of minimally invasive spine stabilization in metastatic spinal tumors. Medicina 2022, 58, 358. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tani, Y.; Saito, T.; Taniguchi, S.; Ishihara, M.; Paku, M.; Adachi, T.; Ando, M.; Kotani, Y. A New Treatment Algorithm That Incorporates Minimally Invasive Surgery for Pyogenic Spondylodiscitis in the Thoracic and Lumbar Spines: The Results of Its Clinical Application to a Series of 34 Patients. Medicina 2022, 58, 478. https://doi.org/10.3390/medicina58040478
Tani Y, Saito T, Taniguchi S, Ishihara M, Paku M, Adachi T, Ando M, Kotani Y. A New Treatment Algorithm That Incorporates Minimally Invasive Surgery for Pyogenic Spondylodiscitis in the Thoracic and Lumbar Spines: The Results of Its Clinical Application to a Series of 34 Patients. Medicina. 2022; 58(4):478. https://doi.org/10.3390/medicina58040478
Chicago/Turabian StyleTani, Yoichi, Takanori Saito, Shinichiro Taniguchi, Masayuki Ishihara, Masaaki Paku, Takashi Adachi, Muneharu Ando, and Yoshihisa Kotani. 2022. "A New Treatment Algorithm That Incorporates Minimally Invasive Surgery for Pyogenic Spondylodiscitis in the Thoracic and Lumbar Spines: The Results of Its Clinical Application to a Series of 34 Patients" Medicina 58, no. 4: 478. https://doi.org/10.3390/medicina58040478