
Does the Change in the Diagnostic Criteria for Gestational Diabetes in Poland Affect Maternal and Fetal Complications? A Prospective Study


Abstract
:1. Introduction
- -
- diabetes mellitus during pregnancy—a disorder which meets the general criteria for diabetes mellitus already at diagnosis
- -
- gestational diabetes mellitus—it is mostly manifested during the second or third trimester of pregnancy and meets the specific criteria for the pregnancy period.
- -
- fasting blood glucose ≥ 126 mg/dL (7 mmol/L) or
- -
- 2-h plasma glucose ≥ 200 mg/dL (11.1 mmol/L) following a 75 g oral glucose load or
- -
- random plasma glucose ≥ 200 mg/dL (11.1 mmol/L) in the presence of diabetes symptoms.
- -
- fasting blood glucose 92–125 mg/dL (5.1–6.9 mmol/L) or
- -
- 1-h plasma glucose ≥ 180 mg/dL (10.0 mmol/L) following a 75 g oral glucose load or
- -
- 2-h plasma glucose 153–199 mg/dL (8.5–11.0 mmol/L) following a 75 g oral glucose load.
2. Objective of Study
3. Patients and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiefari, E.; Arcidiacono, B.; Foti, D.; Brunetti, A. Gestational diabetes mellitus: An updated overview. J. Endocrinol. Investig. 2017, 40, 899–909. [Google Scholar] [CrossRef]
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat. Rev. Dis. Primers 2019, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarry-Adkins, J.L.; Aiken, C.E.; Ozanne, S.E. Neonatal, infant, and childhood growth following metformin versus insulin treatment for gestational diabetes: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002848. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Zhang, C. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: A Global Perspective. Curr. Diab. Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Polish Gynecological Society. Polish Gynecological Society’s recommendations regarding pregnant women with diabetes mellitus. Ginekol. Pol. 2005, 76, 936–948. (In Polish) [Google Scholar]
- Li-Zhen, L.; Yun, X.; Xiao-Dong, Z. Evaluation of guidelines on the screening and diagnosis of gestational diabetes mellitus: Systematic review. BMJ Open 2019, 9, e023014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araszkiewicz, A.; Bandurska-Stankiewicz, E.; Borys, S.; Budzyński, A.; Cyganek, K.; Cypryk, K.; Czech, A.; Czupryniak, L.; Drzewoski, J.; Dzida, G.; et al. 2021 Guidelines on the management of patients with diabetes. A position of Diabetes Poland. Clin. Diabetol. 2021, 10, 1–113. [Google Scholar] [CrossRef]
- Coustan, D.R.; Lowe, L.P.; Metzger, B.E.; Dyer, A.R. International Association of Diabetes and Pregnancy Study Groups. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study: Paving the way for new diagnostic criteria for gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2010, 202, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S.; Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahavandi, S.; Seah, J.M.; Shub, A.; Houlihan, C.; Ekinci, E.I. Biomarkers for Macrosomia Prediction in Pregnancies Affected by Diabetes. Front. Endocrinol. 2018, 9, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikawa, T.; Ono, K.; Hashimoto, S.; Kinoshita, H.; Watanabe, T.; Araki, H.; Otsu, K.; Sakamoto, W.; Harada, M.; Toyonaga, T.; et al. One-hour oral glucose tolerance test plasma glucose at gestational diabetes diagnosis is a common predictor of the need for insulin therapy in pregnancy and postpartum impaired glucose tolerance. J. Diabetes Investig. 2018, 9, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Benhalima, K.; Jegers, K.; Devlieger, R.; Verhaeghe, J.; Mathieu, C. Glucose Intolerance after a Recent History of Gestational Diabetes Based on the 2013 WHO Criteria. PLoS ONE 2016, 11, e0157272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyce, B.L.; Dolinsky, V.W. Maternal β-Cell Adaptations in Pregnancy and Placental Signalling: Implications for Gestational Diabetes. Int. J. Mol. Sci. 2018, 19, 3467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boney, C.M.; Verma, A.; Tucker, R.; Vohr, B.R. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005, 115, e290–e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louvigne, M.; Rouleau, S.; Caldagues, E. Association of maternal nutrition with transient neonatal hyperinsulinism. PLoS ONE 2018, 13, e0195383. [Google Scholar] [CrossRef] [PubMed]
- Stanley, C.A. Hypoglycemia in the neonate. Pediatr. Endocrinol. Rev. 2006, 1, 76–81. [Google Scholar]
- Bishop, K.C.; Harris, B.S.; Boyd, B.K. Pharmacologic Treatment of Diabetes in Pregnancy. Obstet. Gynecol. Surv. 2019, 74, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Immanuel, J.; Simmons, D. Screening and Treatment for Early-Onset Gestational Diabetes Mellitus: A Systematic Review and Meta-analysis. Curr. Diabetes Rep. 2017, 17, 115. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | GDM in Group-15/16 (n = 58) | GDM in Group-17/18 (n = 65) | p | ||||
|---|---|---|---|---|---|---|---|
| Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| Body weight before pregnancy, kg | 77.00 | 59.50 | 82.85 | 64.10 | 57.00 | 88.00 | 0.6974 |
| Height, cm | 165.00 | 160.00 | 170.00 | 165.00 | 160.00 | 170.00 | 0.9574 |
| BMI, kg/m2 | 26.821 | 21.57 | 31.06 | 24.53 | 21.25 | 30.11 | 0.5900 |
| Age, years | 30.00 | 27.00 | 34.00 | 31.00 | 27.00 | 34.00 | 0.3750 |
| Body weight gain during pregnancy, kg | 10.00 | 6.00 | 15.00 | 9.50 | 6.00 | 14.50 | 0.9505 |
| Week in which GDM was diagnosed | 26.00 | 23.00 | 27.00 | 26.00 | 20.00 | 28.00 | 0.5397 |
| Week in which insulin was started | 30.00 | 27.00 | 33.00 | 27.00 | 19.00 | 31.00 | 0.0663 |
| Week of delivery | 39.00 | 37.00 | 40.00 | 39.00 | 36.00 | 40.00 | 0.5880 |
| Neonatal body weight at delivery, g | 3330.00 | 2810.00 | 3650.00 | 3250.00 | 2920.00 | 3500.00 | 0.7619 |
| Neonatal body length at delivery, cm | 53.00 | 52.000 | 56.00 | 54.00 | 52.00 | 56.00 | 0.9783 |
| Apgar score at 1 min | 10.00 | 9.00 | 10.00 | 10.00 | 9.000 | 10.00 | 0.7869 |
| Oder of Pregnancy | GDM in Group-15/16 | GDM in Group-17/18 | p | ||
|---|---|---|---|---|---|
| 1 | 34 | 58.62% | 36 | 55.38% | 0.4197 |
| 2 | 15 | 25.86% | 16 | 24.62% | |
| 3 and the following pregnancies | 9 | 15.52% | 13 | 20.00% | |
| Total | 58 | 65 | |||
| GDM Group | <4000 g | >4000 g | n | GDM Group | <4000 g | >4000 g | p |
|---|---|---|---|---|---|---|---|
| 15/16 | 53 | 5 | 58 | 15/16 | 91.40% | 8.60% | p = 0.5455 |
| 17/18 | 61 | 4 | 65 | 17/18 | 93.85% | 6.15% | |
| Total | 114 | 9 | 123 |
| OGTT | Group—15/16 | Group—17/18 | n | p | ||
|---|---|---|---|---|---|---|
| Fasting | 13 | 22.4% | 22 | 33.8% | 35 | p < 0.0001 |
| Fasting glucose and 1-h after OGTT | 1 | 1.7% | 4 | 6.15% | 5 | |
| Fasting glucose and 2-h after OGTT | 18 | 31% | 3 | 4.61% | 21 | |
| 2-h after OGTT | 26 | 44.8% | 19 | 29.2% | 45 | |
| 1-h and 2-h after OGTT | 0 | 0 | 7 | 10.76% | 7 | |
| 1-h after OGTT | 0 | 7 | 10.76% | 7 | ||
| Fasting and 1-h and 2-h after OGTT | 0 | 3 | 4.6% | 3 | ||
| Total | 58 | 65 | 123 | |||
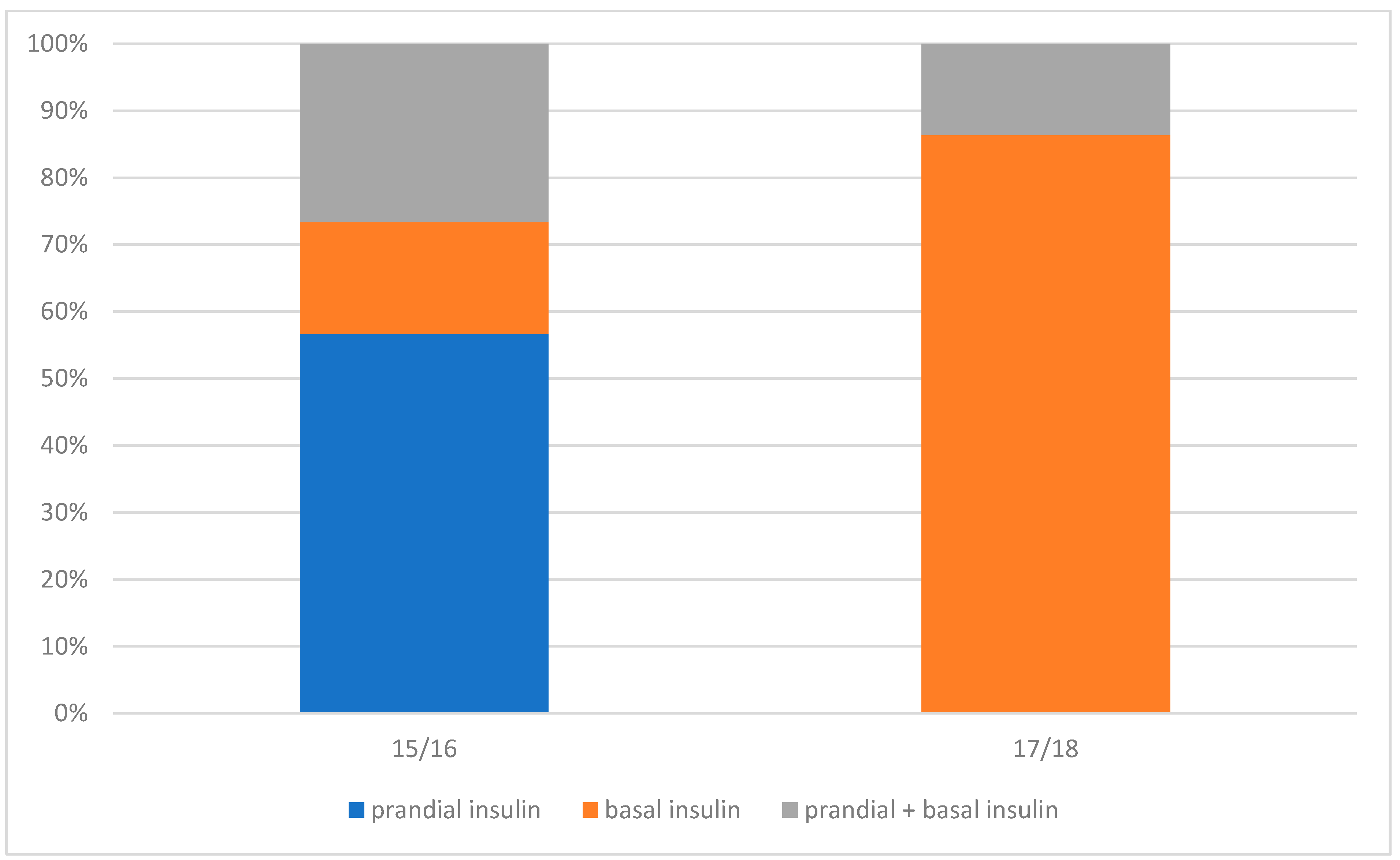
| Mode of GDM Treatment | GDM Group | |||||
|---|---|---|---|---|---|---|
| 15/16 (n = 58) | 17/18 (n = 65) | n | ||||
| Diet + Insulin | 30 | 51.7% | 22 | 33.8% | 52 | p = 0.04244 |
| Prandial insulin only | 17 | 56.7% | 0 | 0 | ||
| Basal insulin only | 5 | 16.7% | 19 | 86.4% | ||
| Prandial+basal insulin | 8 | 26.7% | 3 | 13.6% | ||
| Diet | 28 | 48.3% | 43 | 66.2% | 71 | |
| Variable | GDM in Group-15/16 Treated with Diet and Insulin | GDM in Group-15/16 Treated with Diet Only | p | ||||
| Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| BMI, kg/m2 | 28.05 | 24.30 | 31.97 | 24.53 | 20.51 | 25.60 | p = 0.037626 |
| Age, years | 32.0 | 29.0 | 36.0 | 29.0 | 26.0 | 32.0 | p = 0.019224 |
| GDM in Group-17/18 Treated with Diet and Insulin | GDM in Group-17/18 Treated with Diet Only | p | |||||
| Median | Q1 | Q3 | Median | Q1 | Q3 | ||
| BMI, kg/m2 | 29.67 | 21.3 | 35.12 | 23.4 | 20.9 | 27.34 | p = 0.125727 |
| Age, years | 31.5 | 29.0 | 34.0 | 30.0 | 27.0 | 35.0 | p = 0.579396 |
| Maternal Comorbidities | GDM Group-15/16 (n = 58) | GDM Group-17/18 (n = 65) | Total | |
|---|---|---|---|---|
| Arterial hypertension | 2 | 6 | 8 | p = 0.19422 |
| Hypothyroidism | 7 | 18 | 25 | p = 0.02596 |
| Polycystic ovary syndrome | 2 | 2 | 4 | p = 0.64637 |
| Neonatal Comorbidities | GDM Group-15/16 | GDM Group-17/18 | Total | |
|---|---|---|---|---|
| Prolonged jaundice | 9 | 10 | 19 | p = 0.58926 |
| Hypoglycemia | 0 | 3 | 3 | p = 0.14434 |
| Heart defect | 0 | 2 | 2 | p = 0.27722 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cichocka, E.; Gumprecht, J. Does the Change in the Diagnostic Criteria for Gestational Diabetes in Poland Affect Maternal and Fetal Complications? A Prospective Study. Medicina 2022, 58, 398. https://doi.org/10.3390/medicina58030398
Cichocka E, Gumprecht J. Does the Change in the Diagnostic Criteria for Gestational Diabetes in Poland Affect Maternal and Fetal Complications? A Prospective Study. Medicina. 2022; 58(3):398. https://doi.org/10.3390/medicina58030398
Chicago/Turabian StyleCichocka, Edyta, and Janusz Gumprecht. 2022. "Does the Change in the Diagnostic Criteria for Gestational Diabetes in Poland Affect Maternal and Fetal Complications? A Prospective Study" Medicina 58, no. 3: 398. https://doi.org/10.3390/medicina58030398