
Prognostic Impact of In-Hospital Use of Mechanical Cardiopulmonary Resuscitation Devices Compared with Manual Cardiopulmonary Resuscitation: A Nationwide Population-Based Observational Study in South Korea

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
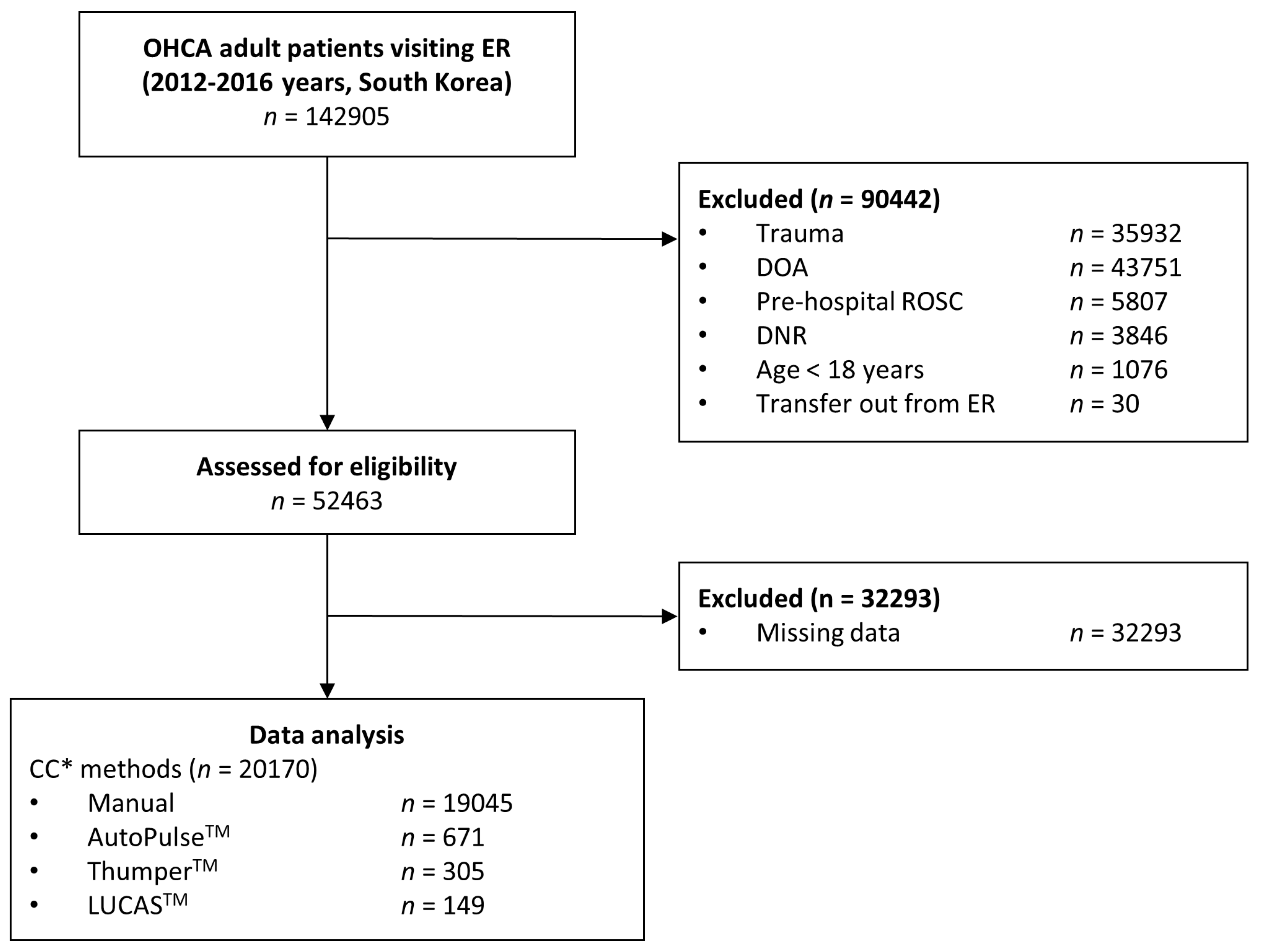
2.2. Participants
2.3. Outcome Measures
2.4. Data Extraction
2.5. Statistical Analyses
2.6. Ethics Statement
3. Results
3.1. Study Subject Characteristics
3.2. Matched Univariate Analysis
3.3. Matched Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jiang, J.; Ma, D.; Li, B.; Yue, Y.; Xue, F. Video laryngoscopy does not improve the intubation outcomes in emergency and critical patients—A systematic review and meta-analysis of randomized controlled trials. Crit. Care 2017, 21, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savino, P.B.; Reichelderfer, S.; Mercer, M.P.; Wang, R.C.; Sporer, K.A. Direct versus video laryngoscopy for prehospital intubation: A systematic review and meta-analysis. Acad. Emerg. Med. 2017, 24, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Gates, S.; Quinn, T.; Deakin, C.D.; Blair, L.; Couper, K.; Perkins, G.D. Mechanical chest compression for out of hospital cardiac arrest: Systematic review and meta-analysis. Resuscitation 2015, 94, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Circulation-Part 3: Adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef]
- Ewy, G.A. The mechanism of blood flow during chest compressions for cardiac arrest is probably influenced by the patient’s chest configuration. Acute Med. Surg. 2018, 5, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Ewy, G.A.; Zuercher, M. Role of manual and mechanical chest compressions during resuscitation efforts throughout cardiac arrest. Future Cardiol. 2013, 9, 863–873. [Google Scholar] [CrossRef]
- Zoll Medical. AutoPulse Resuscitation System. Available online: https://www.zoll.com/products/automated-cpr/autopulse-for-ems (accessed on 11 January 2022).
- Michigan Instruments. Thumper. Available online: https://www.michiganinstruments.com (accessed on 11 January 2022).
- Contol, P. LUCAS Chest Compression System. Available online: https://www.lucas-cpr.com (accessed on 11 January 2022).
- Khan, S.U.; Lone, A.N.; Talluri, S.; Khan, M.Z.; Khan, M.U.; Kaluski, E. Efficacy and safety of mechanical versus manual compression in cardiac arrest—A Bayesian network meta-analysis. Resuscitation 2018, 130, 182–188. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Hayashida, K.; Tagami, T.; Fukuda, T.; Suzuki, M.; Yonemoto, N.; Kondo, Y.; Ogasawara, T.; Sakurai, A.; Tahara, Y.; Nagao, K.; et al. Mechanical Cardiopulmonary Resuscitation and Hospital Survival Among Adult Patients With Nontraumatic Out-of-Hospital Cardiac Arrest Attending the Emergency Department: A Prospective, Multicenter, Observational Study in Japan (SOS-KANTO [Survey of Survivors after Out-of-Hospital Cardiac Arrest in Kanto Area] 2012 Study). J. Am. Heart Assoc. 2017, 6, e007420. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.K.; Huang, M.C.; Feng, Y.T.; Jeng, W.H.; Chung, T.C.; Lau, Y.W.; Cheng, K.I. Effectiveness of Mechanical Chest Compression for Out-of-Hospital Cardiac Arrest Patients in an Emergency Department. J. Chin. Med. Assoc. 2015, 78, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.T.; Kim, J.G.; Jang, Y.S.; Kang, G.H.; Kim, W.; Choi, H.Y.; Jun, G.S. Comparison of in-Hospital Use of Mechanical Chest Compression Devices for Out-of-Hospital Cardiac Arrest Patients: AUTOPULSE vs LUCAS. Medicine 2019, 98, e17881. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Shiozaki, T.; Hirose, T.; Ohnishi, M.; Nakamori, Y.; Ogura, H.; Shimazu, T. Load-Distributing-Band Cardiopulmonary Resuscitation for Out-of-Hospital Cardiac Arrest Increases Regional Cerebral Oxygenation: A Single-Center Prospective Pilot Study. Scand. J. Trauma. Resusc. Emerg. Med. 2015, 23, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duchateau, F.X.; Gueye, P.; Curac, S.; Tubach, F.; Broche, C.; Plaisance, P.; Payen, D.; Mantz, J.; Ricard-Hibon, A. Effect of the AutoPulse automated band chest compression device on hemodynamics in out-of-hospital cardiac arrest resuscitation. Intensive Care Med. 2010, 36, 1256–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gässler, H.; Ventzke, M.M.; Lampl, L.; Helm, M. Transport with ongoing resuscitation: A comparison between manual and mechanical compression. Emerg. Med. J. 2013, 30, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Lyon, R.M.; Crawford, A.; Crookston, C.; Short, S.; Clegg, G.R. The combined use of mechanical CPR and a carry sheet to maintain quality resuscitation in out-of-hospital cardiac arrest patients during extrication and transport. Resuscitation 2015, 93, 102–106. [Google Scholar] [CrossRef]
- Gao, C.; Chen, Y.; Peng, H.; Chen, Y.; Zhuang, Y.; Zhou, S. Clinical evaluation of the AutoPulse automated chest compression device for out-of-hospital cardiac arrest in the northern district of Shanghai, China. Arch. Med. Sci. 2016, 12, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, A.; Rea, T.D.; Sayre, M.R.; Christenson, J.; Anton, A.R.; Mosesso, V.N., Jr.; Ottingham, L.V.; Olsufka, M.; Pennington, S.; White, L.J.; et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: A randomized trial. JAMA 2006, 295, 2620–2628. [Google Scholar] [CrossRef] [Green Version]
- Wik, L.; Olsen, J.A.; Persse, D.; Sterz, F.; Lozano, M., Jr.; Brouwer, M.A.; Westfall, M.; Souders, C.M.; Malzer, R.; van Grunsven, P.M.; et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation 2014, 85, 741–748. [Google Scholar] [CrossRef]
- Koster, R.W.; Beenen, L.F.; van der Boom, E.B.; Spijkerboer, A.M.; Tepaske, R.; van der Wal, A.C.; Beesems, S.G.; Tijssen, J.G. Safety of mechanical chest compression devices AutoPulse and LUCAS in cardiac arrest: A randomized clinical trial for non-inferiority. Eur. Heart J. 2017, 38, 3006–3013. [Google Scholar] [CrossRef]
- Betz, A.E.; Menegazzi, J.J.; Logue, E.S.; Callaway, C.W.; Wang, H.E. A randomized comparison of manual, mechanical and high-impulse chest compression in a porcine model of prolonged ventricular fibrillation. Resuscitation 2006, 69, 495–501. [Google Scholar] [CrossRef]
- Steen, S.; Liao, Q.; Pierre, L.; Paskevicius, A.; Sjöberg, T. Evaluation of LUCAS, a new device for automatic mechanical compression and active decompression resuscitation. Resuscitation 2002, 55, 285–299. [Google Scholar] [CrossRef]
- Rubertsson, S.; Karlsten, R. Increased cortical cerebral blood flow with LUCAS; a new device for mechanical chest compressions compared to standard external compressions during experimental cardiopulmonary resuscitation. Resuscitation 2005, 65, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Lall, R.; Quinn, T.; Deakin, C.D.; Cooke, M.W.; Horton, J.; Lanb, S.E.; Slowther, A.-M.; Woollard, M.; Carson, A.; et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): A pragmatic, cluster randomised controlled trial. Lancet 2015, 385, 947–955. [Google Scholar] [CrossRef] [Green Version]
- Rubertsson, S.; Lindgren, E.; Smekal, D.; Östlund, O.; Silfverstolpe, J.; Lichtveld, R.A.; Boomars, R.; Ahlstedt, B.; Skoog, G.; Kastberg, R.; et al. Mechanical chest compressions and simultaneous defibrillation vs conventional cardiopulmonary resuscitation in out-of-hospital cardiac arrest: The LINC randomized trial. JAMA 2014, 311, 53–61. [Google Scholar] [CrossRef]
- Smekal, D.; Johansson, J.; Huzevka, T.; Rubertsson, S. A pilot study of mechanical chest compressions with the LUCAS™ device in cardiopulmonary resuscitation. Resuscitation 2011, 82, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Azadi, N.; Niemann, J.T.; Thomas, J.L. Coronary imaging and intervention during cardiovascular collapse: Use of the LUCAS mechanical CPR device in the cardiac catheterization laboratory. J. Invasive Cardiol. 2012, 24, 79–83. [Google Scholar] [PubMed]
- Levy, M.; Yost, D.; Walker, R.G.; Scheunemann, E.; Mendive, S.R. A quality improvement initiative to optimize use of a mechanical chest compression device within a high-performance CPR approach to out-of-hospital cardiac arrest resuscitation. Resuscitation 2015, 92, 32–37. [Google Scholar] [CrossRef]
- Oberladstaetter, D.; Braun, P.; Freund, M.C.; Rabl, W.; Paal, P.; Baubin, M. Autopsy is more sensitive than computed tomography in detection of LUCAS-CPR related non-dislocated chest fractures. Resuscitation 2012, 83, e89–e90. [Google Scholar] [CrossRef]
- Smekal, D.; Lindgren, E.; Sandler, H.; Johansson, J.; Rubertsson, S. CPR-related injuries after manual or mechanical chest compressions with the LUCAS™ device: A multicentre study of victims after unsuccessful resuscitation. Resuscitation 2014, 85, 1708–1712. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Classification | AutoPulseTM | ThumperTM | LUCASTM | |
|---|---|---|---|---|
| Specification of device | Backboard | Yes | Yes | Yes |
| Connecting arm | 2 | 1 | 2 | |
| Compression band | Yes | No | No | |
| Compression tool | Band type | Pad type | Suction cup type | |
| Movement of the device during CPR | Possible | Possible | Possible | |
| Driving force | Battery | Oxygen or air | Battery | |
| CC parameters | CC depth | 20% of Chest AP diameter | 5–6 cm | 4–5 cm |
| CC rate | 80 ± 5/min | 100 ± 6/min | 102 ± 2/min | |
| Duty cycle | 50 ± 5% | 50/50 cycle | 50 ± 5% | |
| CC location | Unknown | The lower half of the sternum | The lower half of the sternum | |
| Active decompression | Impossible | Impossible | Possible | |
| Devices | AutoPulseTM | ThumperTM | LUCASTM | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Manual CPR ** N = 671 | Mechanical CPR ** N = 671 | p-Value * | Manual CPR ** N = 305 | Mechanical CPR ** N = 305 | p-Value * | Manual CPR ** N = 149 | Mechanical CPR ** N = 149 | p-Value * | |
| Age, years | 69 (57–78) | 69 (57–78) | 0.951 | 69 (56–78) | 71 (56–78) | 0.790 | 68 (56–79) | 70 (56–78) | 0.705 |
| Male | 436 (65.0%) | 445 (66.3%) | 0.646 | 185 (60.7%) | 205 (67.2%) | 0.109 | 96 (64.4%) | 101 (67.8%) | 0.624 |
| Witnessed | 380 (56.6%) | 422 (62.9%) | 0.022 | 189 (62.0%) | 184 (60.3%) | 0.740 | 94 (63.1%) | 95 (63.8%) | 1.000 |
| Place | 0.888 | 0.048 | 1.000 | ||||||
| Non-public | 545 (81.2%) | 548 (81.7%) | 258 (84.6%) | 238 (78.0%) | 116 (77.9%) | 115 (77.2%) | |||
| Public | 126 (18.8%) | 123 (18.3%) | 47 (15.4%) | 67 (22.0%) | 33 (22.1%) | 34 (22.8%) | |||
| Bystander CPR | 176 (26.2%) | 191 (28.5%) | 0.391 | 69 (22.6%) | 80 (26.2%) | 0.346 | 53 (35.6%) | 53 (35.6%) | |
| Arrest cause | 0.923 | 1.000 | 0.193 | ||||||
| Cardiac | 612 (91.2%) | 614 (91.5%) | 280 (91.8%) | 281 (92.1%) | 134 (89.9%) | 141 (94.6%) | |||
| Non-cardiac | 59 (8.8%) | 57 (8.5%) | 25 (8.2%) | 24 (7.9%) | 15 (10.1%) | 8 (5.4%) | |||
| Arrest rhythm | 1.000 | 0.506 | 0.561 | ||||||
| Non-shockable | 568 (84.6%) | 568 (84.6%) | 260 (85.2%) | 253 (83.0%) | 117 (78.5%) | 122 (81.9%) | |||
| Shockable | 103 (15.4%) | 103 (15.4%) | 45 (14.8%) | 52 (17.0%) | 32 (21.5%) | 27 (18.1%) | |||
| PCI | 10 (1.5%) | 10 (1.5%) | 1.000 | 8 (2.6%) | 6 (2.0%) | 0.787 | 12 (8.1%) | 8 (5.4%) | 0.487 |
| TTM | 22 (3.3%) | 47 (7.0%) | 0.003 | 9 (3.0%) | 9 (3.0%) | 1.000 | 14 (9.4%) | 14 (9.4%) | 1.000 |
| Pacemaker | 3 (0.4%) | 0 (0.0%) | 0.249 | 4 (1.3%) | 3 (1.0%) | 1.000 | 4 (2.7%) | 1 (0.7%) | 0.371 |
| ECMO | 7 (1.0%) | 19 (2.8%) | 0.029 | 6 (2.0%) | 4 (1.3%) | 0.750 | 11 (7.4%) | 11 (7.4%) | 1.000 |
| Sustained ROSC | 240 (35.8%) | 203 (30.3%) | 0.037 | 110 (36.1%) | 62 (20.3%) | <0.001 | 69 (46.3%) | 41 (27.5%) | 0.001 |
| Survival to discharge | 42 (6.3%) | 33 (4.9%) | 0.342 | 14 (4.6%) | 10 (3.3%) | 0.532 | 8 (5.4%) | 4 (2.7%) | 0.377 |
| AutoPulseTM | ThumperTM | LUCASTM | ||||||
|---|---|---|---|---|---|---|---|---|
| Factors | aOR (95% CI) * | p-Value | Factors | aOR (95% CI) * | p-Value | Factors | aOR (95% CI) * | p-Value |
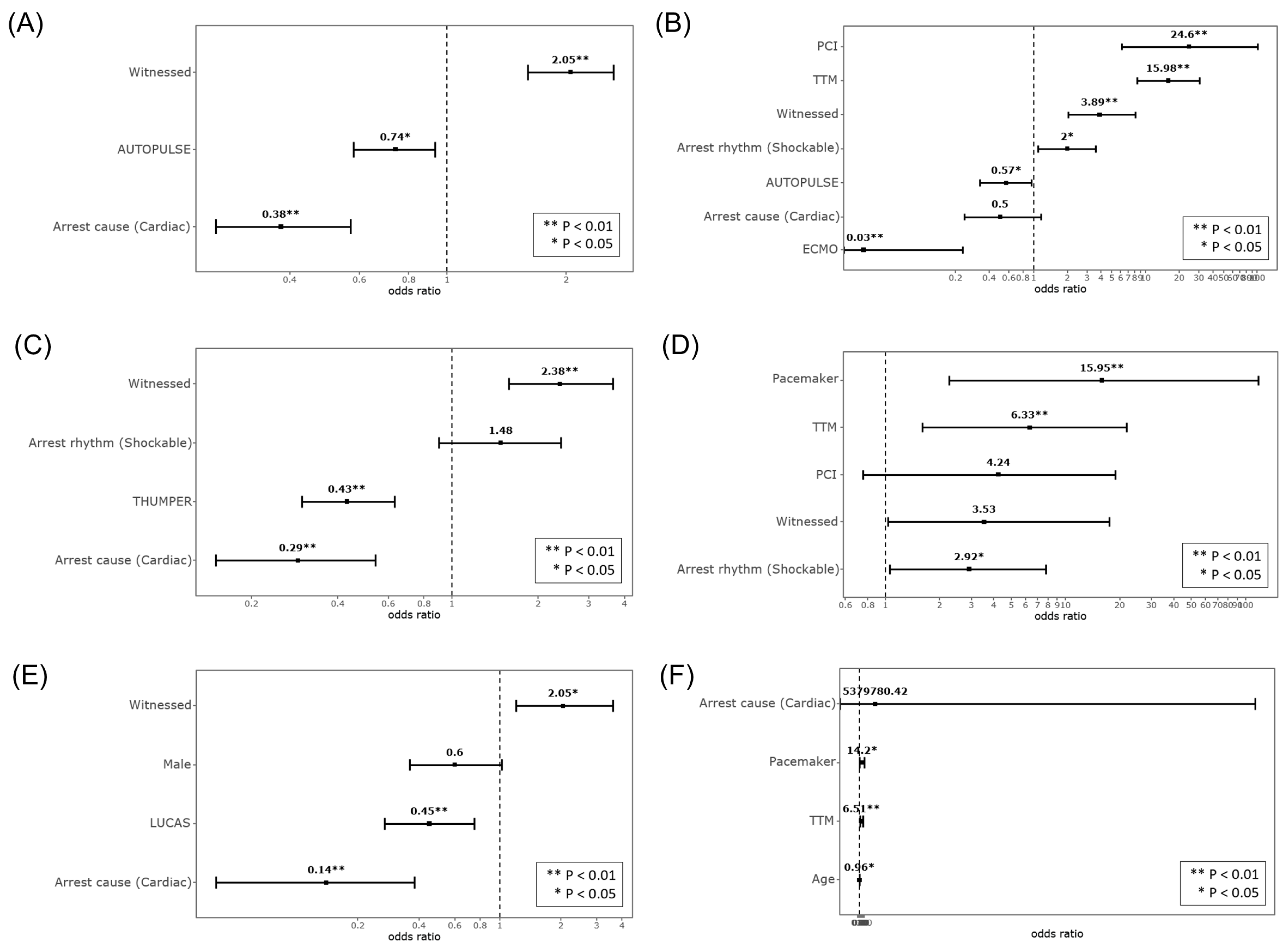
| Witnessed | 2.05 (1.60–2.62) | <0.001 | Witnessed | 2.38 (1.57–3.60) | <0.001 | Male | 0.60 (0.36–1.02) | 0.060 |
| Arrest cause (cardiac origin) | 0.38 (0.26–0.57) | <0.001 | Arrest cause (cardiac origin) | 0.29 (0.15–0.54) | <0.001 | Witnessed | 2.05 (1.19–3.55) | 0.010 |
| Mechanical CPR devices | 0.74 (0.58–0.93) | 0.011 | Arrest rhythm (shockable) | 1.48 (0.91–2.41) | 0.115 | Arrest cause (cardiac origin) | 0.14 (0.05–0.41) | <0.001 |
| Mechanical CPR devices | 0.43 (0.30–0.63) | <0.001 | Mechanical CPR devices | 0.45 (0.27–0.75) | 0.002 | |||
| AutoPulseTM | ThumperTM | LUCASTM | ||||||
|---|---|---|---|---|---|---|---|---|
| Factor | aOR (95% CI) * | p-Value | Factor | aOR (95% CI) * | p-Value | Factor | aOR (95% CI) * | p-Value |
| Witnessed | 3.89 (1.95–7.73) | <0.001 | Witnessed | 3.53 (0.90–13.92) | 0.071 | Age, year | 0.96 (0.92–1.00) | 0.033 |
| Arrest cause (cardiac origin) | 0.50 (0.23–1.09) | 0.081 | Arrest rhythm (shockable) | 2.92 (1.09–7.79) | 0.032 | Arrest cause (cardiac) | 5379780.42 (0.00–) | 0.990 |
| Arrest rhythm (shockable) | 2.00 (1.11–3.61) | 0.021 | PCI | 4.24 (0.87–20.59) | 0.072 | TTM | 6.51 (1.65–25.74) | 0.007 |
| PCI | 24.60 (6.26–96.76) | <0.001 | TTM | 6.33 (1.75–22.98) | 0.005 | Pacemaker | 14.20 (1.48–136.61) | 0.021 |
| TTM | 15.98 (8.41–30.37) | <0.001 | Pacemaker | 15.95 (2.33–109.00) | 0.004 | |||
| Mechanical CPR devices | 0.57 (0.33–0.96) | 0.035 | ||||||
| ECMO | 0.03 (0.00–0.34) | 0.004 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.; Ahn, C.; Kim, I.-Y.; Choi, H.-Y.; Kim, J.-G.; Kim, J.; Shin, H.; Moon, S.; Lee, J.; Lee, J.; et al. Prognostic Impact of In-Hospital Use of Mechanical Cardiopulmonary Resuscitation Devices Compared with Manual Cardiopulmonary Resuscitation: A Nationwide Population-Based Observational Study in South Korea. Medicina 2022, 58, 353. https://doi.org/10.3390/medicina58030353
Kim W, Ahn C, Kim I-Y, Choi H-Y, Kim J-G, Kim J, Shin H, Moon S, Lee J, Lee J, et al. Prognostic Impact of In-Hospital Use of Mechanical Cardiopulmonary Resuscitation Devices Compared with Manual Cardiopulmonary Resuscitation: A Nationwide Population-Based Observational Study in South Korea. Medicina. 2022; 58(3):353. https://doi.org/10.3390/medicina58030353
Chicago/Turabian StyleKim, Wonhee, Chiwon Ahn, In-Young Kim, Hyun-Young Choi, Jae-Guk Kim, Jihoon Kim, Hyungoo Shin, Shinje Moon, Juncheol Lee, Jongshill Lee, and et al. 2022. "Prognostic Impact of In-Hospital Use of Mechanical Cardiopulmonary Resuscitation Devices Compared with Manual Cardiopulmonary Resuscitation: A Nationwide Population-Based Observational Study in South Korea" Medicina 58, no. 3: 353. https://doi.org/10.3390/medicina58030353