
Leukocytosis and C-Reactive Protein May Predict Development of Secondary Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Laboratory Assays
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
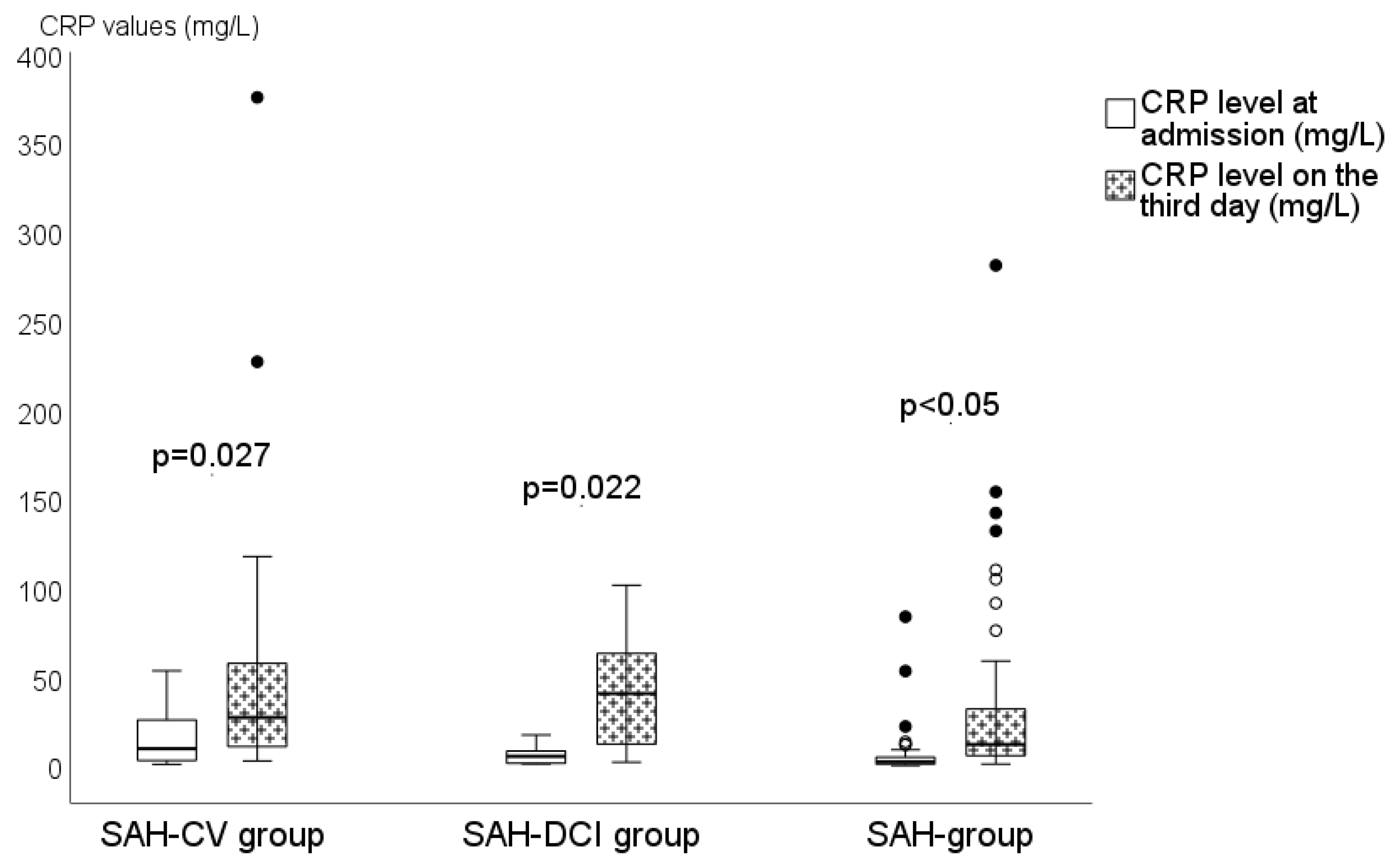
3.2. Difference in Inflammatory Parameters between Three Groups
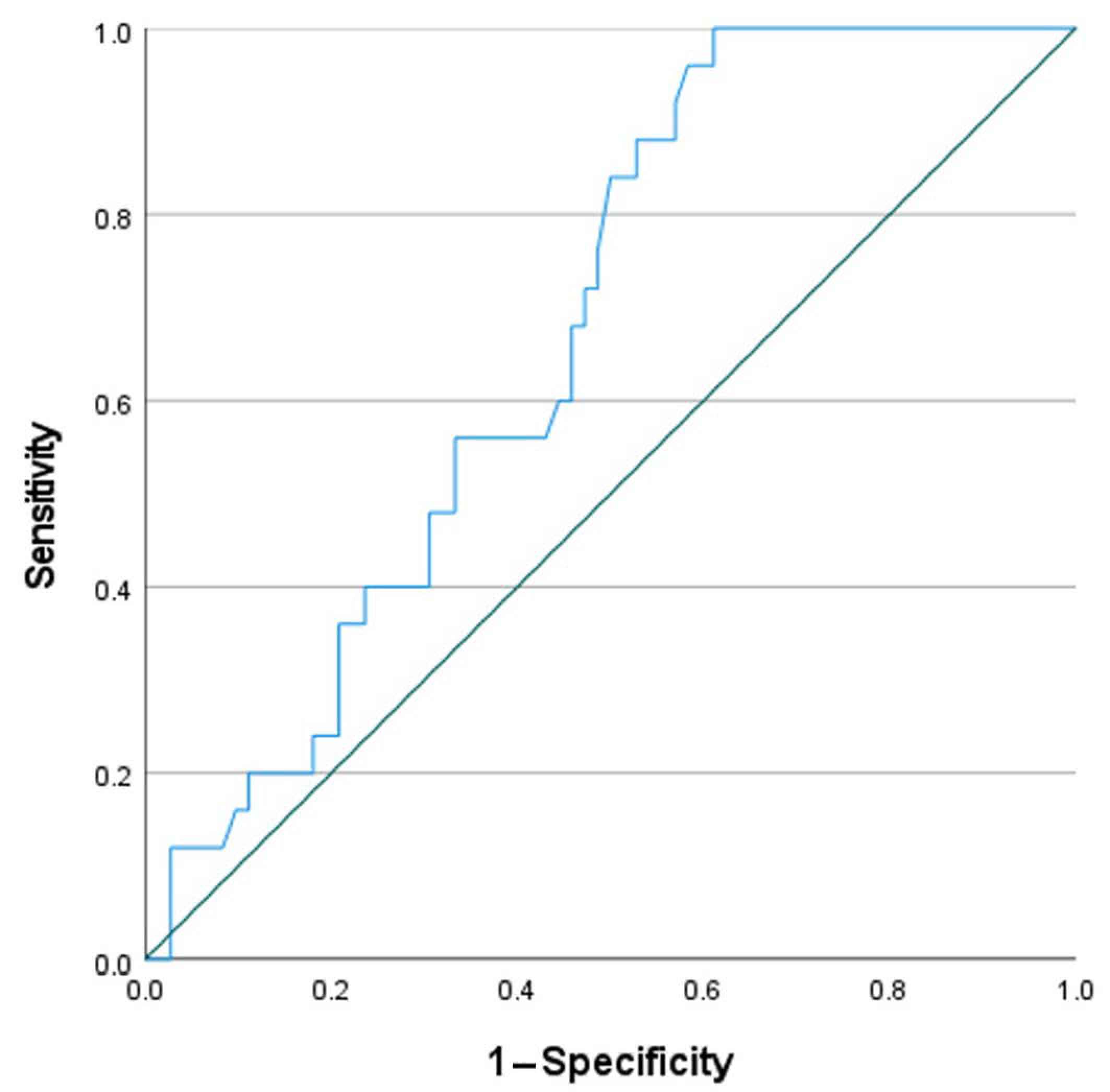
3.3. Role of Dynamic Changes in Inflammatory Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics–2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Etminan, N.; Chang, H.S.; Hackenberg, K.; de Rooij, N.K.; Vergouwen, M.D.I.; Rinkel, G.J.E.; Agra, A. Worldwide Incidence of Aneurysmal Subarachnoid Hemorrhage According to Region, Time Period, Blood Pressure, and Smoking Prevalence in the Population: A Systematic Review and Meta-analysis. JAMA Neurol. 2019, 76, 588–597. [Google Scholar] [CrossRef]
- Inagawa, T. Risk Factors for Cerebral Vasospasm Following Aneurysmal Subarachnoid Hemorrhage: A Review of the Literature. World Neurosurg. 2016, 85, 56–76. [Google Scholar] [CrossRef] [PubMed]
- Rumalla, K.; Lin, M.; Ding, L.; Gaddis, M.; Giannotta, S.L.; Attenello, F.J.; Mack, W.J. Risk Factors for Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage: A Population-Based Study of 8346 Patients. World Neurosurg. 2021, 145, e233–e241. [Google Scholar] [CrossRef]
- Phan, K.; Moore, J.M.; Griessenauer, C.J.; Xu, J.; Teng, I.; Dmytriw, A.A.; Chiu, A.H.; Ogilvy, C.S.; Thomas, A. Ultra-Early Angiographic Vasospasm After Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. World Neurosurg. 2017, 102, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Starnoni, D.; Maduri, R.; Hajdu, S.D.; Pierzchala, K.; Giammattei, L.; Rocca, A.; Grosfilley, S.B.; Saliou, G.; Messerer, M.; Daniel, R.T. Early Perfusion Computer Tomography Scan for Prediction of Vasospasm and Delayed Cerebral Ischemia After Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2019, 130, e743–e752. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Lan, F.; Zhang, Y. Associations between C-reactive protein and white blood cell count, occurrence of delayed cerebral ischemia and poor outcome following aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. Acta Neurol. Belg. 2021, 121, 1311–1324. [Google Scholar] [CrossRef]
- Available online: https://www.spkc.gov.lv/lv (accessed on 8 August 2021).
- de Oliveira Manoel, A.L.; Macdonald, R.L. Neuroinflammation as a Target for Intervention in Subarachnoid Hemorrhage. Front. Neurol. 2018, 9, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, V.Z.; Wong, G.K.C. Neuroinflammation responses after subarachnoid hemorrhage: A review. J. Clin. Neurosci. 2017, 42, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.A.; Turan, N.; Chau, M.; Pradilla, G. Inflammation, vasospasm, and brain injury after subarachnoid hemorrhage. Biomed Res. Int. 2014, 2014, 384342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, C.J.; Hopkins, S.; Vail, A.; King, A.T.; Smith, D.; Illingworth, K.J.; Clark, S.; Rothwell, N.J.; Tyrrell, P.J. Inflammation as a predictor for delayed cerebral ischemia after aneurysmal subarachnoid haemorrhage. J. NeuroInterv. Surg. 2013, 5, 512–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matano, F.; Fujiki, Y.; Mizunari, T.; Kokestu, K.; Tamaki, T.; Murai, Y.; Yokota, H.; Morita, A. Serum Glucose and Potassium Ratio as Risk Factors for Cerebral Vasospasm after Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2019, 28, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhuang, Z.; Wei, Y.; Liu, X.; Li, W.; Gao, Y.; Li, J.; Hang, C. Association of Admission Serum Glucose-Phosphate Ratio with Severity and Prognosis of Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2019, 127, e1145–e1151. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Kanamaru, K.; Shiba, M.; Fujimoto, M.; Imanaka-Yoshida, K.; Yoshida, T.; Taki, W. Cerebrospinal fluid tenascin-C in cerebral vasospasm after aneurysmal subarachnoid hemorrhage. J. Neurosurg. Anesthesiol. 2011, 23, 310–317. [Google Scholar] [CrossRef]
- Llull, L.; Thiel, S.; Amaro, S.; Cervera, Á.; Planas, A.M.; Chamorro, Á. Ficolin-1 Levels in Patients Developing Vasospasm and Cerebral Ischemia After Spontaneous Subarachnoid Hemorrhage. Mol. Neurobiol. 2017, 54, 6572–6580. [Google Scholar] [CrossRef]
- Rasmussen, R.; Bache, S.; Stavngaard, T.; Møller, K. Plasma Levels of Il-6, Il-8, Il-10, ICAM-1, VCAM-1, IFNγ, and TNFα are not Associated with Delayed Cerebral Ischemia, Cerebral Vasospasm, or Clinical Outcome in Patients with Subarachnoid Hemorrhage. World Neurosurg. 2019, 128, e1131–e1136. [Google Scholar] [CrossRef]
- Ridwan, S.; Grote, A.; Simon, M. Interleukin 6 in cerebrospinal fluid is a biomarker for delayed cerebral ischemia (DCI) related infarctions after aneurysmal subarachnoid hemorrhage. Sci. Rep. 2021, 11, 12. [Google Scholar] [CrossRef]
- Chaudhry, S.R.; Güresir, A.; Stoffel-Wagner, B.; Fimmers, R.; Knife, T.M.; Dietrich, D.; Lamprecht, A.; Vatter, H.; Gūresir, E.; Muhammad, S. Systemic High-Mobility Group Box-1: A Novel Predictive Biomarker for Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage. Crit. Care Med. 2018, 46, e1023–e1028. [Google Scholar] [CrossRef] [PubMed]
- Przybycien-Szymanska, M.M.; Ashley, W.W., Jr. Biomarker Discovery in Cerebral Vasospasm after Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2015, 24, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Hurth, H.; Birkenhauer, U.; Steiner, J.; Schlak, D.; Hennersdorf, F.; Ebner, F.H. Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage–Serum D-dimer and C-reactive Protein as Early Markers. J. Stroke Cerebrovasc. Dis. 2020, 29, 104558. [Google Scholar] [CrossRef]
- Fountas, K.N.; Tasiou, A.; Kapsalaki, E.Z.; Paterakis, K.N.; Grigorian, A.A.; Lee, G.P.; Robinson, J.S., Jr. Serum and cerebrospinal fluid C-reactive protein levels as predictors of vasospasm in aneurysmal subarachnoid hemorrhage. Neurosurg. Focus 2009, 26, E22. [Google Scholar] [CrossRef] [Green Version]
- Romero, F.R.; Cataneo, D.C.; Cataneo, A.J.M. C-reactive protein and vasospasm after aneurysmal subarachnoid hemorrhage. Acta Cir. Bras. 2014, 29, 340–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, Y.T.; Lee, J.H.; Lee, H.; Lee, H.K.; Hwang, J.W.; Lim, Y.J.; Park, H.P. The postoperative C-reactive protein level can be useful prognostic Factor for poor outcome and symptomatic vasospasm in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. Anesthesiol. 2012, 24, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucke-Wold, B.P.; Logsond, A.F.; Manoranjan, B.; Turner, R.C.; McConnell, E.; Vates, G.E.; Huber, J.D.; Rosen, C.L.; Simard, J.M. Aneurysmal Subarachnoid Hemorrhage and Neuroinlfammation: A Comprehensive Review. Int. J. Mol. Sci. 2016, 17, 497. [Google Scholar] [CrossRef]
- Moraes, L.; Grille, S.; Morelli, P.; Mila, R.; Trias, N.; Brugnini, A.; LLuberas, N.; Biestro, A.; Lens, D. Immune cells subpopulations in cerebrospinal fluid and peripheral blood of patients with aneurysmal subarachnoid hemorrhage. Springerplus 2015, 4, 195. [Google Scholar] [CrossRef] [Green Version]
- Choy, E.; Rose-John, S. Interleukin-6 as a multifunctional regulator: Inflammation, immune response, and fibrosis. J. Scleroderma Relat. Disord. 2017, 2 (Suppl. 2), S1–S5. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Rodríguez, A.; Egea-Guerrero, J.J.; de Azúa-López, Z.R.; Murillo-Cabezas, F. Biomarkers of vasospasm development and outcome in aneurysmal subarachnoid hemorrhage. J. Neurol. Sci. 2014, 341, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Ciurea, A.V.; Palade, C.; Voinescu, D.; Nica, D.A. Subarachnoid hemorrhage and cerebral vasospasm–literature review. J. Med. Life 2013, 6, 120–125. [Google Scholar]
- Francoeur, C.L.; Mayer, S.A. Management of delayed cerebral ischemia after subarachnoid hemorrhage. Crit. Care 2016, 20, 277. [Google Scholar] [CrossRef] [Green Version]
- Rajajee, V. Grading scales in subarachnoid hemorrhage–many options, but do we have a winner? Eur. J. Neurol. 2018, 25, 207–208. [Google Scholar] [CrossRef]
- Rosen, D.S.; Macdonald, R.L. Subarachnoid hemorrhage grading scales: A systematic review. Neurocrit. Care 2005, 2, 110–118. [Google Scholar] [CrossRef]
- Degen, L.A.R.; Mees, S.M.D.; Algra, A.; Rinkel, G.J.E. Interobserver variability of grading scales for aneurysmal subarachnoid hemorrhage. Stroke 2011, 42, 1546–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerlaan, H.E.; van Dijk, J.M.C.; Jansen-van der Weide, M.C.; de Groot, J.C.; Groen, R.J.M.; Mooij, J.J.A.; Oudkerk, M. Intracranial aneurysms in patients with subarachnoid hemorrhage: CT angiography as a primary examination tool for diagnosis—systematic review and meta-analysis. Radiology 2011, 258, 134–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legriel, S.; Grigoresco, B.; Martel, P.; Henry-Lagarrigue, M.; Lvovschi, V.; Troché, G.; Amara, M.; Jacq, G.; Bruneel, F.; Brenard, M.; et al. Diagnostic Accuracy of Procalcitonin for Early Aspiration Pneumonia in Critically Ill Patients with Coma: A Prospective Study. Neurocrit. Care 2019, 30, 440–448. [Google Scholar] [CrossRef]
- Vahtera, A.S.; Junttila, E.K.; Jalkanen, L.V.; Huhtala, H.S.; Katanadova, K.V.; Hélen, P.T.; Kuitunen, A.H. Activation of Bloos Coagulation After Aneurysmal Subarachnoid Hemorrhage: A Prospective Observational Trial of Rotational Tromboelastometry. World Neurosurg. 2019, 122, e334–e341. [Google Scholar] [CrossRef] [Green Version]
- Hakimi, R.; Alexandrov, A.V.; Garami, Z. Neuro-ultrasonography. Neurol. Clin. 2020, 38, 215–229. [Google Scholar] [CrossRef]
- Robba, C.; Goffi, A.; Geeraets, T.; Cardim, D.; Via, G.; Czosnyka, M.; Park, S.; Sarwal, A.; Padayachy, L.; Rasulo, F.; et al. Brain ultrasonography: Methodology, basic and advanced principles and clinical applications. A narrative review. Intensive Care Med. 2019, 45, 913–927. [Google Scholar] [CrossRef]
- Marshall, S.A.; Nyquist, P.; Ziai, W. The role of transcranial Doppler ultrasonography in the diagnosis and management of vasospasm after aneurysmal subarachnoid hemorrhage. Neurosurg. Clin. N. Am. 2010, 21, 291–303. [Google Scholar] [CrossRef]
- Behrouz, R. The Rise and Fall of Transcranial Doppler Ultrasonography for the Diagnosis of Vasospasm in Aneurysmal Subarachnoid Hemorrhage. J. Neurosurg. Anesthesiol. 2019, 31, 79–80. [Google Scholar] [CrossRef]
- Kondziella, D.; Friberg, C.K.; Wellwood, I.; Reiffurth, C.; Fabricius, M.; Dreier, J.P. Continuous EEG monitoring in aneurysmal subarachnoid hemorrhage: A systematic review. Neurocrit. Care 2015, 22, 450–461. [Google Scholar] [CrossRef]
- Schulz, M.K.; Wang, L.P.; Tange, M.; Bjerre, P. Cerebral microdialysis monitoring: Determination of normal and ischemic cerebral metabolisms in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2000, 93, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Peerdeman, S.M.; van Tulder, M.W.; Vandertop, W.P. Cerebral microdialysis as a monitoring method in subarachnoid hemorrhage patients, and correlation with clinical events–a systematic review. J. Neurol. 2003, 250, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Khozhenko, A.; Lamperti, M.; Terracina, S.; Bilotta, F. Can Cerebral Near-infrared Spectroscopy Predict Cerebral Ischemic Events in Neurosurgical Patients? A Narrative Review of the Literature. J. Neurosurg. Anesthesiol. 2019, 31, 378–384. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Totally n = 117 | SAH-CV Group n = 25 | SAH-DCI Group n = 12 | SAH Group (Controls) n = 80 | p-Value |
|---|---|---|---|---|---|
| Demographic data | |||||
| Male sex, n (%) | 48 (41) | 13 (52) | 9 (75) & | 26 (32.5) | 0.005 & |
| Age, yr (mean ± SD) | 56 ± 15 | 53 ± 13 | 47 ± 14 & | 58 ± 157 | 0.022 & |
| BMI, kg/m2 (mean ± SD) * | 26 ± 4 | 25.5 ± 3.5 | 26 ± 4 | 26 ± 4 | NS |
| Comorbidities | |||||
| Arterial hypertension, n (%) * | 70 (63.6) | 14 (63.6) | 5 (45.5) | 51 (66.2) | NS |
| Diabetes mellitus, n (%) * | 6 (5.4) | 1 (4.3) | 0 (0) | 5 (6.5) | NS |
| General atherosclerosis, n (%) * | 16 (14.7) | 2 (8.7) | 2 (18.2) | 12 (16) | NS |
| Harmful habits | |||||
| Smoking, n (%) * | 14 (24.6) | 2 (8.7) | 4 (50) | 8 (19.5) | NS |
| Chronic alcohol intake, n (%) * | 7 (10.8) | 2 (20) | 0 (0) | 5 (10.9) | NS |
| SAH severity according to scores | |||||
| GCS, points (median) | 15 | 13 # | 15 | 15 # | 0.025 # |
| Fisher score grade, n (%) | |||||
| I | 3 (2.6) | 0 (0) | 0 (0) | 3 (3.8) | NS |
| II | 10 (8.5) | 1 (4) # | 2 (16.7) & | 7 (8.8) # | 0.011 # |
| 0.003 & | |||||
| III | 30 (25.6) | 7 (28) #,$ | 5 (41.7) &,$ | 18 (22.5) # | 0.003 # |
| <0.001 &,$ | |||||
| IV (without ICH) | 74 (63.2) | 17 (68) #,$ | 5 (41.7) &,$ | 52 (65) #,& | <0.001 #,&,$ |
| Mortality, n (%) | 14 (12) | 8 (32) # | 1 (8.3) | 5 (6.3) # | <0.001 # |
| Length of stay in hospital, days (median) | |||||
| Days in ICU | 4 | 8 # | 5 | 4 # | 0.002 # |
| Total stay | 18 | 23 | 21 | 17.5 | NS |
| Laboratory Parameters | Totally n = 117 | SAH-CV Group n = 25 | SAH-DCI Group n = 12 | SAH Group (Controls) n = 80 | p-Value |
|---|---|---|---|---|---|
| WBC count at admission (×109/L) (mean ± SD) | 11.7 ± 3.8 | 13.2 ± 3.3 *,$ | 11.3 ± 4.7 $ | 11.2 ± 3.7 * | 0.01 *, 0.016 $ |
| WBC count on the third day (×109/L) (mean ± SD) | 11.6 ± 3.6 | 12.4 ± 3.5 | 12.5 ± 3.9 | 11.1 ± 3.7 | NS |
| CRP values at admission (mg/L) (median) | 2.95 | 9.3 *,$ | 1.1 $ | 1.9 * | <0.001 *, 0.017 $ |
| CRP values on the third day (mg/L) (median) | 15.5 | 26.3 | 25.5 | 11.67 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buce-Satoba, I.; Rozkalne, D.; Mamaja, B.; Krumina, G.; Ozolina, A. Leukocytosis and C-Reactive Protein May Predict Development of Secondary Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage. Medicina 2022, 58, 323. https://doi.org/10.3390/medicina58020323
Buce-Satoba I, Rozkalne D, Mamaja B, Krumina G, Ozolina A. Leukocytosis and C-Reactive Protein May Predict Development of Secondary Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage. Medicina. 2022; 58(2):323. https://doi.org/10.3390/medicina58020323
Chicago/Turabian StyleBuce-Satoba, Ieva, Daina Rozkalne, Biruta Mamaja, Gaida Krumina, and Agnese Ozolina. 2022. "Leukocytosis and C-Reactive Protein May Predict Development of Secondary Cerebral Vasospasm in Patients with Aneurysmal Subarachnoid Hemorrhage" Medicina 58, no. 2: 323. https://doi.org/10.3390/medicina58020323