
Interaction between Dexamethasone, Ropivacaine, and Contrast Media Used in Interventional Pain Treatment: Considerations in Safety
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
- 0.1% ropivacaine + dexamethasone,
- 0.1% ropivacaine + dexamethasone + contrast media,
- 0.2% ropivacaine + dexamethasone,
- 0.2% ropivacaine + dexamethasone + contrast media.
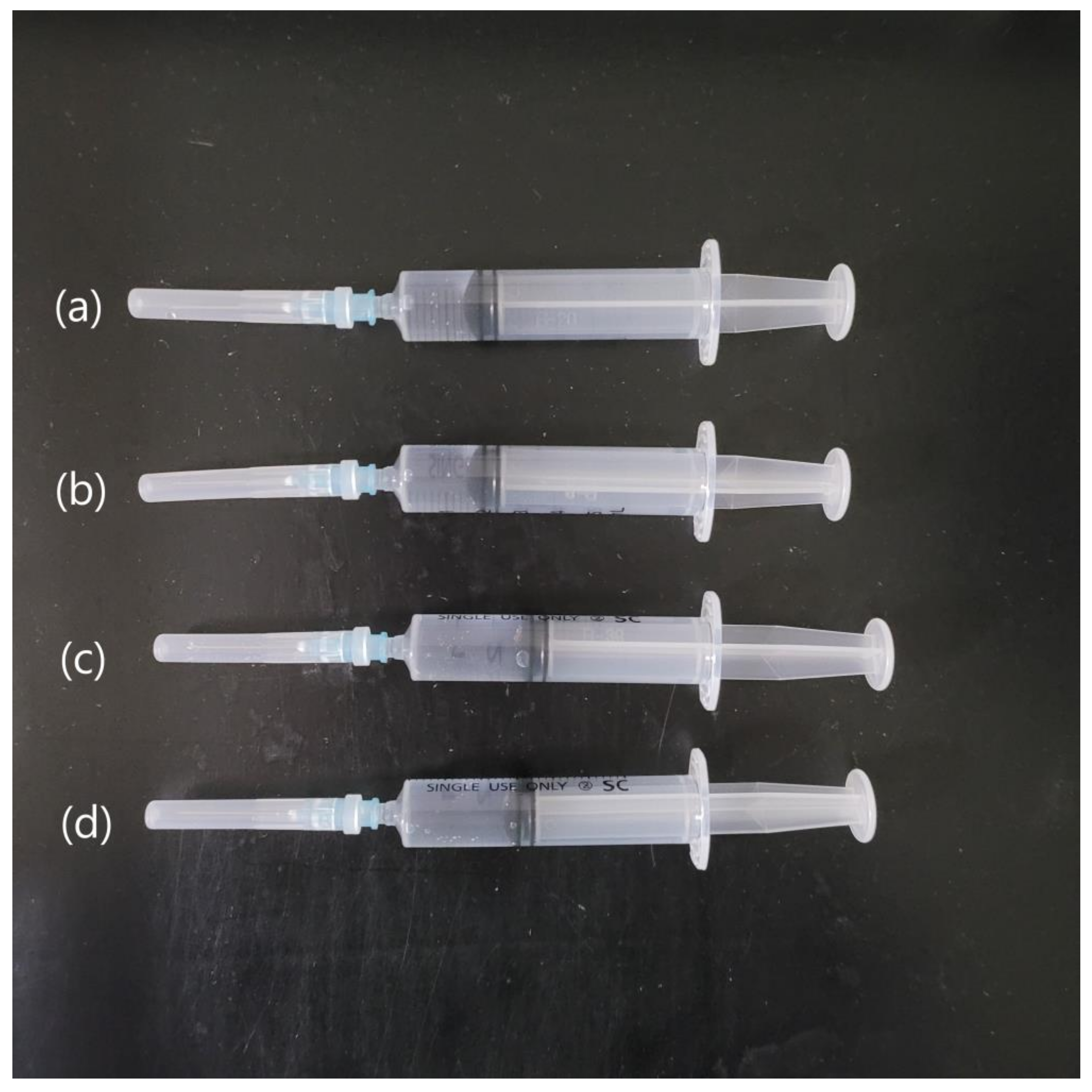
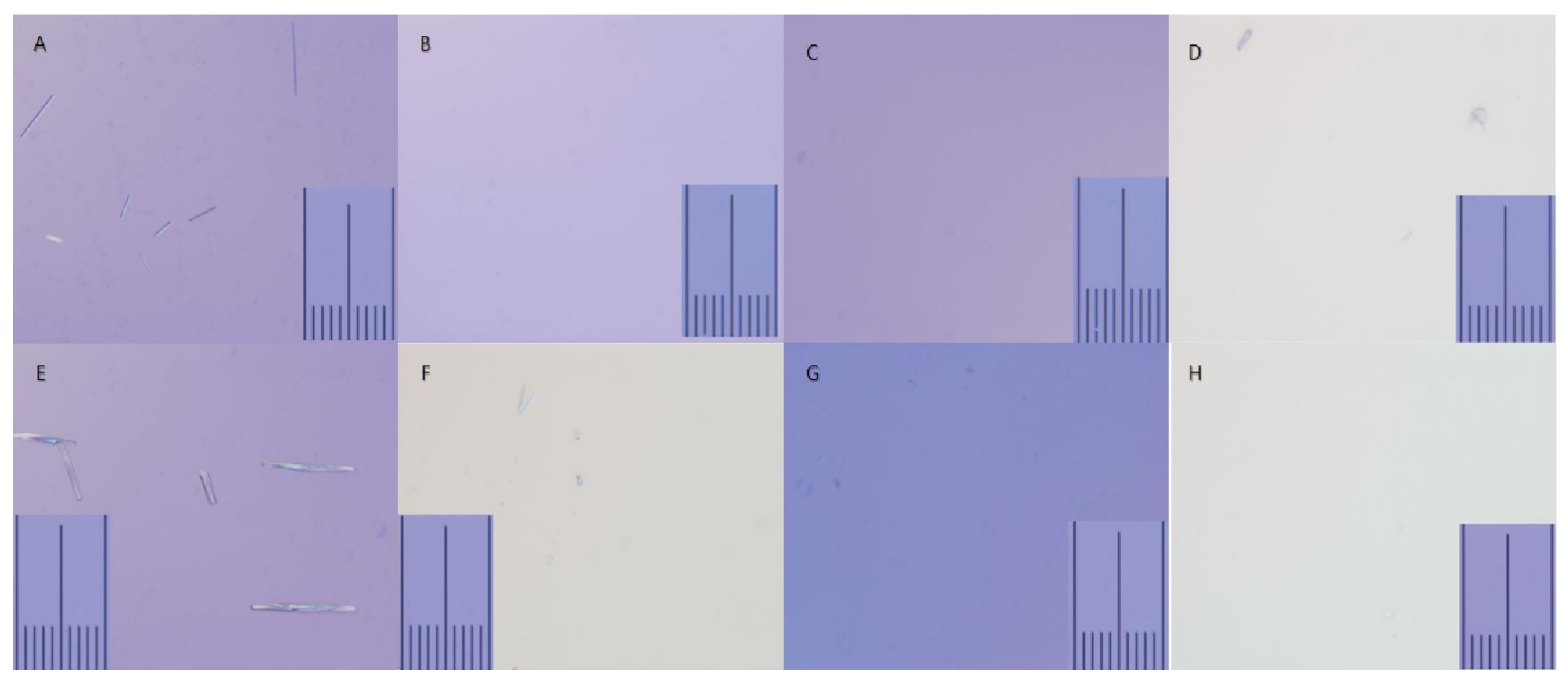
2.1. Macroscopic and Microscopic Analysis of Mixtures
2.2. Measurement of pH
3. Results
3.1. Macroscopic and Microscopic Analysis of Mixtures
3.2. pH Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rowlingson, J.C.; Kirschenbaum, L.P. Epidural analgesic techniques in the management of cervical pain. Anesth. Analg. 1986, 65, 938–942. [Google Scholar] [CrossRef]
- Leung, S.; Chau, W.; Law, S.; Fung, K. Clinical value of transforaminal epidural steroid injection in lumbar radiculopathy. Hong Kong Med. J. 2015, 21, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.Y.; Lee, J.W.; Lee, E.; Yeom, J.S.; Kim, K.; Shin, H.; Kang, H.S. Evaluation of the efficacy and safety of epidural steroid injection using a nonparticulate steroid, dexamethasone or betamethasone: A double-blind, randomized, crossover, clinical trial. Korean J. Pain 2022, 35, 336–344. [Google Scholar] [CrossRef]
- Kim, E.J.; Moon, J.Y.; Park, K.S.; Yoo, D.H.; Kim, Y.C.; Sim, W.S.; Lee, C.J.; Shin, H.Y.; Kim, J.H.; Kim, Y.D.; et al. Epidural Steroid Injection in Korean Pain Physicians: A National Survey. Korean J. Pain 2014, 27, 35–42. [Google Scholar] [CrossRef]
- Robecchi, A.; Capra, R. Hydrocortisone (compound F); first clinical experiments in the field of rheumatology. Minerva Med. 1952, 43, 1259–1263. [Google Scholar] [PubMed]
- Manchikanti, L.; Sanapati, M.R.; Soin, A.; Manchikanti, M.V.; Pampati, V.; Singh, V.; Hirsch, J.A. An updated analysis of utilization of epidural procedures in managing chronic pain in the Medicare population from 2000 to 2018. Pain Physician 2020, 23, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kyoung-ho, S.; Park, S.J.; Lee, G.J.; Chang-Hyung, L.; Kim, D.H.; Kim, D.H.; Yang, H.S. Comparison of Clinical Efficacy Between Transforaminal and Interlaminar Epidural Injections in Lumbosacral Disc Herniation: A Systematic Review and Meta-Analysis. Pain Physician 2018, 21, 433–448. [Google Scholar] [CrossRef] [PubMed]
- Sencan, S.; Edipoglu, I.S.; Celenlioglu, A.E.; Yolcu, G.; Gunduz, O.H. Comparison of treatment outcomes in lumbar central stenosis patients treated with epidural steroid injections: Interlaminar versus bilateral transforaminal approach. Korean J. Pain 2020, 33, 226. [Google Scholar] [CrossRef]
- Scanlon, G.C.; Moeller-Bertram, T.; Romanowsky, S.M.; Wallace, M.S. Cervical transforaminal epidural steroid injections: More dangerous than we think? Spine 2007, 32, 1249–1256. [Google Scholar] [CrossRef]
- Horseheads, N.; Director, C.P.; Atluri, S. Needle position analysis in cases of paralysis from transforaminal epidurals: Consider alternative approaches to traditional technique. Pain Physician 2013, 16, 321–334. [Google Scholar]
- Ziai, W.C.; Ardelt, A.A.; Llinas, R.H. Brainstem stroke following uncomplicated cervical epidural steroid injection. Arch. Neurol. 2006, 63, 1643–1646. [Google Scholar] [CrossRef] [PubMed]
- Aprill, C.N.; Dumitrescu, M. Adverse central nervous system sequelae after selective transforaminal block: The role of corticosteroids. Spine J. 2005, 5, 475. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Chae, K.W.; Ju, C.I.; Kim, B.W. Acute cervical subdural hematoma with quadriparesis after cervical transforaminal epidural block. J. Korean Neurosurg. Soc. 2015, 58, 483. [Google Scholar] [CrossRef] [PubMed]
- MacMahon, P.; Shelly, M.; Scholz, D.; Eustace, S.; Kavanagh, E. Injectable corticosteroid preparations: An embolic risk assessment by static and dynamic microscopic analysis. AJNR Am. J. Neuroradiol. 2011, 32, 1830–1835. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.J.; Kim, D.H.; Han, W.K.; Lee, H.J.; Kang, I.; Nahm, F.S.; Lee, P.B. Non-Particulate Steroids (Betamethasone Sodium Phosphate, Dexamethasone Sodium Phosphate, and Dexamethasone Palmitate) Combined with Local Anaesthetics (Ropivacaine, Levobupivacaine, Bupivacaine, and Lidocaine): A Potentially Unsafe Mixture. J. Pain Res. 2021, 14, 1495. [Google Scholar] [CrossRef]
- Derby, R.; Lee, S.-H.; Date, E.S.; Lee, J.-H.; Lee, C.-H. Size and aggregation of corticosteroids used for epidural injections. Pain Med. 2008, 9, 227–234. [Google Scholar] [CrossRef]
- Capnogna, G.; Celleno, D.; Laudano, D.; Giunta, F. Alkalinization of local anaesthetics. Which block, which local anaesthetic. Reg. Anesth. 1995, 20, 369–377. [Google Scholar]
- Fulling, P.D.; Peterfreund, R.A. Alkalinization and precipitation characteristics of 0.2% ropivacaine. Reg. Anesth. Pain Med. 2000, 25, 518–521. [Google Scholar] [CrossRef]
- McLure, H.; Rubin, A. Review of local anaesthetic agents. Minerva Anestesiol. 2005, 71, 59–74. [Google Scholar]
- Chassard, D.; Berrada, K.; Bouletreau, P. Alkalinization of local anaesthetics: Theoretically justified but clinically useless. Can. J. Anaesth. 1996, 43, 384–393. [Google Scholar] [CrossRef] [Green Version]
- Milner, Q.; Guard, B.; Allen, J. Alkalinization of amide local anaesthetics by addition of 1% sodium bicarbonate solution. Eur. J. Anaesthesiol. 2000, 17, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Bigeleisen, P.; Wempe, M. Identification of the precipitate in alkalinized solutions of mepivacaine and bupivacaine at 37° C. J. Clin. Pharm. Ther. 2001, 26, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Kovacic, B.; Vrecer, F.; Planinsek, O. Spherical crystallization of drugs. Acta Pharm. 2012, 62, 1. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.; Park, J.; Lee, W.K.; Lee, W.H.; Leigh, J.H.; Lee, J.J.; Chung, S.G.; Lim, C.; Park, S.J.; Kim, K. Crystallization of local anaesthetics when mixed with corticosteroid solutions. Ann. Rehabil. Med. 2016, 40, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyoshi, M.; Imoto, T.; Hiji, Y. Alkalinizing water-soluble local anesthetic solutions by addition of cyclodextrin. Reg. Anesth. Pain Med. 1998, 23, 176–181. [Google Scholar] [CrossRef]
- Manchikanti, L.; Hirsch, J.A. Neurological complications associated with epidural steroid injections. Curr. Pain Headache Rep. 2015, 19, 10. [Google Scholar] [CrossRef]
- Kim, Y.D.; Moon, H.S. Review of medical dispute cases in the pain management in Korea: A medical malpractice liability insurance database study. Korean J. Pain 2015, 28, 254–264. [Google Scholar] [CrossRef]
- Rozin, L.; Rozin, R.; Koehler, S.A.; Shakir, A.; Ladham, S.; Barmada, M.; Dominick, J.; Wecht, C.H. Death during transforaminal epidural steroid nerve root block (C7) due to perforation of the left vertebral artery. Am. J. Forensic. Med. Pathol. 2003, 24, 351–355. [Google Scholar] [CrossRef]
- Wallace, M.A.; Fukui, M.B.; Williams, R.L.; Ku, A.; Baghai, P. Complications of cervical selective nerve root blocks performed with fluoroscopic guidance. AJR Am. J. Roentgenol. 2007, 188, 1218–1221. [Google Scholar] [CrossRef]
- Huntoon, M.A. Anatomy of the cervical intervertebral foramina: Vulnerable arteries and ischemic neurologic injuries after transforaminal epidural injections. Pain 2005, 117, 104–111. [Google Scholar] [CrossRef]
- Pasqualucci, A.; Varrassi, G.; Braschi, A.; Peduto, V.A.; Brunelli, A.; Marinangeli, F.; Gori, F.; Colò, F.; Paladini, A.; Mojoli, F. Epidural local anesthetic plus corticosteroid for the treatment of cervical brachial radicular pain: Single injection versus continuous infusion. Clin. J. Pain 2007, 23, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Marinangeli, F.; Ciccozzi, A.; Donatelli, F.; Paladini, A.; Varrassi, G. Clinical use of spinal or epidural steroids. Minerva Anestesiol. 2002, 68, 613–620. [Google Scholar] [PubMed]
- Kang, W.Y.; Lee, J.W.; Lee, E.; Kang, Y.; Ahn, J.M.; Kang, H.S. Systemic effects of fluoroscopically guided epidural steroid injection with dexamethasone. Korean J. Pain 2019, 32, 178–186. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Room Temperature (at 26 °C) | Body Temperature (at 36 °C) | With/Add Contrast Media at 26 °C | With/Add Contrast Media 36 °C | |
|---|---|---|---|---|
| 0.1% ropivacaine with dexamethasone | ++++ | clear | clear | + |
| 0.2% ropivacaine with dexamethasone | +++++ | + | clear | clear |
| Mixed Solutions | pH |
|---|---|
| 0.1% ropivacaine 1cc + dexamethasone 1cc (26 °C) | 7.51 |
| 0.1% ropivacaine 1cc + dexamethasone 1cc (36 °C) | 7.42 |
| 0.1% ropivacaine 1cc + dexamethasone 1cc + contrast media 1cc (26 °C) | 7.44 |
| 0.1% ropivacaine 1cc + dexamethasone 1cc + contrast media 1cc (36 °C) | 7.28 |
| 0.2% ropivacaine 1cc + dexamethasone 1cc (26 °C) | 7.42 |
| 0.2% ropivacaine 1cc + dexamethasone 1cc (36 °C) | 7.14 |
| 0.2% ropivacaine 1cc + dexamethasone 1cc + contrast media 1cc (26 °C) | 7.36 |
| 0.2% ropivacaine 1cc + dexamethasone 1cc + contrast media 1cc (36 °C) | 7.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.J.; Kim, Y.-D.; Kim, H.; Ahn, D.J.; Kim, H.-J.; Koh, W.U.; Ro, Y.-J. Interaction between Dexamethasone, Ropivacaine, and Contrast Media Used in Interventional Pain Treatment: Considerations in Safety. Medicina 2022, 58, 1871. https://doi.org/10.3390/medicina58121871
Kim YJ, Kim Y-D, Kim H, Ahn DJ, Kim H-J, Koh WU, Ro Y-J. Interaction between Dexamethasone, Ropivacaine, and Contrast Media Used in Interventional Pain Treatment: Considerations in Safety. Medicina. 2022; 58(12):1871. https://doi.org/10.3390/medicina58121871
Chicago/Turabian StyleKim, Yeon Ju, Yeon-Dong Kim, Hyungtae Kim, Dong Ji Ahn, Ha-Jung Kim, Won Uk Koh, and Young-Jin Ro. 2022. "Interaction between Dexamethasone, Ropivacaine, and Contrast Media Used in Interventional Pain Treatment: Considerations in Safety" Medicina 58, no. 12: 1871. https://doi.org/10.3390/medicina58121871