
Management of Complex Acetabular Fractures by Using 3D Printed Models


Abstract
:1. Introduction
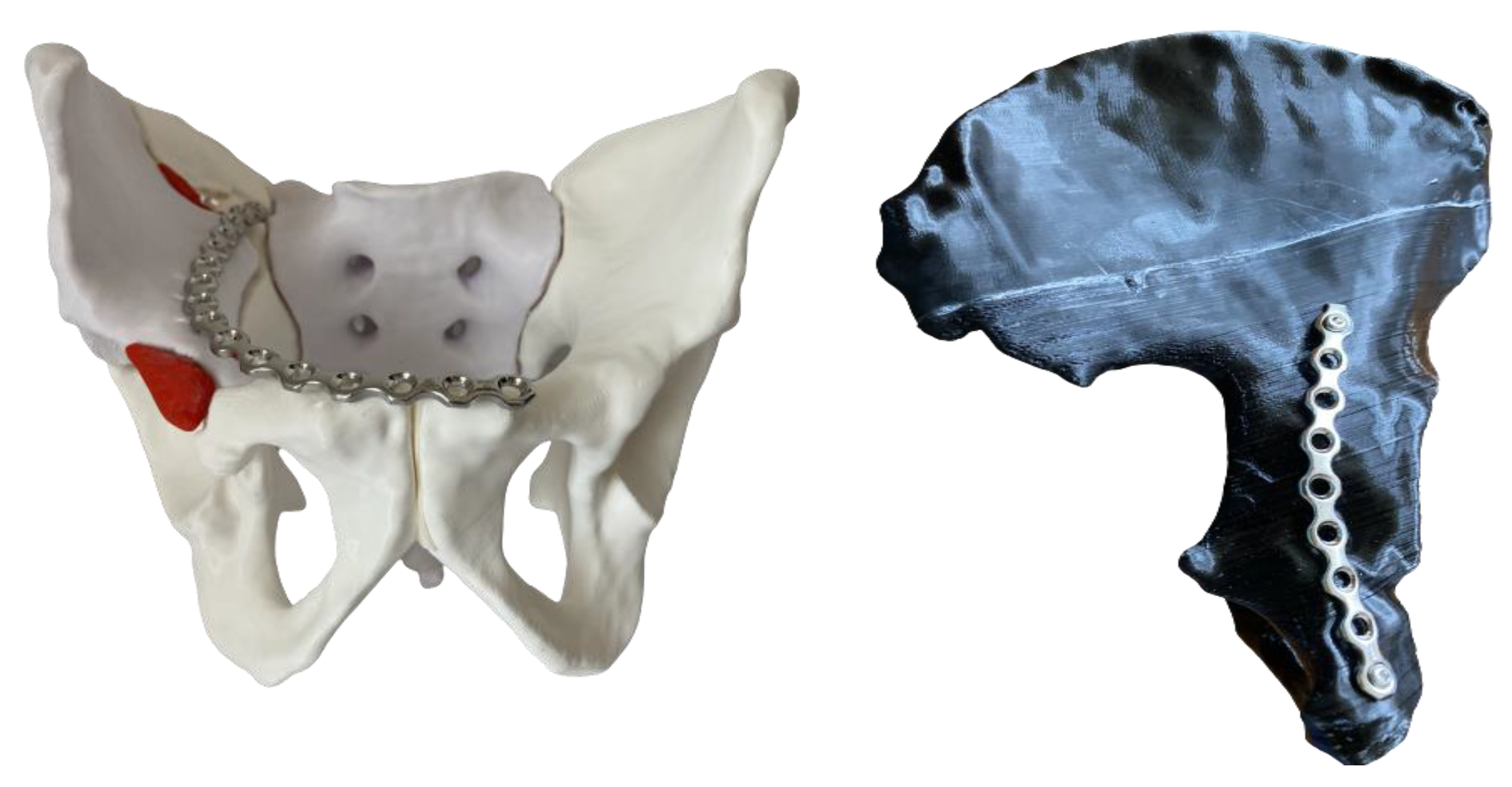
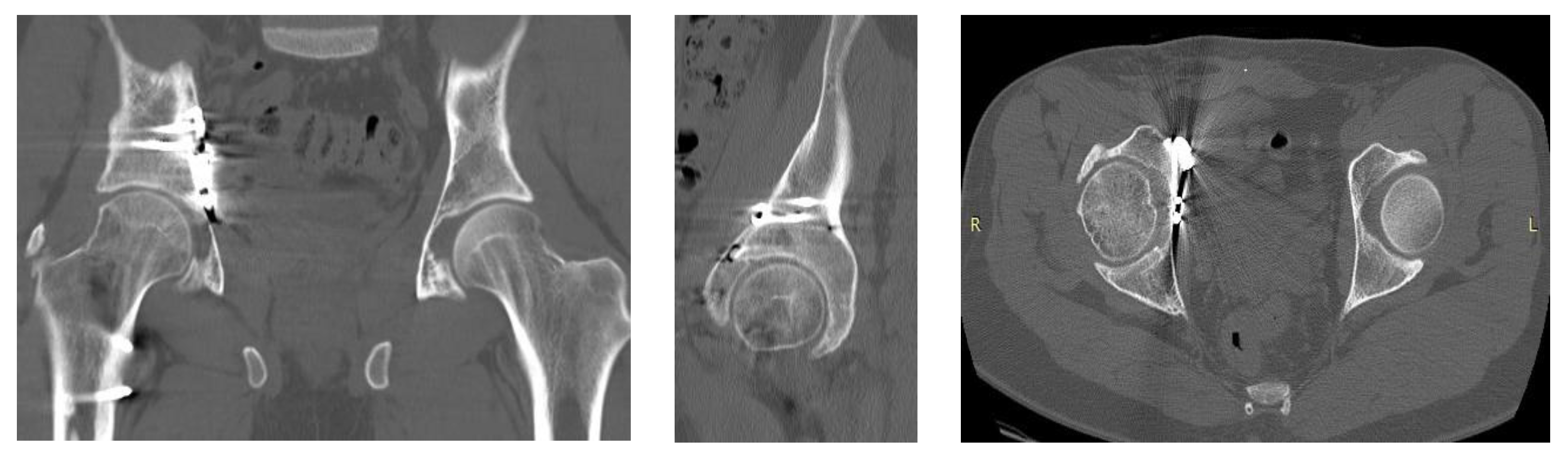
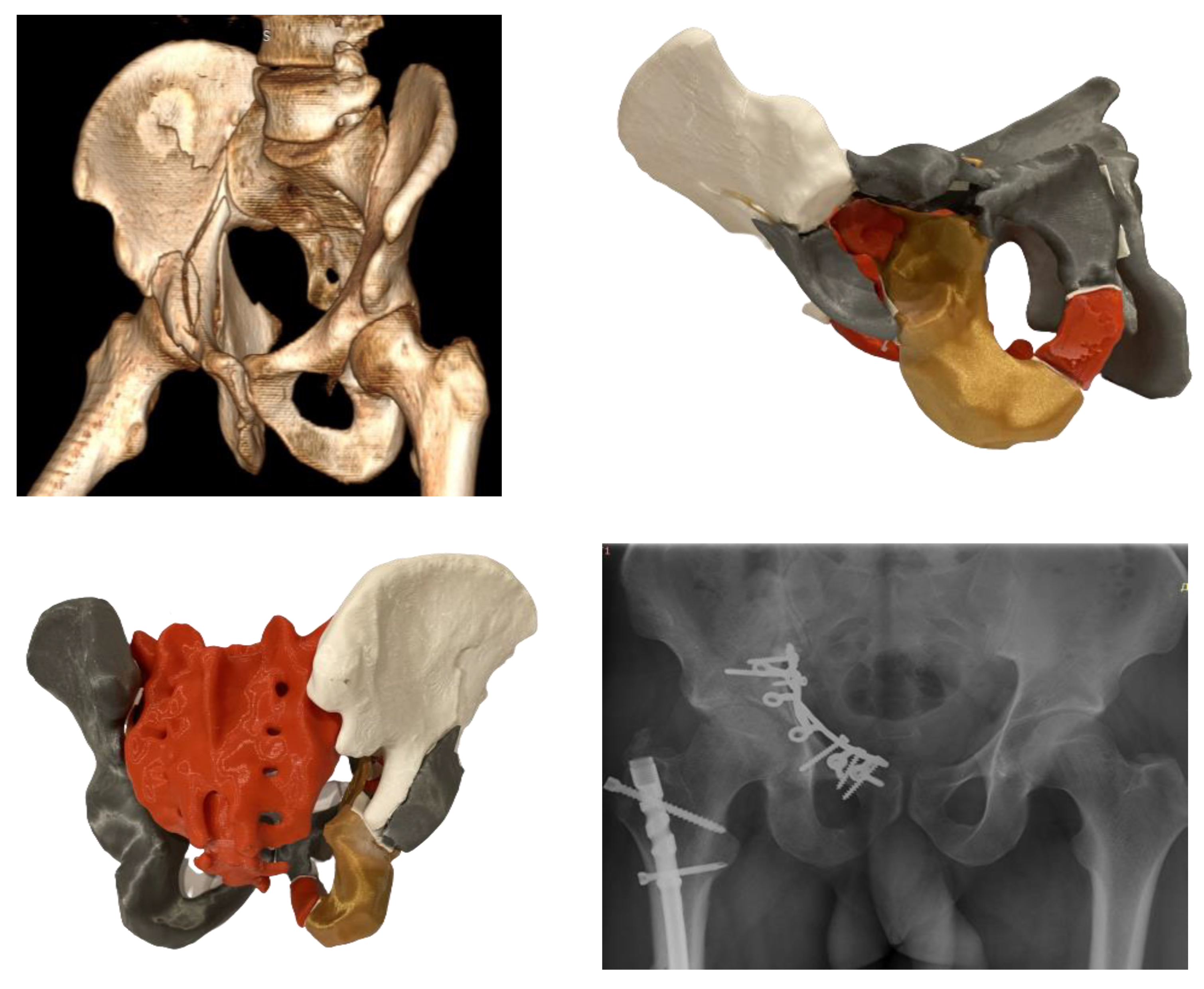
2. Materials and Methods
Technical Specifications
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rinne, P.P.; Laitinen, M.K.; Huttunen, T.; Kannus, P.; Mattila, V.M. The incidence and trauma mechanisms of acetabular fractures: A nationwide study in Finland between 1997 and 2014. Injury 2017, 48, 2157–2161. [Google Scholar] [CrossRef]
- Melhem, E.; Riouallon, G.; Habboubi, K.; Gabbas, M.; Jouffroy, P. Epidemiology of pelvic and acetabular fractures in France. Orthop. Traumatol. Surg. Res. 2020, 106, 831–839. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Grotz, M.R.W.; Papakostidis, C.; Dinopoulos, H. Operative treatment of displaced fractures of the acetabulum. J. Bone Jt. Surg. 2005, 87, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Hirvensalo, E.; Lindahl, J.; Kiljunen, V. Modified and new approaches for pelvic and acetabular surgery. Injury 2007, 38, 431–441. [Google Scholar] [CrossRef]
- Mears, D.C.; Velyvis, J.H.; Chang, C.-P. Displaced Acetabular Fractures Managed Operatively: Indicators of Outcome. Clin. Orthop. Relat. Res. 2003, 407, 173–186. [Google Scholar] [CrossRef]
- Beaulé, P.E.; Dorey, F.J.; Matta, J.M. Letournel classification for acetabular fractures. Assessment of interobserver and intraobserver reliability. J. Bone Jt. Surg. 2003, 85, 1704–1709. [Google Scholar] [CrossRef]
- Garrett, J.; Halvorson, J.; Carroll, E.; Webb, L.X. Value of 3-D CT in Classifying Acetabular Fractures During Orthopedic Residency Training. Orthopedics 2012, 35, e615–e620. [Google Scholar] [CrossRef] [Green Version]
- Cimerman, M.; Kristan, A. Preoperative planning in pelvic and acetabular surgery: The value of advanced computerised planning modules. Injury 2007, 38, 442–449. [Google Scholar] [CrossRef]
- Durkee, N.J.; Jacobson, J.; Jamadar, D.; Karunakar, M.A.; Morag, Y.; Hayes, C. Classification of Common Acetabular Fractures: Radiographic and CT Appearances. Am. J. Roentgenol. 2006, 187, 915–925. [Google Scholar] [CrossRef]
- Lal, H.; Patralekh, M.K. 3D printing and its applications in orthopaedic trauma: A technological marvel. J. Clin. Orthop. Trauma 2018, 9, 260–268. [Google Scholar] [CrossRef]
- Judet, R.; Judet, J.; Letournel, E. Fractures of the acetabulum: Classification and surgical approaches for open reduction. preliminary report. J. Bone Jt. Surgery. Am. 1964, 46, 1615–1646. [Google Scholar] [CrossRef]
- Alton, T.B.; Gee, A.O. Classifications in Brief: Letournel Classification for Acetabular Fractures. Clin. Orthop. Relat. Res. 2013, 472, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Autodesk Meshmixer. Available online: https://www.meshmixer.com (accessed on 11 December 2022).
- Prusa MK3S 3D Printer. Prusa Research. Available online: https://www.prusa3d.com/product/original-prusa-i3-mk3s-3d-printer-3 (accessed on 11 December 2022).
- Ansari, S.; Barik, S.; Singh, S.K.; Sarkar, B.; Goyal, T.; Kalia, R.B. Role of 3D printing in the management of complex acetabular fractures: A comparative study. Eur. J. Trauma Emerg. Surg. 2020, 47, 1291–1296. [Google Scholar] [CrossRef]
- Hung, C.-C.; Li, Y.-T.; Chou, Y.-C.; Chen, J.-E.; Wu, C.-C.; Shen, H.-C.; Yeh, T.-T. Conventional plate fixation method versus pre-operative virtual simulation and three-dimensional printing-assisted contoured plate fixation method in the treatment of anterior pelvic ring fracture. Int. Orthop. 2018, 43, 425–431. [Google Scholar] [CrossRef]
- Huang, J.-H.; Liao, H.; Tan, X.-Y.; Xing, W.-R.; Zhou, Q.; Zheng, Y.-S.; Cao, H.-Y.; Zeng, C.-J. Surgical treatment for both-column acetabular fractures using pre-operative virtual simulation and three-dimensional printing techniques. Chin. Med J. 2020, 133, 395–401. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Pohlemann, T.; Bircher, M. Pelvic and acetabular surgery within Europe: The need for the co-ordination of treatment concepts. Injury 2007, 38, 410–415. [Google Scholar] [CrossRef]
- Glas, P.Y.; Fessy, M.H.; Carret, J.P.; Béjui-Hugues, J. Surgical treatment of acetabular fractures: Outcome in a series of 60 consecutive cases. Rev. Chir. Orthopédique Réparatrice L’appareil Mot. 2001, 87, 529–538. [Google Scholar]
- Horas, K.; Hoffmann, R.; Faulenbach, M.; Heinz, S.M.; Langheinrich, A.; Schweigkofler, U. Advances in the Preoperative Planning of Revision Trauma Surgery Using 3D Printing Technology. J. Orthop. Trauma 2020, 34, e181–e186. [Google Scholar] [CrossRef]
- Preece, D.; Williams, S.B.; Lam, R.; Weller, R. Let’s Get Physical: Advantages of a physical model over 3D computer models and textbooks in learning imaging anatomy. Anat. Sci. Educ. 2013, 6, 216–224. [Google Scholar] [CrossRef]
- Fang, C.; Cai, H.; Kuong, E.; Chui, E.; Siu, Y.C.; Ji, T.; Drstvenšek, I. Surgical applications of three-dimensional printing in the pelvis and acetabulum: From models and tools to implants. Der Unfallchirurg 2019, 122, 278–285. [Google Scholar] [CrossRef]
- Valchanov, P.S. 3D Printing in medicine—Principles, applications and challenges. Scr. Sci. Vox Stud. 2017, 1, 18–22. [Google Scholar] [CrossRef]
- Brouwers, L.; Pull Ter Gunne, A.F.; De Jongh, M.A.C.; Van Der Heijden, F.H.W.M.; Leenen, L.P.H.; Spanjersberg, W.R.; Van Helden, S.H.; Verbeek, D.O.; Bemelman, M.; Lansink, K.W.W. The Value of 3D Printed Models in Understanding Acetabular Fractures. 3D Print. Addit. Manuf. 2018, 5, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Hansen, E.; Marmor, M.; Matityahu, A. Impact of a Three-Dimensional “Hands-On” Anatomic Teaching Module on Acetabular Fracture Pattern Recognition by Orthopaedic Residents. J. Bone Jt. Surg. 2012, 94, e177. [Google Scholar] [CrossRef]
- Manganaro, M.S.; Morag, Y.; Weadock, W.J.; Yablon, C.M.; Gaetke-Udager, K.; Stein, E.B. Creating Three-dimensional Printed Models of Acetabular Fractures for Use as Educational Tools. RadioGraphics 2017, 37, 871–880. [Google Scholar] [CrossRef]
- Yu, A.W.; Duncan, J.M.; Daurka, J.S.; Lewis, A.; Cobb, J. A Feasibility Study into the Use of Three-Dimensional Printer Modelling in Acetabular Fracture Surgery. Adv. Orthop. 2015, 2015, 617046. [Google Scholar] [CrossRef]
- Niikura, T.; Sugimoto, M.; Lee, S.Y.; Sakai, Y.; Nishida, K.; Kuroda, R.; Kurosaka, M. Tactile Surgical Navigation System for Complex Acetabular Fracture Surgery. Orthopedics 2014, 37, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.K.-X.; Lin, T.-L.; Hsu, C.-J.; Fong, Y.-C.; Chen, H.-T.; Tsai, C.-H. Three-Dimensional Printing and Fracture Mapping in Pelvic and Acetabular Fractures: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 5258. [Google Scholar] [CrossRef]
- Cao, J.; Zhu, H.; Gao, C. A Systematic Review and Meta-Analysis of 3D Printing Technology for the Treatment of Acetabular Fractures. BioMed Res. Int. 2021, 2021, 1–15. [Google Scholar] [CrossRef]
- Øvre, S.; Sandvik, L.; Madsen, J.E.; Røise, O. Comparison of distribution, agreement and correlation between the original and modified Merle d’Aubigné-Postel Score and the Harris Hip Score after acetabular fracture treatment: Moderate agreement, high ceiling effect and excellent correlation in 450 patients. Acta Orthop. 2005, 76, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Matta, J.M.; Mehne, D.K.; Roffi, R. Fractures of the acetabulum. Early results of a prospective study. Clin. Orthop. Relat. Res. 1986, 205, 241–250. [Google Scholar] [CrossRef]
- Zhang, Y.-D.; Wu, R.-Y.; Xie, D.-D.; Zhang, L.; He, Y.; Zhang, H. Effect of 3D printing technology on pelvic fractures: A Meta-analysis. Zhongguo Gu Shang 2018, 31, 465–471. [Google Scholar] [CrossRef]
- Öztürk, A.M.; Süer, O.; Şirintürk, S.; Aktuğlu, K.; Govsa, F.; Özer, M.A. A retrospective comparison of the conventional versus three-dimensional printed model-assisted surgery in the treatment of acetabular fractures. Acta Orthop. Traumatol. Turc. 2020, 54, 385–393. [Google Scholar] [CrossRef]
- Wang, C.; Chen, Y.; Wang, L.; Wang, D.; Gu, C.; Lin, X.; Liu, H.; Chen, J.; Wen, X.; Liu, Y.; et al. Three-dimensional printing of patient-specific plates for the treatment of acetabular fractures involving quadrilateral plate disruption. BMC Musculoskelet. Disord. 2020, 21, 451. [Google Scholar] [CrossRef]
- Wan, L.; Zhang, X.; Zhang, S.; Li, K.; Cao, P.; Li, J.; Wu, G. Clinical feasibility and application value of computer virtual reduction combined with 3D printing technique in complex acetabular fractures. Exp. Ther. Med. 2019, 17, 3630–3636. [Google Scholar] [CrossRef] [Green Version]
- Downey, C.; McCarrick, C.; Fenelon, C.; Murphy, E.P.; O’Daly, B.J.; Leonard, M. A novel approach using 3-D printing in the Irish National Centre for pelvic and acetabular surgery. Ir. J. Med Sci. 2019, 189, 219–228. [Google Scholar] [CrossRef]
- Li, Y.-T.; Hung, C.-C.; Chou, Y.-C.; Chen, J.-E.; Wu, C.-C.; Shen, H.-C.; Yeh, T.-T. Surgical Treatment for Posterior Dislocation of Hip Combined with Acetabular Fractures Using Preoperative Virtual Simulation and Three-Dimensional Printing Model-Assisted Precontoured Plate Fixation Techniques. BioMed Res. Int. 2019, 2019, 3971571. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Oh, H. The submuscular sliding plate technique for acetabular posterior wall fractures extending to the acetabular roof. Orthop. Traumatol. Surg. Res. 2014, 100, 967–970. [Google Scholar] [CrossRef] [Green Version]
- Elmadağ, M.; Güzel, Y.; Acar, M.; Uzer, G.; Arazi, M. The Stoppa approach versus the ilioinguinal approach for anterior acetabular fractures: A case control study assessing blood loss complications and function outcomes. Orthop. Traumatol. Surg. Res. 2014, 100, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Upex, P.; Jouffroy, P.; Riouallon, G. Application of 3D printing for treating fractures of both columns of the acetabulum: Benefit of pre-contouring plates on the mirrored healthy pelvis. Orthop. Traumatol. Surg. Res. 2017, 103, 331–334. [Google Scholar] [CrossRef]
- De Franco, C.; Colò, G.; Melato, M.; Battini, A.; Cambursano, S.; Logrieco, G.P.; Balato, G.; Zoccola, K. Fracture-Related Infection in Bicolumnar Acetabular Fracture: A Case Report. Diagnostics 2022, 12, 2476. [Google Scholar] [CrossRef]
- Chepelev, L.; Wake, N.; Ryan, J.; Althobaity, W.; Gupta, A.; Arribas, E.; Santiago, L.; Ballard, D.H.; Wang, K.C.; Weadock, W.; et al. Radiological Society of North America (RSNA) 3D printing Special Interest Group (SIG): Guidelines for medical 3D printing and appropriateness for clinical scenarios. 3D Print. Med. 2018, 4, 1–38. [Google Scholar] [CrossRef]
- Brouwers, L.; Teutelink, A.; van Tilborg, F.A.J.B.; de Jongh, M.A.C.; Lansink, K.W.W.; Bemelman, M. Validation study of 3D-printed anatomical models using 2 PLA printers for preoperative planning in trauma surgery, a human cadaver study. Eur. J. Trauma Emerg. Surg. 2018, 45, 1013–1020. [Google Scholar] [CrossRef]
- Kanters, D.; de Vries, A.; Boon, H.; Urbach, J.; Becht, A.; Kooistra, H.-A. Quality Assurance in Medical 3D-Printing. IFMBE Proc. 2018, 68, 669–674. [Google Scholar] [CrossRef]
- Odeh, M.; Levin, D.; Inziello, J.; Fenoglietto, F.L.; Mathur, M.; Hermsen, J.; Stubbs, J.; Ripley, B. Methods for verification of 3D printed anatomic model accuracy using cardiac models as an example. 3D Print. Med. 2019, 5, 6–12. [Google Scholar] [CrossRef]
- Kannus, P.; Palvanen, M.; Niemi, S.; Parkkari, J.; Järvinen, M. Epidemiology of Osteoporotic Pelvic Fractures in Elderly People in Finland: Sharp Increase in 1970-1997 and Alarming Projections for the New Millennium. Osteoporos. Int. 2000, 11, 443–448. [Google Scholar] [CrossRef]
- Brouwers, L.; ter Gunne, A.F.P.; de Jongh, M.A.; Maal, T.J.J.; Vreeken, R.; van der Heijden, F.H.W.M.; Leenen, L.P.H.; Spanjersberg, W.R.; van Helden, S.H.; Verbeek, D.O.; et al. What is the value of 3D virtual reality in understanding acetabular fractures? Eur. J. Orthop. Surg. Traumatol. 2019, 30, 109–116. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group | p-Value | |
|---|---|---|---|
| Conventional | 3D Printed | ||
| Gender | 10 m/2 f | 9 m/2 f | 0.65 |
| Fracture I | 6 | 5 | 0.93 |
| Fracture II | 2 | 2 | 0.94 |
| Fracture III | 4 | 3 | 0.93 |
| Parameter | Group | Mean | SD | Median | Range | p-Value |
|---|---|---|---|---|---|---|
| Patents age (years) | 1 | 50.9 | 11.6 | 54 | 27–65 | 0.74 |
| 2 | 49.1 | 12.2 | 54 | 26–64 | ||
| Time from injury to operation (days) | 1 | 7.5 | 2.4 | 7 | 5–8 | 0.89 |
| 2 | 7.8 | 2.8 | 7 | 5–9 | ||
| Operative time (min) | 1 | 252.5 | 30.2 | 240 | 220–300 | <0.01 |
| 2 | 193.5 | 26.0 | 195 | 160–240 | ||
| Blood loss (mL) | 1 | 837.5 | 68.0 | 835 | 780–980 | <0.01 |
| 2 | 665.0 | 52.7 | 690 | 580–720 | ||
| Intraoperative x-rays | 1 | 66.5 | 6.7 | 65 | 58–80 | <0.01 |
| 2 | 25.9 | 5.6 | 24.5 | 20–36 | ||
| Follow-up (months) | 1 | 17.6 | 0.7 | 18 | 17–19 | 0.78 |
| 2 | 17.1 | 5.2 | 17 | 8–24 | ||
| Modified Merle d’Aubigné–Postel score at follow-up | 1 | 13.1 | 1.7 | 14 | 10–15 | 0.03 |
| 2 | 14.7 | 1.6 | 15 | 12–17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivanov, S.; Valchanov, P.; Hristov, S.; Veselinov, D.; Gueorguiev, B. Management of Complex Acetabular Fractures by Using 3D Printed Models. Medicina 2022, 58, 1854. https://doi.org/10.3390/medicina58121854
Ivanov S, Valchanov P, Hristov S, Veselinov D, Gueorguiev B. Management of Complex Acetabular Fractures by Using 3D Printed Models. Medicina. 2022; 58(12):1854. https://doi.org/10.3390/medicina58121854
Chicago/Turabian StyleIvanov, Stoyan, Petar Valchanov, Stoyan Hristov, Deyan Veselinov, and Boyko Gueorguiev. 2022. "Management of Complex Acetabular Fractures by Using 3D Printed Models" Medicina 58, no. 12: 1854. https://doi.org/10.3390/medicina58121854