
The Efficacy of Urinary Continence in Patients Undergoing Robot-Assisted Radical Prostatectomy with Bladder-Prostatic Muscle Reconstruction and Bladder Neck Eversion Anastomosis
Abstract
:1. Background
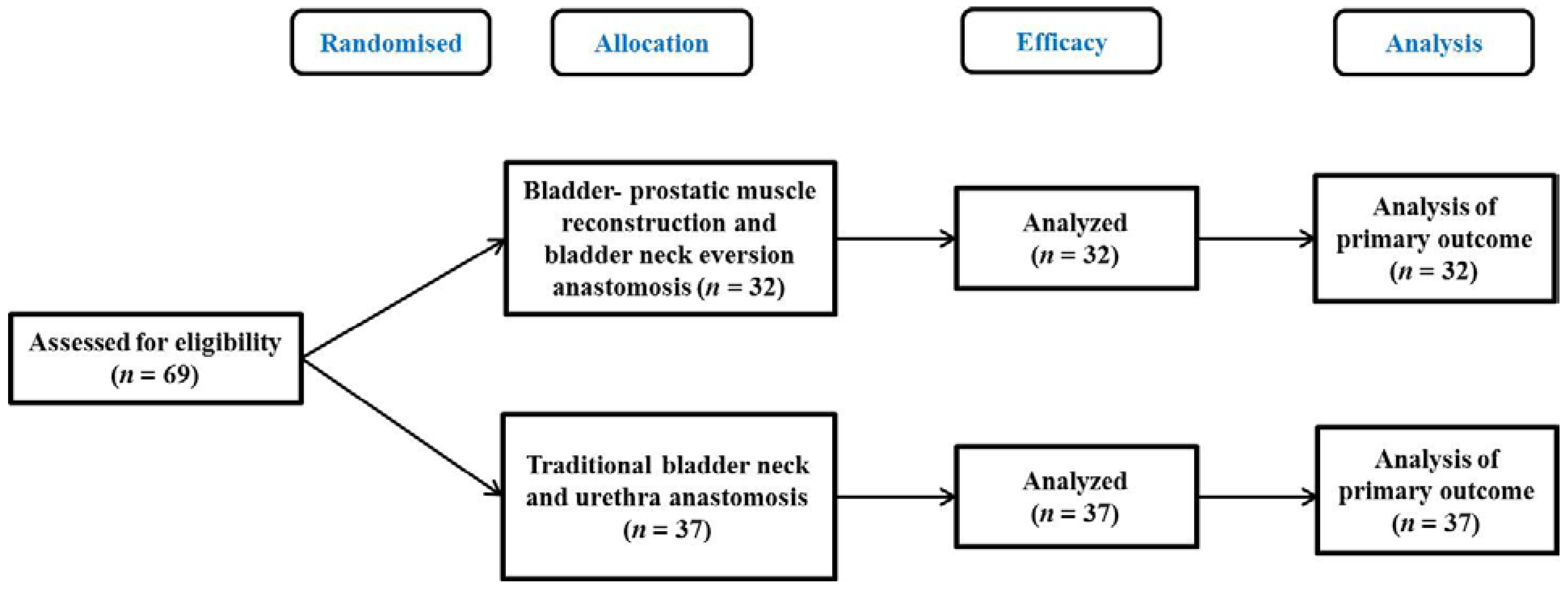
2. Methods
2.1. Clinical Data
2.2. Surgical Technique
3. Statistical Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Sun, K.; Zheng, R.; Zeng, H.; Zhang, S.; Xia, C.; Yang, Z.; Li, H.; Zou, X.; He, J. Cancer incidence and mortality in China, 2014. Chin. J. Cancer Res. 2018, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, S.A.; Cowan, J.E.; Lonergan, P.E.; Washington, S.L.; Nguyen, H.G.; Zagoria, R.J.; Carroll, P.R. The effect of preoperative membranous urethral length on likelihood of postoperative urinary incontinence after robot-assisted radical prostatectomy. Prostate Cancer Prostatic Dis. 2022, 25, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Kawabata, H.; Deguchi, R.; Ueda, Y.; Higuchi, M.; Muraoka, S.; Koike, H.; Kikkawa, K.; Kohjimoto, Y.; Hara, I. Myosteatosis as a novel predictor of urinary incontinence after robot-assisted radical prostatectomy. Int. J. Urol. 2022, 29, 34–40. [Google Scholar] [CrossRef]
- Xu, B.; Cheng, S.-D.; Peng, Y.-J.; Zhang, Q. Comparison of functional and oncological outcomes of innovative “three-port” and traditional “four-port” laparoscopic radical prostatectomy in patients with prostate cancer. BMC Urol. 2021, 21, 21. [Google Scholar] [CrossRef]
- Chung, J.H.; Kwon, T.G.; Kwak, C.; Sung, G.T.; Kim, S.D.; Cho, J.S.; Kim, H.J.; Ahn, H.; Jeon, S.S. Efficacy and Safety of Udenafil Once Daily in Patients with Erectile Dysfunction after Bilateral Nerve-Sparing Robot-Assisted Laparoscopic Radical Prostatectomy: A Randomized, Double-Blind, Placebo-Controlled Study. World J. Men’s Health 2022, 40, e62. [Google Scholar] [CrossRef]
- Strojek, K.; Weber-Rajek, M.; Strączyńska, A.; Piekorz, Z.; Pilarska, B.; Jarzemski, P.; Kozakiewicz, M.; Brzoszczyk, B.; Jarzemski, M.; Styczyńska, H.; et al. Randomized-Controlled Trial Examining the Effect of Pelvic Floor Muscle Training in the Treatment of Stress Urinary Incontinence in Men after a Laparoscopic Radical Prostatectomy Pilot Study. J. Clin. Med. 2021, 10, 2946. [Google Scholar] [CrossRef]
- Novara, G.; Ficarra, V.; Mocellin, S.; Ahlering, T.E.; Carroll, P.R.; Graefen, M.; Guazzoni, G.; Menon, M.; Patel, V.R.; Shariat, S.F.; et al. Systematic Review and Meta-analysis of Studies Reporting Oncologic Outcome After Robot-assisted Radical Prostatectomy. Eur. Urol. 2012, 62, 382–404. [Google Scholar] [CrossRef]
- Stolzenburg, J.-U.; Holze, S.; Arthanareeswaran, V.-K.; Neuhaus, P.; Do, H.M.; Haney, C.M.; Dietel, A.; Truss, M.C.; Stützel, K.D.; Teber, D.; et al. Robotic-assisted versus Laparoscopic Radical Prostatectomy: 12-month Outcomes of the Multicentre Randomised Controlled LAP-01 Trial. Eur. Urol. Focus 2022. [CrossRef]
- Holze, S.; Lemaire, E.; Mende, M.; Neuhaus, P.; Arthanareeswaran, V.; Truss, M.C.; Do, H.M.; Dietel, A.; Teber, D.; Stützel, K.D.; et al. Quality of life after robotic-assisted and laparoscopic radical prostatectomy: Results of a multicenter randomized controlled trial (LAP-01). Prostate 2022, 82, 894–903. [Google Scholar] [CrossRef]
- Yaxley, J.W.; Coughlin, G.; Patel, V. Level 1 Evidence of Better Early Urinary Continence at 3 Months Following Robot-assisted Laparoscopic Radical Prostatectomy Compared with Laparoscopic Radical Prostatectomy. Results of the LAP-01 Randomised Controlled Trial. Eur. Urol. 2021, 79, 760–761. [Google Scholar] [CrossRef] [PubMed]
- Savera, A.T.; Kaul, S.; Badani, K.; Stark, A.T.; Shah, N.L.; Menon, M. Robotic Radical Prostatectomy with the “Veil of Aphrodite” Technique: Histologic Evidence of Enhanced Nerve Sparing. Eur. Urol. 2006, 49, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Choinière, R.; Violette, P.D.; Morin, M.; Tu, L.M.; Guyatt, G.H.; Reed, C.; Philie, C.-A.; Legault, B.; Beaudry, M.-M.; Ahmed, M.M.; et al. Evaluation of Benefits and Harms of Surgical Treatments for Post–radical Prostatectomy Urinary Incontinence: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2022, 8, 1042–1052. [Google Scholar] [CrossRef] [PubMed]
- Parry, M.G.; Skolarus, T.A.; Nossiter, J.; Sujenthiran, A.; Morris, M.; Cowling, T.E.; Berry, B.; Aggarwal, A.; Payne, H.; Cathcart, P.; et al. Urinary incontinence and use of incontinence surgery after radical prostatectomy: A national study using patient-reported outcomes. BJU Int. 2022, 130, 84–91. [Google Scholar] [CrossRef]
- Del Giudice, F.; Huang, J.; Li, S.; Sorensen, S.; Enemchukwu, E.; Maggi, M.; Salciccia, S.; Ferro, M.; Crocetto, F.; Pandolfo, S.D.; et al. Contemporary trends in the surgical management of urinary incontinence after radical prostatectomy in the United States. Prostate Cancer Prostatic Dis. 2022. [CrossRef]
- Salomon, L.; Saint, F.; Anastasiadis, A.G.; Sebe, P.; Chopin, D.; Abbou, C.-C. Combined Reporting of Cancer Control and Functional Results of Radical Prostatectomy. Eur. Urol. 2003, 44, 656–660. [Google Scholar] [CrossRef]
- Inoue, S.; Hieda, K.; Hayashi, T.; Teishima, J.; Matsubara, A. Longitudinal analysis of trifecta outcome in Japanese patients with prostate cancer following robot-assisted laparoscopic radical prostatectomy. World J. Urol. 2022, 40, 2009–2015. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, J.; Yang, Z.; Liu, Q.; Zhang, W.; Qing, Z.; Wang, D. Comparison of Retzius-sparing and conventional robot-assisted laparoscopic radical prostatectomy regarding continence and sexual function: An updated meta-analysis. Prostate Cancer Prostatic Dis. 2022, 25, 47–54. [Google Scholar] [CrossRef]
- Galfano, A.; Ascione, A.; Grimaldi, S.; Petralia, G.; Strada, E.; Bocciardi, A.M. A New Anatomic Approach for Robot-Assisted Laparoscopic Prostatectomy: A Feasibility Study for Completely Intrafascial Surgery. Eur. Urol. 2010, 58, 457–461. [Google Scholar] [CrossRef]
- Ma, H.; Qiu, X.; Xu, L.; Gan, W.; Zhang, G.; Li, X.; Guo, H. A comparative study between Retzius-sparing robot-assisted laparoscopic radical prostatectomy and conventional robot-assisted laparoscopic radical prostatectomy. Chin. J. Urol. 2018, 039, 509–514. [Google Scholar]
- Dalela, D.; Jeong, W.; Prasad, M.-A.; Sood, A.; Abdollah, F.; Diaz, M.; Karabon, P.; Sammon, J.; Jamil, M.; Baize, B.; et al. A Pragmatic Randomized Controlled Trial Examining the Impact of the Retzius-sparing Approach on Early Urinary Continence Recovery After Robot-assisted Radical Prostatectomy. Eur. Urol. 2017, 72, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Cadeddu, J.A. Re: A Pragmatic Randomized Controlled Trial Examining the Impact of the Retzius-Sparing Approach on Early Urinary Continence Recovery after Robot-Assisted Radical Prostatectomy. J. Urol. 2018, 199, 875–876. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.K.; Kim, K.H.; Shin, T.-Y.; Han, W.K.; Chung, B.H.; Hong, S.J.; Choi, Y.D.; Rha, K.H. Retzius-sparing robot-assisted laparoscopic radical prostatectomy: Combining the best of retropubic and perineal approaches. BJU Int. 2014, 114, 236–244. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, D.K.; Ahn, H.K.; Jung, H.D.; Lee, J.Y.; Cho, K.S. Effect of Bladder Neck Preservation on Long-Term Urinary Continence after Robot-Assisted Laparoscopic Prostatectomy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 2068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, S.; Ak, E.; Gazel, E.; Yalcin, S.; Yildiz, K.Y.; Tunc, L. Bladder neck sparing during robot-assisted laparoscopic radical prostatectomy: Six-year experience. North. Clin. Istanb. 2021, 8, 269–274. [Google Scholar]
- Wiatr, T.; Choragwicki, D.; Gronostaj, K.; Czech, A.; Przydacz, M.; Chlosta, M.; Belch, L.; Dudek, P.; Curylo, L.; Zembrzuski, M.; et al. Long-term functional outcomes of vesicourethral anastomosis with bladder neck preservation and distal urethral length preservation after videolaparoscopic radical prostatectomy. Videosurg. Other Miniinvasive Tech. 2022, 17, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Tolkach, Y.; Godin, K.; Petrov, S.; Schelin, S.; Imkamp, F. A new technique of bladder neck reconstruction during radical prostatectomy in patients with prostate cancer. Int. Braz. J. Urol. 2015, 41, 455–465. [Google Scholar] [CrossRef] [Green Version]
- Coelho, R.F.; Chauhan, S.; Orvieto, M.A.; Sivaraman, A.; Palmer, K.J.; Coughlin, G.; Patel, V.R. Influence of Modified Posterior Reconstruction of the Rhabdosphincter on Early Recovery of Continence and Anastomotic Leakage Rates after Robot-Assisted Radical Prostatectomy. Eur. Urol. 2011, 59, 72–80. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; Jung, J.H.; Edgerton, Z.; Lee, H.; Lee, S.; Bakker, C.J.; Dahm, P. Retzius-sparing versus standard robot-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer. BJU Int. 2021, 128, 12–20. [Google Scholar] [CrossRef]
- Deng, W.; Zhang, C.; Jiang, H.; Li, Y.; Zhu, K.; Liu, X.; Chen, L.; Liu, W.; Guo, J.; Zhou, X.; et al. Transvesical Versus Posterior Approach to Retzius-Sparing Robot-Assisted Radical Prostatectomy: A Retrospective Comparison with a 12-Month Follow-Up. Front. Oncol. 2021, 11, 641887. [Google Scholar] [CrossRef]
- Asimakopoulos, A.D.; Topazio, L.; De Angelis, M.; Agrò, E.F.; Pastore, A.L.; Fuschi, A.; Annino, F. Retzius-sparing versus standard robot-assisted radical prostatectomy: A prospective randomized comparison on immediate continence rates. Surg. Endosc. 2019, 33, 2187–2196. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Observation Group | Control Group | p-Value |
|---|---|---|---|
| Age (Years) | 67.53 ± 4.76 | 65.72 ± 6.31 | 0.189 |
| BMI (kg/m2) | 24.15 ± 3.21 | 25.17 ± 3.44 | 0.210 |
| Prostate volume (mL) | 40.19 ± 14.15 | 38.54 ± 16.36 | 0.658 |
| PSA(ng/mL) | 17.12 ± 12.37 | 19.14 ± 9.69 | 0.450 |
| Gleason score [n (%)] | 0.893 | ||
| 6 | 8 (25.00) | 9 (24.32) | |
| 7 | 15 (46.88) | 20 (54.05) | |
| 8 | 6 (18.75) | 6 (16.21) | |
| ≥9 | 3 (9.38) | 2 (5.41) |
| Groups | Observation Group | Control Group | p-Value |
|---|---|---|---|
| Operative time (min) | 127.76 ± 21.23 | 118.85 ± 24.71 | 0.116 |
| Blood loss (mL) | 118.27 ± 16.75 | 110.77 ± 19.63 | 0.095 |
| Rate of leakage (%) | 3.13 (1/32) | 2.70 (1/37) | 0.917 |
| Rate of positive surgical margin (%) | 6.25 (2/32) | 10.81 (4/37) | 0.498 |
| Postoperative Gleason score [n (%)] | 0.943 | ||
| 6 | 7 (21.88) | 8 (21.62) | |
| 7 | 14 (43.75) | 17 (45.95) | |
| 8 | 7 (21.88) | 9 (24.32) | |
| ≥9 | 4 (12.50) | 3 (8.11) | |
| Urinary continence rates [n (%)] | 0.034 | ||
| 24 h | 15 (46.88) | 8 (21.62) | 0.026 |
| 1 week | 22 (68.75) | 14 (37.84) | 0.010 |
| 4 weeks | 27 (84.38) | 23 (62.16) | 0.039 |
| 12 weeks | 29 (90.63) | 32 (86.49) | 0.874 |
| 24 weeks | 30 (93.75) | 34 (91.89) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luan, Y.; Ding, X.-F.; Lu, S.-M.; Huang, T.-B.; Chen, J.; Xiao, Q.; Wang, L.-P.; Chen, H.-P.; Han, Y.-X. The Efficacy of Urinary Continence in Patients Undergoing Robot-Assisted Radical Prostatectomy with Bladder-Prostatic Muscle Reconstruction and Bladder Neck Eversion Anastomosis. Medicina 2022, 58, 1821. https://doi.org/10.3390/medicina58121821
Luan Y, Ding X-F, Lu S-M, Huang T-B, Chen J, Xiao Q, Wang L-P, Chen H-P, Han Y-X. The Efficacy of Urinary Continence in Patients Undergoing Robot-Assisted Radical Prostatectomy with Bladder-Prostatic Muscle Reconstruction and Bladder Neck Eversion Anastomosis. Medicina. 2022; 58(12):1821. https://doi.org/10.3390/medicina58121821
Chicago/Turabian StyleLuan, Yang, Xue-Fei Ding, Sheng-Ming Lu, Tian-Bao Huang, Ji Chen, Qin Xiao, Li-Ping Wang, Hao-Peng Chen, and Yue-Xing Han. 2022. "The Efficacy of Urinary Continence in Patients Undergoing Robot-Assisted Radical Prostatectomy with Bladder-Prostatic Muscle Reconstruction and Bladder Neck Eversion Anastomosis" Medicina 58, no. 12: 1821. https://doi.org/10.3390/medicina58121821