
Safety and Efficacy of Simultaneous Resection of Gastric Carcinoma and Synchronous Liver Metastasis—A Western Center Experience
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Patient Selection
2.2. Surgical and Oncologic Management
2.3. Ethics
2.4. Statistical Analysis
3. Results
3.1. Clinico-Pathological Characteristics
3.2. Surgical Data
3.3. Short-Term Outcomes
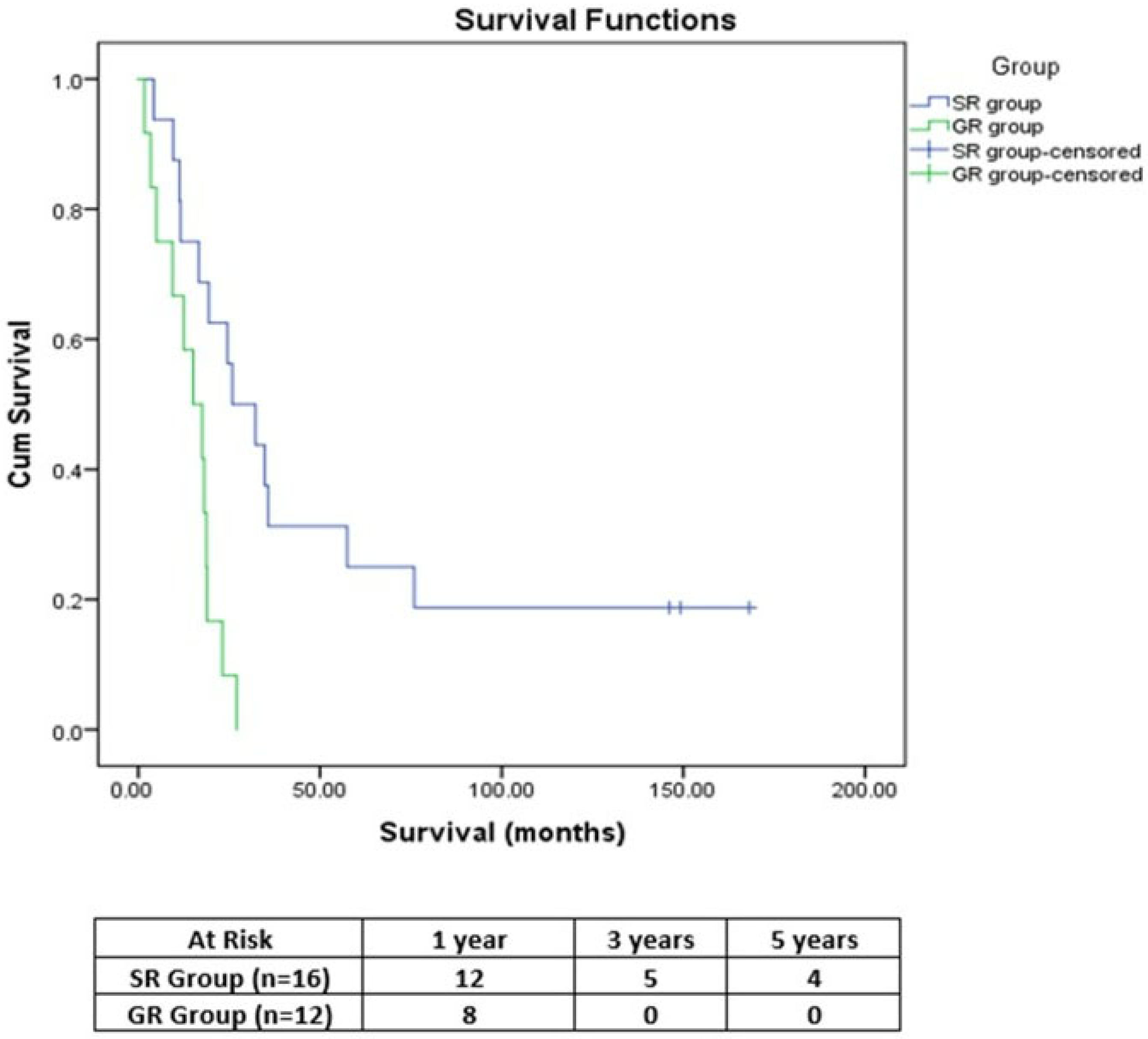
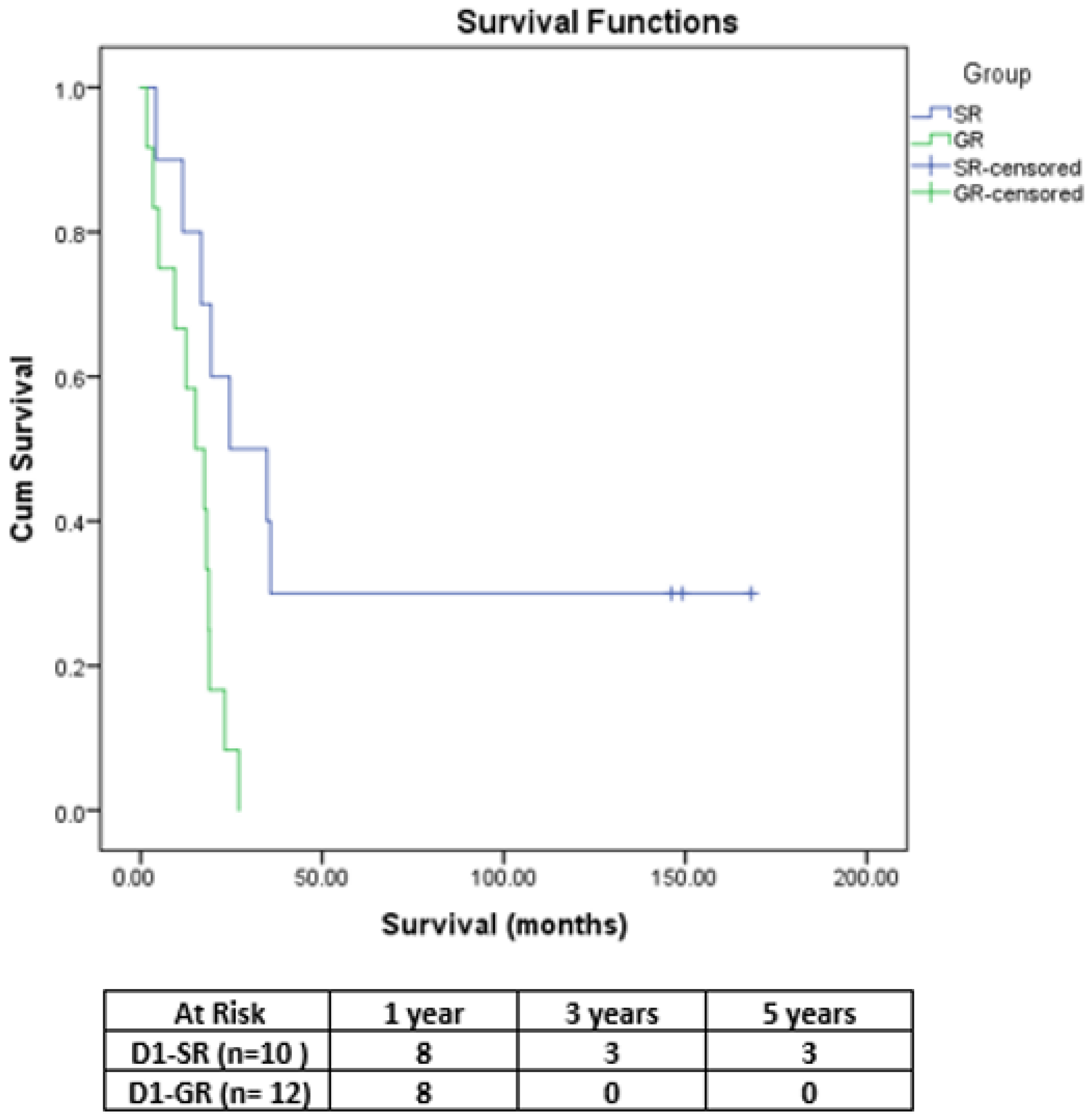
3.4. Overall Survival (OS)
3.5. Univariate Analysis
3.6. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ECOG | Eastern Cooperative Oncology Group |
| ESMO | European Society for Medical Oncology |
| GC | gastric cancer |
| GR | gastric resection |
| LM | liver metastasis |
| LMGC | gastric cancer with liver metastasis |
| NCCN | National Comprehensive Cancer Network |
| SD | standard deviation |
| SR | synchronous resection |
References
- Uggeri, F.; Ripamonti, L.; Pinotti, E.; Scotti, M.A.; Famularo, S.; Garancini, M.; Gianotti, L.; Braga, M.; Romano, F. Is there a role for treatment-oriented surgery in liver metastases from gastric cancer? World J. Clin. Oncol. 2020, 11, 477–494. [Google Scholar] [CrossRef] [PubMed]
- Qiu, M.Z.; Shi, S.M.; Chen, Z.H.; Yu, H.E.; Sheng, H.; Jin, Y.; Wang, D.S.; Wang, F.H.; Li, Y.H.; Xie, D.; et al. Frequency and clinicopathological features of metastasis to liver, lung, bone, and brain from gastric cancer: A SEER-based study. Cancer Med. 2018, 7, 3662–3672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, A.; Zhang, X.; Yu, F.; Li, D.; Shao, W.; Zhou, Y. Surgical resection for hepatic metastasis from gastric cancer: A multi-institution study. Oncotarget 2017, 8, 71147–71153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granieri, S.; Altomare, M.; Bruno, F.; Paleino, S.; Bonomi, A.; Germini, A.; Facciorusso, A.; Fagnani, D.; Bovo, G.; Cotsoglou, C. Surgical treatment of gastric cancer liver metastases: Systematic review and meta-analysis of long-term outcomes and prognostic factors. Crit. Rev. Oncol./Hematol. 2021, 163, 103313. [Google Scholar] [CrossRef]
- Schildberg, C.W.; Croner, R.; Merkel, S.; Schellerer, V.; Müller, V.; Yedibela, S.; Hohenberger, W.; Peros, G.; Perrakis, A. Outcome of operative therapy of hepatic metastatic stomach carcinoma: A retrospective analysis. World J. Surg. 2012, 36, 872–878. [Google Scholar] [CrossRef]
- Kinoshita, T.; Kinoshita, T.; Saiura, A.; Esaki, M.; Sakamoto, H.; Yamanaka, T. Multicentre analysis of long-term outcome after surgical resection for gastric cancer liver metastases. Br. J. Surg. 2015, 102, 102–107. [Google Scholar] [CrossRef]
- Guckenberger, M.; Lievens, Y.; Bouma, A.B.; Collette, L.; Dekker, A.; deSouza, N.M.; Dingemans, A.C.; Fournier, B.; Hurkmans, C.; Frédéric E Lecouvet, F.E.; et al. Characterisation and classification of oligometastatic disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation. Lancet Oncol. 2020, 21, e18–e28. [Google Scholar] [CrossRef] [Green Version]
- Kroese, T.E.; van Laarhoven, H.W.M.; Nilsson, M.; Lordick, F.; Guckenberger, M.; Ruurda, J.P.; D’Ugo, D.; Haustermans, K.; van Cutsem, E.; van Hillegersberg, R.; et al. Definition of oligometastatic esophagogastric cancer and impact of local oligometastasis-directed treatment: A systematic review and meta-analysis. Eur. J. Cancer 2022, 166, 254–269. [Google Scholar] [CrossRef]
- Casella, F.; Bencivenga, M.; Rosati, R.; Fumagalli, U.R.; Marrelli, D.; Pacelli, F.; Macrì, A.; Donini, A.; Torroni, L.; Pavarana, M.; et al. Pressurized intraperitoneal aerosol chemotherapy (PIPAC) in multimodal therapy for patients with oligometastatic peritoneal gastric cancer: A randomized multicenter phase III trial PIPAC VEROne. Pleura Peritoneum 2022, 7, 135–141. [Google Scholar] [CrossRef]
- Ajani, J.A.; D’Amico, T.A.; Bentrem, D.J.; Chao, J.; Cooke, D.; Corvera, C.; Das, P.; Enzinger, P.C.; Enzler, T.; Fanta, P.; et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 167–192. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef] [PubMed]
- Glimelius, B.; Ekström, K.; Hoffman, K.; Graf, W.; Sjödén, P.O.; Haglund, U.; Svensson, C.; Enander, L.K.; Linné, T.; Sellström, H.; et al. Randomized comparison between chemotherapy plus best supportive care with best supportive care in advanced gastric cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 1997, 8, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Marte, G.; Tufo, A.; Steccanella, F.; Marra, E.; Federico, P.; Petrillo, A.; Maida, P. Efficacy of Surgery for the Treatment of Gastric Cancer Liver Metastases: A Systematic Review of the Literature and Meta-Analysis of Prognostic Factors. J. Clin. Med. 2021, 10, 1141. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Song, M.Q.; Lin, H.Z.; Hao, L.H.; Jiang, X.J.; Li, Z.Y.; Chen, Y.X. Chemotherapy and resection for gastric cancer with synchronous liver metastases. World J. Gastroenterol. 2013, 19, 2097–2103. [Google Scholar] [CrossRef] [PubMed]
- Oki, E.; Tokunaga, S.; Emi, Y.; Kusumoto, T.; Yamamoto, M.; Fukuzawa, K.; Takahashi, I.; Ishigami, S.; Tsuji, A.; Higashi, H.; et al. Surgical treatment of liver metastasis of gastric cancer: A retrospective multicenter cohort study (KSCC1302). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2016, 19, 968–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2021, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.-H.; Shen, L.; Li, J.; Zhou, Z.-W.; Liang, H.; Zhang, X.-T.; Tang, L.; Xin, Y.; Jin, J.; Zhang, Y.-J.; et al. The Chinese Society of Clinical Oncology (CSCO): Clinical guidelines for the diagnosis and treatment of gastric cancer. Cancer Commun. 2019, 39, 10. [Google Scholar] [CrossRef] [Green Version]
- Muro, K.; Van Cutsem, E.; Narita, Y.; Pentheroudakis, G.; Baba, E.; Li, J.; Ryu, M.H.; Zamaniah, W.I.W.; Yong, W.P.; Yeh, K.H.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic gastric cancer: A JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 19–33. [Google Scholar] [CrossRef]
- Zhang, K.; Chen, L. Chinese consensus on the diagnosis and treatment of gastric cancer with liver metastases. Ther. Adv. Med. Oncol. 2020, 12, 1758835920904803. [Google Scholar] [CrossRef] [Green Version]
- Fujitani, K.; Yang, H.K.; Mizusawa, J.; Kim, Y.W.; Terashima, M.; Han, S.U.; Iwasaki, Y.; Hyung, W.J.; Takagane, A.; Park, D.J.; et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): A phase 3, randomised controlled trial. Lancet Oncol. 2016, 17, 309–318. [Google Scholar] [CrossRef]
- Thelen, A.; Jonas, S.; Benckert, C.; Lopez-Hänninen, E.; Neumann, U.; Rudolph, B.; Schumacher, G.; Neuhaus, P. Liver resection for metastatic gastric cancer. Eur. J. Surg. Oncol. 2008, 34, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Picado, O.; Dygert, L.; Macedo, F.I.; Franceschi, D.; Sleeman, D.; Livingstone, A.S.; Merchant, N.; Yakoub, D. The Role of Surgical Resection for Stage IV Gastric Cancer with Synchronous Hepatic Metastasis. J. Surg. Res. 2018, 232, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.R.; Mikhail, S.; Malietzis, G.; Athanasiou, T.; Mariette, C.; Sasako, M.; Hanna, G.B. Influence of Surgical Resection of Hepatic Metastases From Gastric Adenocarcinoma on Long-term Survival: Systematic Review and Pooled Analysis. Ann. Surg. 2016, 263, 1092–1101. [Google Scholar] [CrossRef]
- Gavriilidis, P.; Roberts, K.J.; de’Angelis, N.; Sutcliffe, R.P. Gastrectomy Alone or in Combination With Hepatic Resection in the Management of Liver Metastases from Gastric Cancer: A Systematic Review Using an Updated and Cumulative Meta-Analysis. J. Clin. Med. Res. 2019, 11, 600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garancini, M.; Uggeri, F.; Degrate, L.; Nespoli, L.; Gianotti, L.; Nespoli, A.; Uggeri, F.; Romano, F. Surgical treatment of liver metastases of gastric cancer: Is local treatment in a systemic disease worthwhile? HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2012, 14, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Markar, S.R.; Mackenzie, H.; Mikhail, S.; Mughal, M.; Preston, S.R.; Maynard, N.D.; Faiz, O.; Hanna, G.B. Surgical resection of hepatic metastases from gastric cancer: Outcomes from national series in England. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 379–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirabe, K.; Wakiyama, S.; Gion, T.; Watanabe, M.; Miyazaki, M.; Yoshinaga, K.; Tokunaga, M.; Nagaie, T. Hepatic resection for the treatment of liver metastases in gastric carcinoma: Review of the literature. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2006, 8, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Ng, K.K.C.; Cheng, N.M.Y.; Lok, H.-T.; Kung, J.W.C.; Fung, A.K.Y.; Chan, S.L. Is hepatic resection justified for non-colorectal non-neuroendocrine liver metastases? A systematic review and meta-analysis. Surgeon, 2022; in press. [Google Scholar] [CrossRef]
- Cui, J.-K.; Liu, M.; Shang, X.-K. Hepatectomy for Liver Metastasis of Gastric Cancer: A Meta-Analysis. Surg. Innov. 2019, 26, 692–697. [Google Scholar] [CrossRef]
- Ministrini, S.; Solaini, L.; Cipollari, C.; Sofia, S.; Marino, E.; D’Ignazio, A.; Bencivenga, M.; Tiberio, G.A.M. Surgical treatment of hepatic metastases from gastric cancer. Updat. Surg. 2018, 70, 273–278. [Google Scholar] [CrossRef]
- Jagric, T.; Horvat, M. Surgical resection of synchronous liver metastases in gastric cancer patients. A propensity score-matched study. Radiol. Oncol. 2020, 55, 57–65. [Google Scholar] [CrossRef]
- Yu, P.; Zhang, Y.; Ye, Z.; Chen, X.; Huang, L.; Du, Y.; Cheng, X. Treatment of Synchronous Liver Metastases from Gastric Cancer: A Single-Center Study. Cancer Manag. Res. 2020, 12, 7905–7911. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Kinoshita, T.; Moehler, M.; Mauer, M.; Shitara, K.; Wagner, A.D.; Schrauwen, S.; Yoshikawa, T.; Roviello, F.; Tokunaga, M.; et al. Current management of liver metastases from gastric cancer: What is common practice? New challenge of EORTC and JCOG. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 904–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viganò, L.; Vellone, M.; Ferrero, A.; Giuliante, F.; Nuzzo, G.; Capussotti, L. Liver resection for gastric cancer metastases. Hepato-Gastroenterol. 2013, 60, 557–562. [Google Scholar] [CrossRef]
- Zacherl, J.; Zacherl, M.; Scheuba, C.; Steininger, R.; Wenzl, E.; Mühlbacher, F.; Jakesz, R.; Längle, F. Analysis of hepatic resection of metastasis originating from gastric adenocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2002, 6, 682–689. [Google Scholar] [CrossRef]
- Yamashita, K.; Hosoda, K.; Niihara, M.; Hiki, N. History and emerging trends in chemotherapy for gastric cancer. Ann. Gastroenterol. Surg. 2021, 5, 446–456. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Comparative Descriptive Statistics | ||||
|---|---|---|---|---|
| Group | ||||
| SR | GR | p Value * | ||
| Count (%) | Count (%) | |||
| Gender | Female | 5 (31%) | 2 (17%) | 0.661 |
| Male | 11 (69%) | 10 (83%) | ||
| Age | <65 years | 7 (43%) | 5 (42%) | 0.912 |
| ≥65 years | 9 (57%) | 7 (58%) | ||
| T | T2 | 2 (14%) | 1 (9%) | 0.491 |
| T3 | 12 (86%) | 9 (82%) | ||
| T4a | - | 1 (9%) | ||
| Missing | 2 | 1 | ||
| N | N0 | 3 (21%) | 3 (30%) | 0.665 |
| N+ | 11 (79%) | 7 (70%) | ||
| Missing | 2 | 2 | ||
| Tumor site | Vertical part | 12 (75%) | 5 (42%) | 0.121 |
| Gastric antrum | 4 (25%) | 7 (58%) | ||
| Gastric Resection type | Total gastrectomy | 10 (63%) | 4 (33%) | - |
| Partial gastrectomy | 6 (37%) | 8 (67%) | 0.251 | |
| Number of liver metastases | 1 | 11 (69%) | 4 (33%) | 0.143 |
| 2 | 4 (25%) | 5 (42%) | ||
| 3 | 1 (6%) | 3 (25%) | ||
| Maximum diameter of liver metastases | ≤3 cm | 12 (75%) | 7 (58.3%) | 0.432 |
| >3 cm | 4 (25%) | 5 (41.7%) | ||
| Lymphadenectomy type | D1 | 10 (63%) | 12 (100%) | 0.024 |
| D2 | 6 (37%) | 0 (0%) | ||
| G grade | 1 | 4 (28%) | 2 (18%) | 0.809 |
| 2 | 5 (36%) | 5 (46%) | ||
| 3 | 5 (36%) | 4 (36%) | ||
| Missing | 2 | 1 | ||
| Dindo-Clavien grade of postoperative complications | 0 | 9 (56%) | 10 (83%) | 0.115 |
| I | 5 (32%) | 0 | ||
| II | 1 (6%) | 2 (17%) | ||
| IIIb | 1 (6%) | 0 | ||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| T T2 T3 T4a | 1 1.93 2.94 | 0.446–8.351 0.251–34.379 | 0.379 0.390 | |||
| N N0 N+ | 1 0.839 | 0.323–2.184 | 0.719 | |||
| Gender Female Male | 1 1.021 | 0.407–2.562 | 0.964 | |||
| Age <65 ≥65 | 1 1.395 | 0.622–3.130 | 0.419 | |||
| Primary Tumor Site Vertical Part Gastric antrum | 1 2.070 | 0.868–4.939 | 0.101 | 1 1.360 | 0.378–4.898 | 0.638 |
| Maximum size of LMGC ≤3 cm >3 cm | 1 2.190 | 0.916–5.239 | 0.078 | 1 1.550 | 0.609–3.947 | 0.358 |
| Number of Liver Metastasis 1 2 and 3 | 1 1.325 | 0.600–2.926 | 0.486 | |||
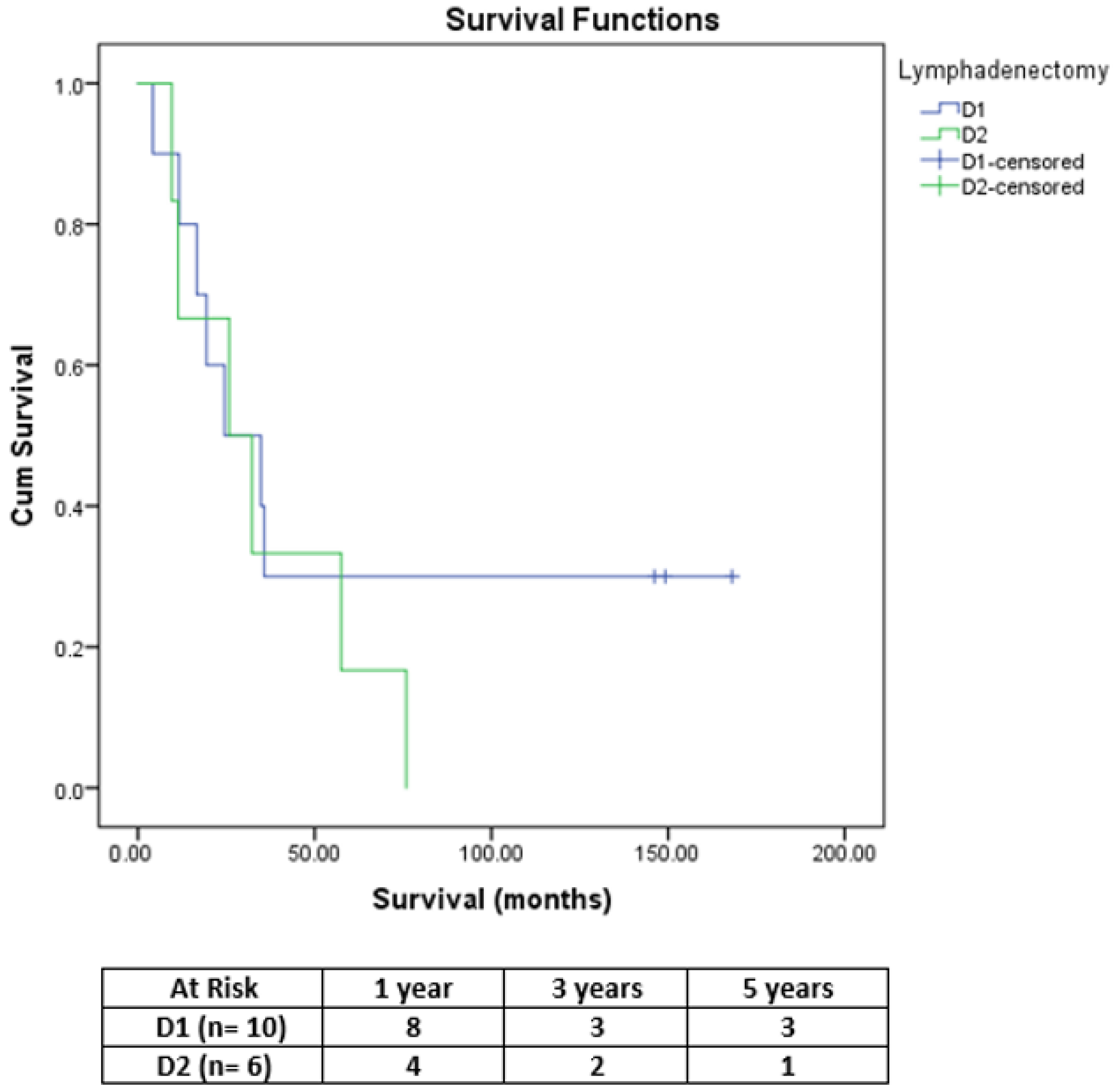
| Lymphadenectomy D1 D2 | 1 0.827 | 0.328–2.089 | 0.688 | |||
| G grade G1 G2 G3 | 1 2.184 0.801 | 0.735–6.488 0.253–2.539 | 0.160 0.706 | |||
| Group SR vs. GR SR GR | 1 3.954 | 1.542–10.139 | 0.002 | 1 3.954 | 1.542–10.139 | 0.004 |
| Postoperative complications 0 1 | 1 1.266 | 0.542–2.959 | 0.585 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minciuna, C.-E.; Tudor, S.; Micu, A.; Diaconescu, A.; Alexandrescu, S.T.; Vasilescu, C. Safety and Efficacy of Simultaneous Resection of Gastric Carcinoma and Synchronous Liver Metastasis—A Western Center Experience. Medicina 2022, 58, 1802. https://doi.org/10.3390/medicina58121802
Minciuna C-E, Tudor S, Micu A, Diaconescu A, Alexandrescu ST, Vasilescu C. Safety and Efficacy of Simultaneous Resection of Gastric Carcinoma and Synchronous Liver Metastasis—A Western Center Experience. Medicina. 2022; 58(12):1802. https://doi.org/10.3390/medicina58121802
Chicago/Turabian StyleMinciuna, Corina-Elena, Stefan Tudor, Alexandru Micu, Andrei Diaconescu, Sorin Tiberiu Alexandrescu, and Catalin Vasilescu. 2022. "Safety and Efficacy of Simultaneous Resection of Gastric Carcinoma and Synchronous Liver Metastasis—A Western Center Experience" Medicina 58, no. 12: 1802. https://doi.org/10.3390/medicina58121802