

Evaluation of the Sensitivity of Selected Candida Strains to Ozonated Water—An In Vitro Study
 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
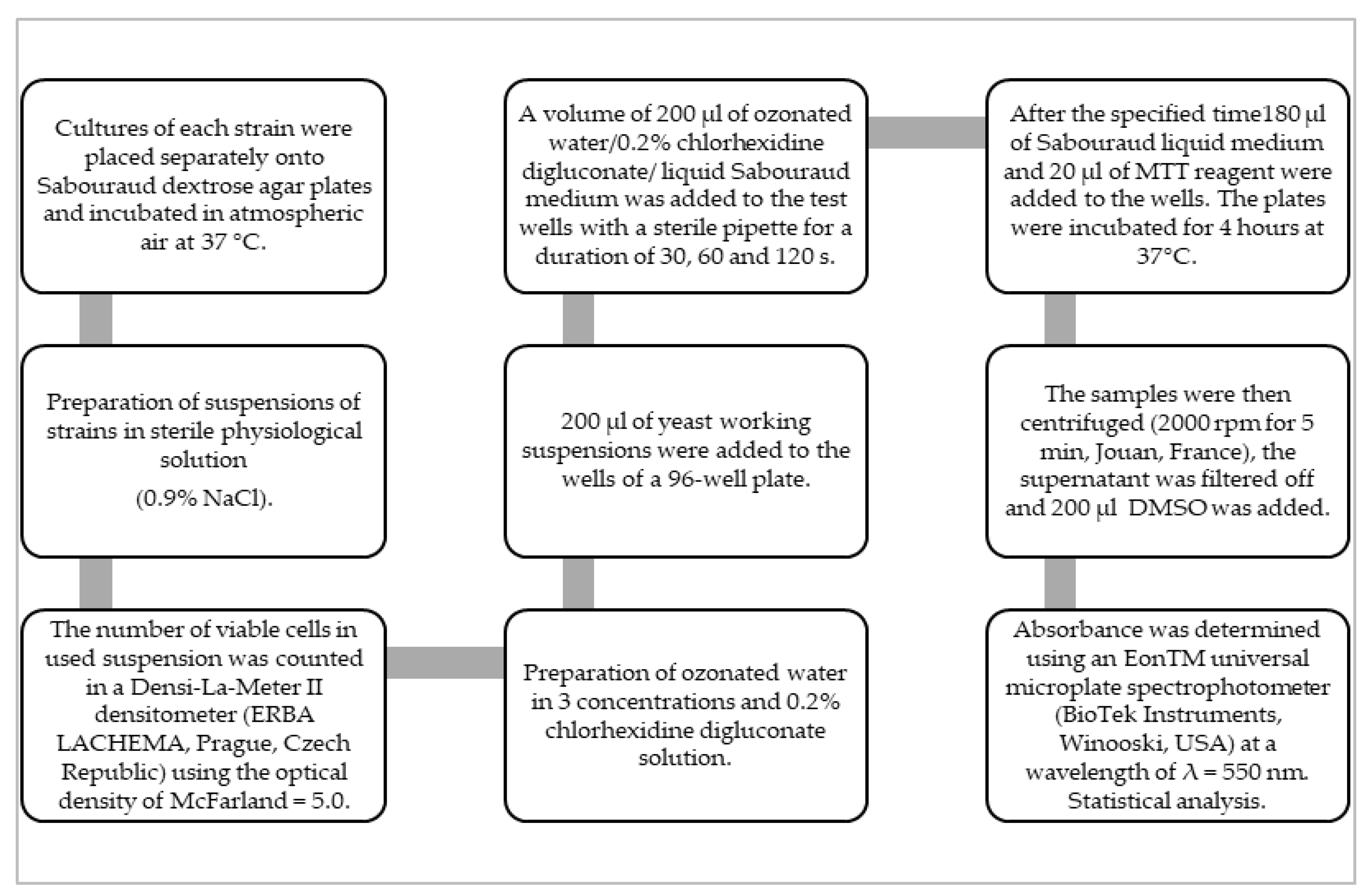
2. Materials and Methods
2.1. Organisms and Growth Conditions
2.2. Ozone Water
2.3. Chlorhexidine Digluconate
2.4. MTT Assay Protocol
2.5. Experimental Groups and Inactivation of Candida spp. In Vitro
2.6. Statistical Analysis
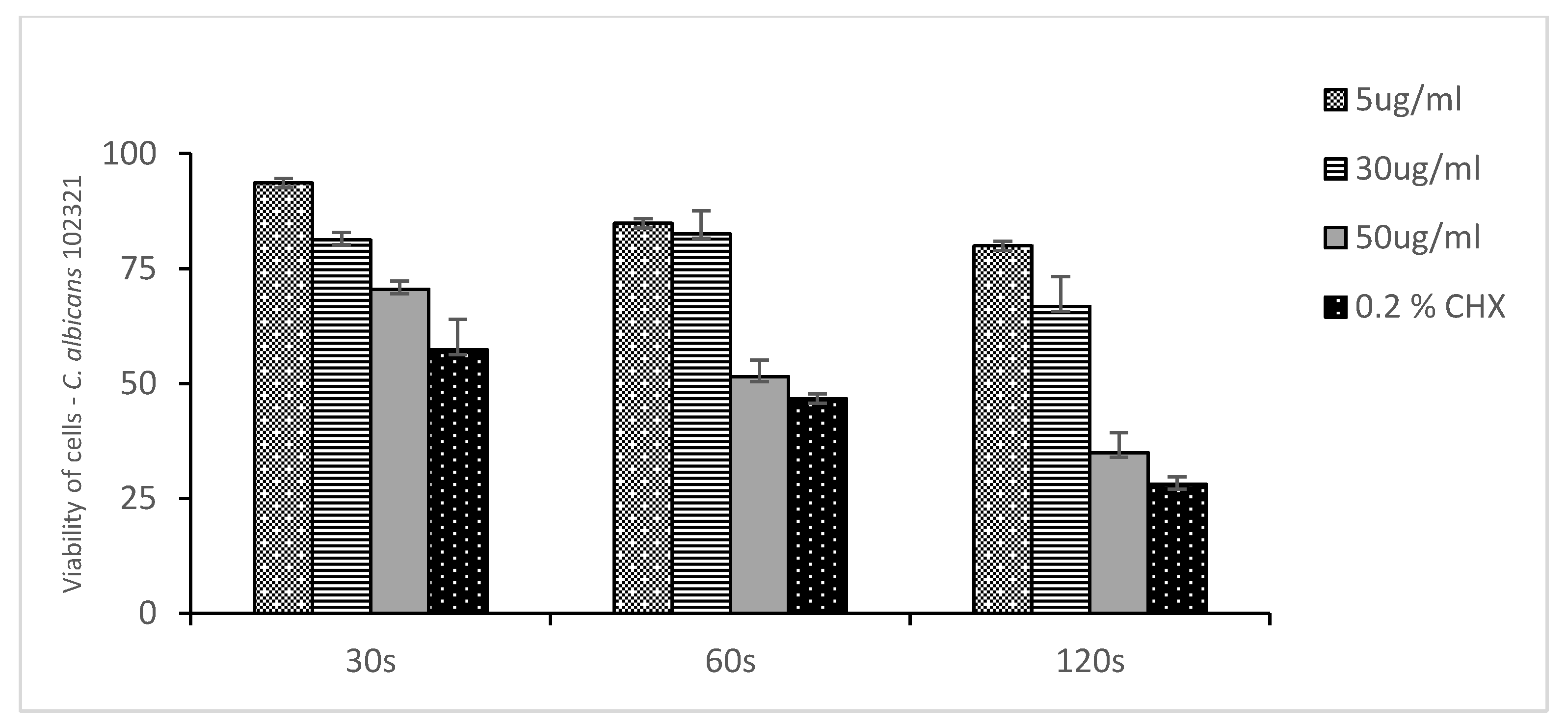
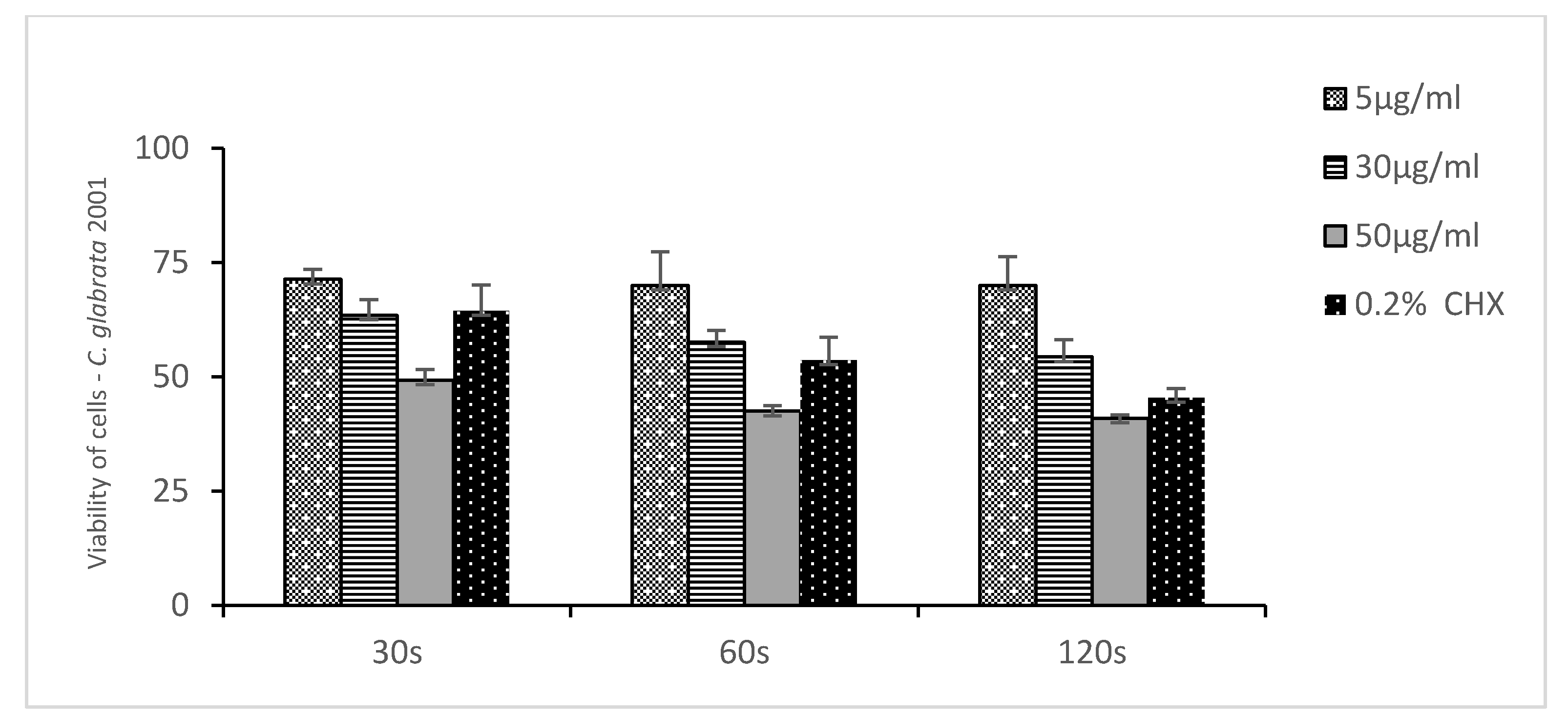
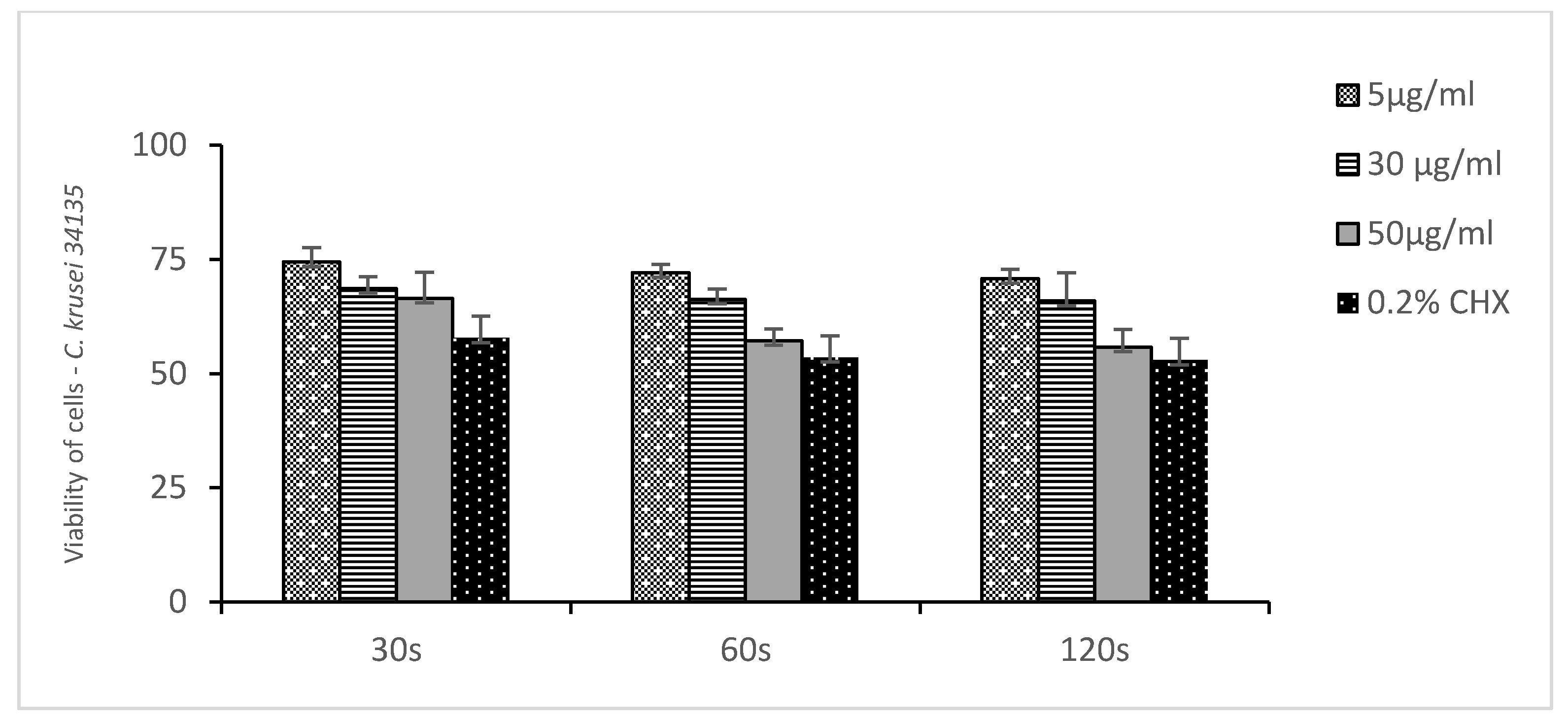
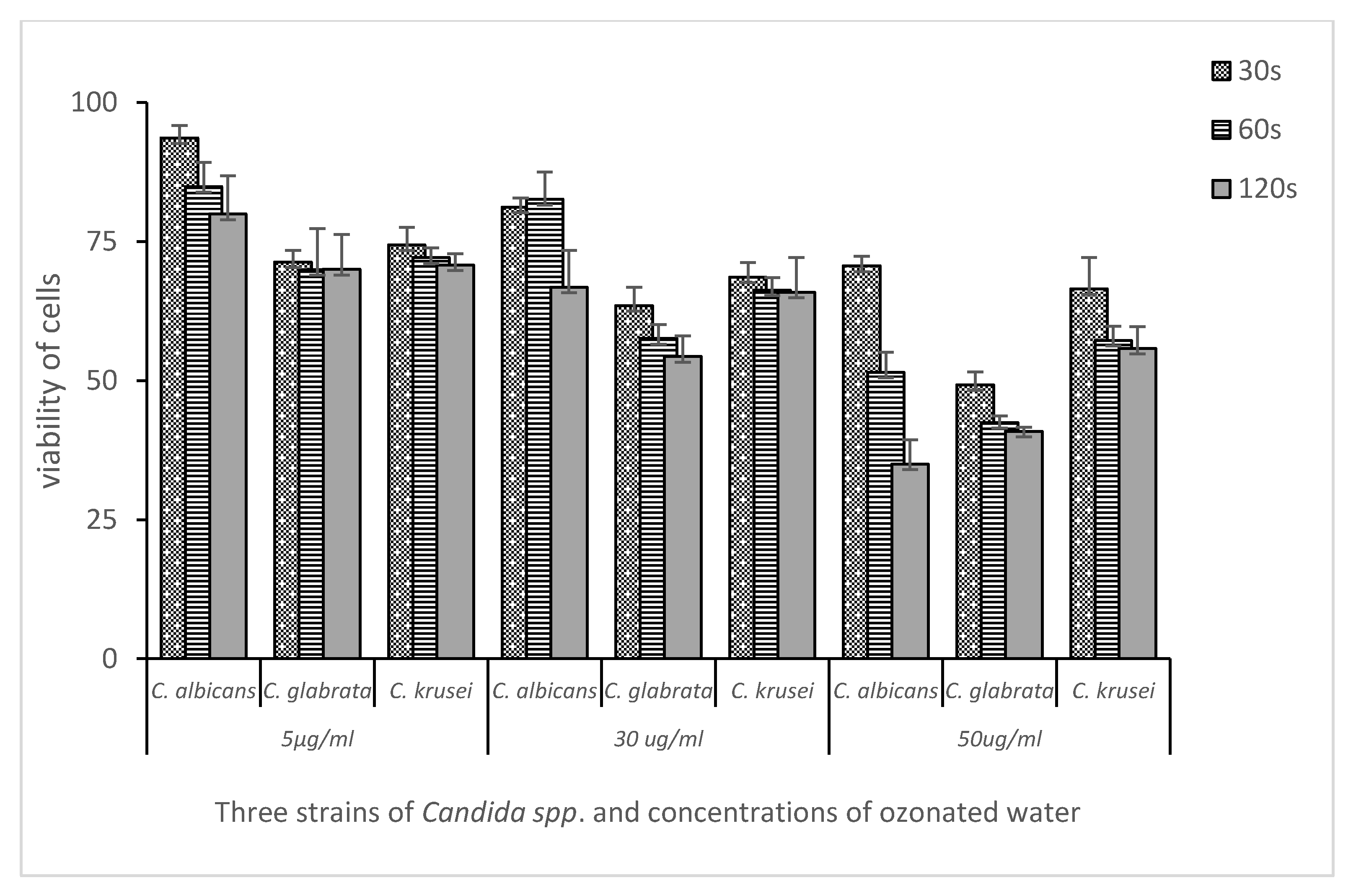
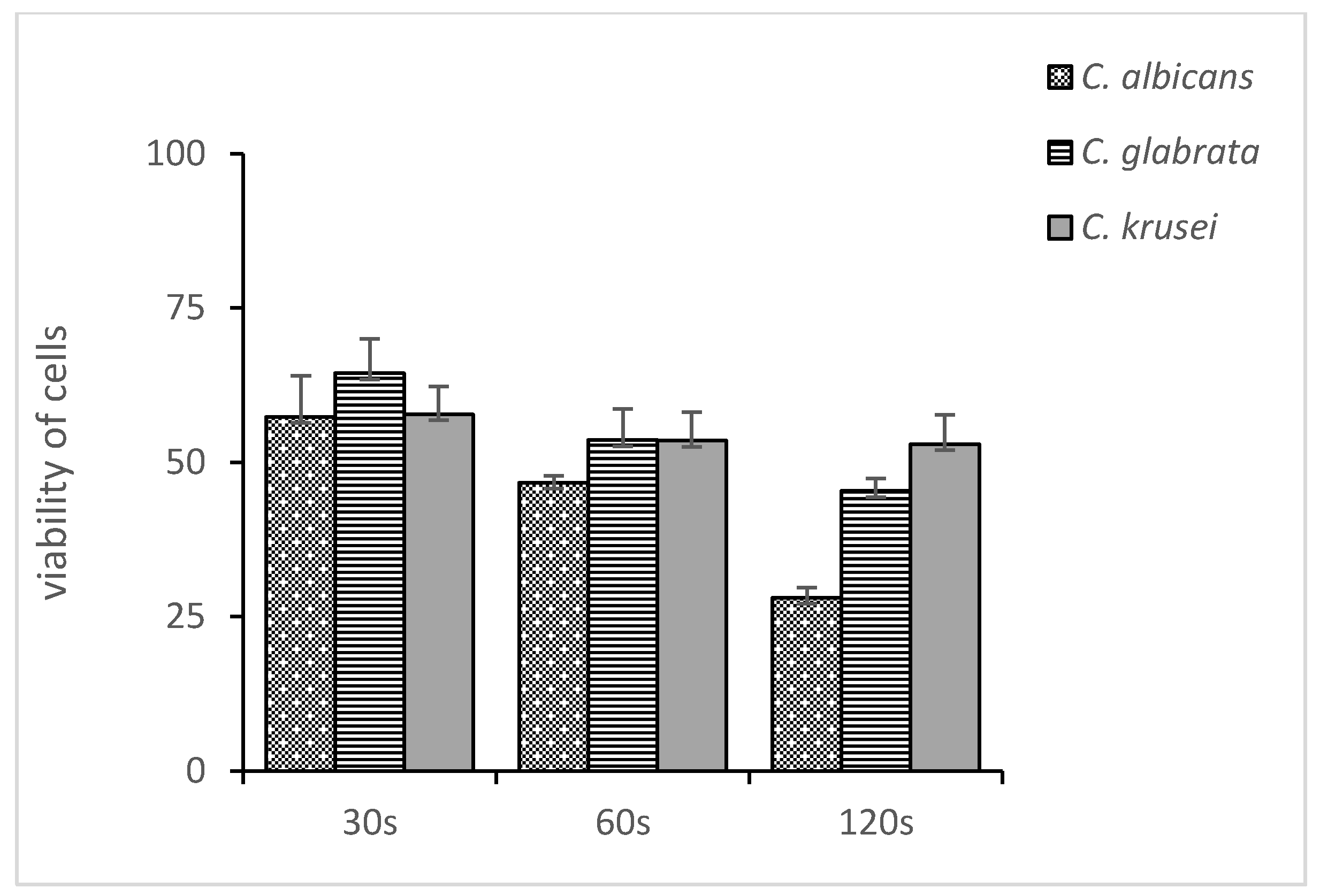
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giacobbe, D.R.; Maraolo, A.E.; Simeon, V.; Magnè, F.; Pace, M.C.; Gentile, I.; Chiodini, P.; Viscoli, C.; Sanguinetti, M.; Mikulska, M.; et al. Changes in the relative prevalence of candidaemia due to non-albicans Candida species in adult in-patients: A systematic review, meta-analysis and meta-regression. Mycoses 2020, 63, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Nobile, C.J.; Johnson, A.D. Candida albicans Biofilms and Human Disease. Annu. Rec. Microbiol. 2016, 69, 71–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vila, T.; Sultan, A.S.; Montelongo-jauregui, D. Oral Candidiasis: A Disease of Opportunity. J. Fungi 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, C.F.; Rodrigues, M.E.; Henriques, M.C.R. Promising Alternative Therapeutics for Oral Candidiasis. Curr. Med. Chem. 2018, 26, 2515–2528. [Google Scholar] [CrossRef]
- Welk, A.; Zahedani, M.; Beyer, C.; Kramer, A.; Müller, G. Antibacterial and antiplaque efficacy of a commercially available octenidine-containing mouthrinse. Clin. Oral Investig. 2016, 20, 1469–1476. [Google Scholar] [CrossRef]
- Soares, I.H.; Loreto, S.; Rossato, L.; Mario, D.N.; Venturini, T.P.; Baldissera, F.; Santurio, J.M.; Alves, S.H. In vitro activity of essential oils extracted from condiments against fluconazole-resistant and -sensitive Candida glabrata. J. Mycol. Med. 2015, 25, 213–217. [Google Scholar] [CrossRef]
- Srivatstava, A.; Ginjupalli, K.; Perampalli, N.U.; Bhat, N.; Ballal, M. Evaluation of the properties of a tissue conditioner containing origanum oil as an antifungal additive. J. Prosthet. Dent. 2013, 110, 313–319. [Google Scholar] [CrossRef]
- Ninomiya, K.; Hayama, K.; Ishijima, S.A.; Maruyama, N.; Irie, H.; Kurihara, J.; Abe, S. Suppression of inflammatory reactions by terpinen-4-ol, a main constituent of tea tree oil, in a murine model of oral candidiasis and its suppressive activity to cytokine production of macrophages In Vitro. Biol Pharm Bull. 2013, 36, 838–844. [Google Scholar] [CrossRef] [Green Version]
- Szweda, P.; Gucwa, K.; Kurzyk, E.; Romanowska, E.; Dzierżanowska-Fangrat, K.; Zielińska Jurek, A.; Kuś, P.M.; Milewski, S. Essential Oils, Silver Nanoparticles and Propolis as Alternative Agents Against Fluconazole Resistant Candida albicans, Candida glabrata and Candida krusei Clinical Isolates. Indian J. Microbiol. 2015, 55, 175–183. [Google Scholar] [CrossRef]
- Dalwai, S.; Rodrigues, S.J.; Baliga, S.; Shenoy, V.K.; Shetty, T.B.; Pai, U.Y.; Saldanha, S. Comparative evaluation of antifungal action of tea tree oil, chlorhexidine gluconate and fluconazole on heat polymerized acrylic denture base resin—An in vitro study. Gerodontology 2016, 33, 402–409. [Google Scholar] [CrossRef]
- Jebali, A.; Hajjar, F.H.E.; Pourdanesh, F.; Hekmatimoghaddam, S.; Kazemi, B.; Masoudi, A.; Daliri, K.; Sedighi, N. Silver and gold nanostructures: Antifungal property of different shapes of these nanostructures on Candida species. Med. Mycol. 2014, 52, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingle, A.P.; Duran, N.; Rai, M. Bioactivity, mechanism of action, and cytotoxicity of copper-based nanoparticles: A review. Appl. Microbiol. Biotechnol. 2014, 98, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.Y. In vitro antimicrobial effect of the tissue conditioner containing silver nanoparticles. J. Adv. Prosthodont. 2011, 3, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Wiench, R.; Nowicka, J.; Pajaczkowska, M.; Kuropka, P.; Skaba, D.; Kruczek-Kazibudzka, A.; Kuśka-Kiełbratowska, A.; Grzech-Leśniak, K. Influence of incubation time on ortho-toluidine blue mediated antimicrobial photodynamic therapy directed against selected Candida strains—An in vitro study. Int. J. Mol. Sci. 2021, 22, 10971. [Google Scholar] [CrossRef]
- Wiench, R.; Skaba, D.; Matys, J.; Grzech-Leśniak, K. Efficacy of Toluidine Blue—Mediated Antimicrobial Photodynamic on Candida spp. A systematic Review. Antibiotics 2021, 10, 349. [Google Scholar] [CrossRef] [PubMed]
- Wiench, R.; Skaba, D.; Stefanik, N.; Kępa, M.; Gilowski, Ł.; Cieślar, G.; Kawczyk-Krupka, A. Assessment of sensitivity of selected Candida strains on antimicrobial photodynamic therapy using diode laser 635 nm and toluidine blue—In vitro research. Photodiagnosis Photodyn. Ther. 2019, 27, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Kumar, T.; Arora, N.; Puri, G.; Aravinda, K.; Dixit, A.; Jatti, D. Efficacy of ozonized olive oil in the management of oral lesions and conditions: A clinical trial. Contemp. Clin. Dent. 2016, 7, 51. [Google Scholar] [CrossRef]
- Khatri, I.; Moge, G.; Kumar, N.A. Evaluation of effect of topical ozone therapy on salivary Candidal carriage in oral candidiasis. Indian J. Dent. Res. 2015, 26, 158–162. [Google Scholar]
- Sechi, L.; Lezcano, I.; Nunez, N.; Espim, M.; Pinna, A.; Molicotti, P.; Dupre, I.; Microbiologia, I. Antibacterial activity of ozonized sunfower oil (Oleozon). J. Appl. Microbiol. 2001, 90, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Lezcano, I.; Nuñez, N.; Espino, M.; Gómez, M. Antibacterial activity of ozonized sunflower oil, oleozon, against Staphylococcus aureus and Staphylococcus epidermidis. Ozone Sci. Eng. 2000, 22, 207–214. [Google Scholar] [CrossRef]
- Garg, R. Ozone: A new face of dentistry. Internet J. Dent. Sci. 2009, 7, 1–7. [Google Scholar] [CrossRef]
- Tiwari, S.; Avinash, A.; Katiyar, S.; Iyer, A.A. Dental applications of ozone therapy : A review of the literature. Saudi J. Dent. Res. 2016, 8, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.; Tyagi, P.; Bhagawati, S.; Kumar, A. Current interpretations and scientific rationale of the ozone usage in dentistry: A systematic review of literature. Eur. J. Gen. Dent. 2014, 3, 175. [Google Scholar] [CrossRef]
- Zeng, J.; Lu, J. Mechanisms of action involved in ozone-therapy in skin diseases. Int. Immunopharmacol. 2018, 56, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.; Patel, S.; Kaitlyn, R.; Gandhi, J.; Joshi, G.; Smith, N.L.; Khan, S.A. Clinical utility of ozone therapy in dental and oral medicine. Med. Gas Res. 2019, 9, 163–167. [Google Scholar] [CrossRef]
- Gupta, G.; Mansi, B. Ozone therapy in periodontics. J. Med. Life 2012, 5, 59–67. [Google Scholar]
- Naik, S.V.; Kohli, S.; Zohabhasan, S.; Bhatia, S. Ozone—A Biological Therapy in Dentistry-Reality or Myth. Open Dent. J. 2016, 10, 196–206. [Google Scholar] [CrossRef] [Green Version]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone gel in chronic periodontal disease: A randomized clinical trial on the anti-inflammatory effects of ozone application. Biology 2021, 10, 625. [Google Scholar] [CrossRef]
- Cardoso, M.G.; de Oliveira, L.D.; Koga-Ito, C.Y.; Jorge, A.O.C. Effectiveness of ozonated water on Candida albicans, Enterococcus faecalis, and endotoxins in root canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 85–91. [Google Scholar] [CrossRef]
- Falagas, M.E.; Roussos, N.; Vardakas, K.Z. Relative frequency of albicans and the various non-albicans Candida spp among candidemia isolates from inpatients in various parts of the world: A systematic review. Int. J. Infect. Dis. 2010, 14, e954–e966. [Google Scholar] [CrossRef] [Green Version]
- Kolliyavar, B.; Shettar, L.; Thakur, S. Chlorhexidine: The Gold Standard Mouth Wash. J. Pharm. Biomed. Sci. 2016; 6, 106–109. [Google Scholar] [CrossRef]
- Nogales, C.G.; Ferrari, P.H.; Olszewer, K.E. Ozone Therapy in Medicine and Dentistry. J. Contemp. Dent. Pract. 2008, 9, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Nagarajan, A.; Uchil, P. Analysis of Cell Viability by the MTT Assay. Cold Spring Harb. Protoc. 2018, 6, pdb-prot095489. [Google Scholar] [CrossRef] [PubMed]
- Monzillo, V.; Lallitto, F.; Russo, A.; Poggio, C.; Scribante, A.; Arciola, C.R.; Bertuccio, F.R.; Colombo, M. Ozonized gel against four Candida species: A pilot study and clinical perspectives. Materials 2020, 13, 1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Faria, I.D.S.; Ueno, M.; Yumi Koga-Ito, C.; Urrichi Irrazabal, W.; Balducci, I.; Jorge, A.O.C. Effects of ozonated water on Candida albicans oral isolates. Braz. J. Oral Sci. 2005, 4, 783–786. [Google Scholar]
- Lohse, M.B.; Gulati, M.; Johnson, A.D.; Nobile, C.J. Development and regulation of single- and multi-species Candida albicans biofilms. Nat. Publ. Gr. 2017, 16, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Colombo, M.; Ceci, M.; Felisa, E.; Poggio, C.; Pietrocola, G. Cytotoxicity evaluation of a new ozonized olive oil. Eur. J. Dent. 2018, 12, 585–589. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuśka-Kiełbratowska, A.; Wiench, R.; Mertas, A.; Bobela, E.; Kiełbratowski, M.; Lukomska-Szymanska, M.; Tanasiewicz, M.; Skaba, D. Evaluation of the Sensitivity of Selected Candida Strains to Ozonated Water—An In Vitro Study. Medicina 2022, 58, 1731. https://doi.org/10.3390/medicina58121731
Kuśka-Kiełbratowska A, Wiench R, Mertas A, Bobela E, Kiełbratowski M, Lukomska-Szymanska M, Tanasiewicz M, Skaba D. Evaluation of the Sensitivity of Selected Candida Strains to Ozonated Water—An In Vitro Study. Medicina. 2022; 58(12):1731. https://doi.org/10.3390/medicina58121731
Chicago/Turabian StyleKuśka-Kiełbratowska, Anna, Rafał Wiench, Anna Mertas, Elżbieta Bobela, Maksymilian Kiełbratowski, Monika Lukomska-Szymanska, Marta Tanasiewicz, and Dariusz Skaba. 2022. "Evaluation of the Sensitivity of Selected Candida Strains to Ozonated Water—An In Vitro Study" Medicina 58, no. 12: 1731. https://doi.org/10.3390/medicina58121731