
Hysteroscopic Removal of Intrauterine Device in Pregnancy: A Scoping Review to Guide Personalized Care
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
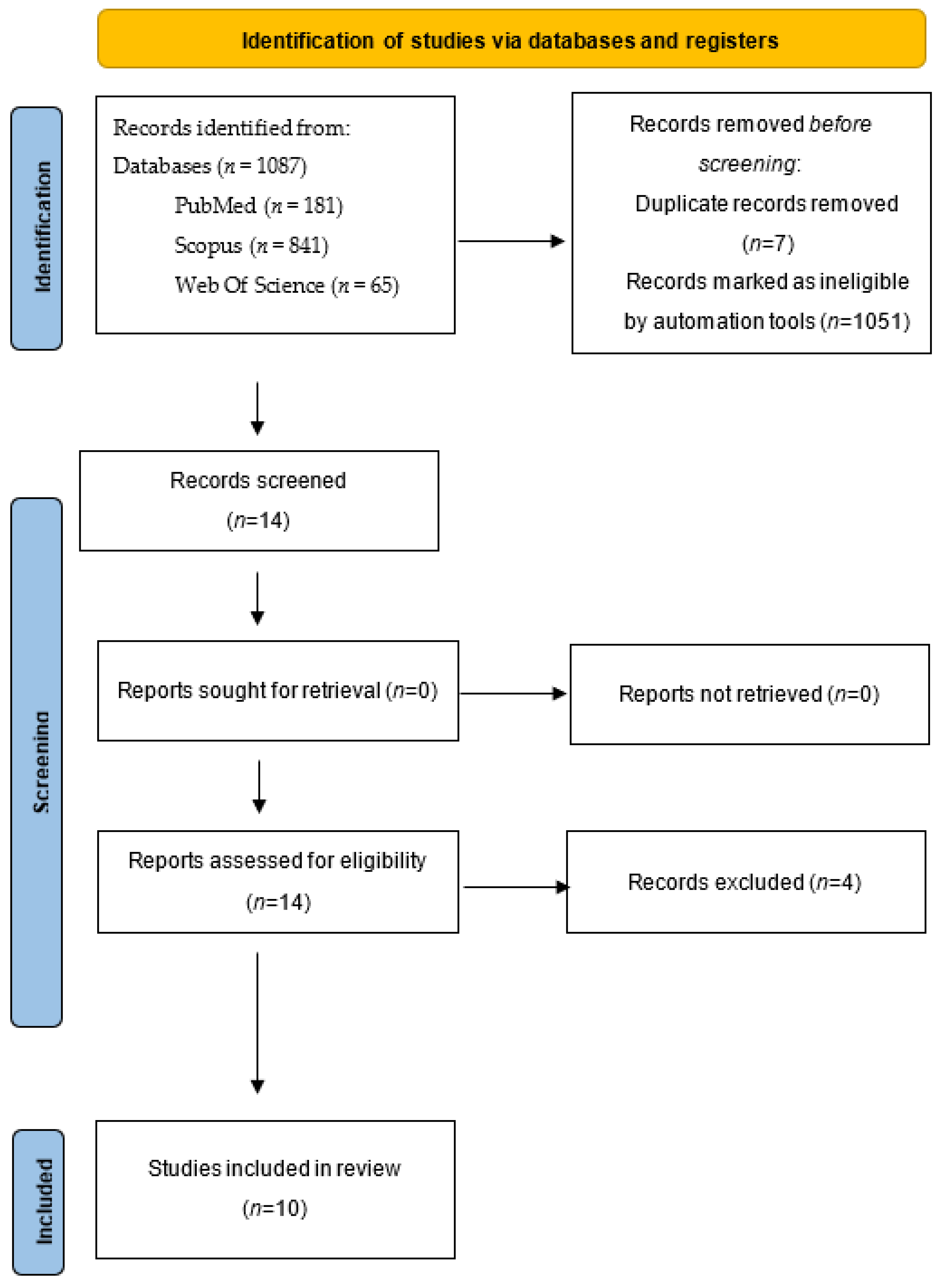
2. Materials and Methods
3. Results
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Author, Year | Study Type | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | D10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Stabile G. et al. (2022) [12] BMC Women’s Health | Case report | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | \ | \ |
| Ari P. Sanders et al. (2018) [13] Fertility and Sterility | Case series | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes |
| Shlomo B. Cohen et al. (2017) [5] JMIG The Journal of Minimally Invasive Gynecology | Case series | Yes | Yes | Yes | Yes | Yes | No | Unclear | Yes | No | Yes |
| Ari P. Sanders et al. (2016) [7] Science Direct | Case series | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes |
| Perez-Medina et al. (2013) [14] JMIG The Journal of Minimally Invasive Gynecology | Case series | Yes | Yes | Yes | No | No | No | Unclear | Yes | No | Yes |
| McCarthy et al. (2012) [6] Contraception | Case report | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | \ | \ |
| Rut Aguiar Couto et al. (2008) [15] Prog Obstet Ginecol. | Case series | Yes | Yes | Yes | Yes | Yes | Unclear | Yes | Yes | No | NA |
| Neis K.J. et al. (1994) [16] Gynecological Endoscopy | Case series | Yes | Yes | Yes | Unclear | Unclear | No | No | Yes | No | Unclear |
| Jen-Ching Lin et al. (1993) [17] Journal of Gynecologic Surgery | Case series | Yes | Yes | Yes | Yes | Yes | Unclear | No | Yes | No | Unclear |
| Assaf et al. (1992) [18] Contraception | Case series | Yes | Yes | Yes | Yes | Yes | No | No | Yes | No | NA |
- D1.
- Were there clear criteria for inclusion in the case series?
- D2.
- Was the condition measured in a standard, reliable way for all participants included in the case series?
- D3.
- Were valid methods used for identification of the condition for all participants included in the case series?
- D4.
- Did the case series have consecutive inclusion of participants?
- D5.
- Did the case series have complete inclusion of participants?
- D6.
- Was there clear reporting of the demographics of the participants in the study?
- D7.
- Was there clear reporting of clinical information of the participants?
- D8.
- Were the outcomes or follow-up results of cases clearly reported?
- D9.
- Was there clear reporting of the presenting site(s)/clinic(s) demographic information?
- D10.
- Was statistical analysis appropriate?
- D1.
- Were patient’s demographic characteristics clearly described?
- D2.
- Was the patient’s history clearly described and presented as a timeline?
- D3.
- Was the current clinical condition of the patient on presentation clearly described?
- D4.
- Were diagnostic tests or assessment methods and the results clearly described?
- D5.
- Was the intervention(s) or treatment procedure(s) clearly described?
- D6.
- Was the post-intervention clinical condition clearly described?
- D7.
- Were adverse events (harms) or unanticipated events identified and described?
- D8.
- Does the case report provide takeaway lessons?
References
- Buhling, K.J.; Zite, N.B.; Lotke, P.; Black, K. Worldwide use of intrauterine contraception: A review. Contraception 2014, 89, 162–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creinin, M.; Kohn, J.E.; Tang, J.H.; Serna, T.B. Society of Family Planning Committee statement on IUD nomenclature. Contraception 2022, 106, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Luukkainen, T.; Toivonen, J. Levonorgestrel-releasing IUD as a method of contraception with therapeutic properties. Contraception 1995, 52, 269–276. [Google Scholar] [CrossRef]
- Di Lorenzo, G.; Romano, F.; Mirenda, G.; Cracco, F.; Buonomo, F.; Stabile, G.; Facchin, S.; Ricci, G. “Nerve-sparing” laparoscopic treatment of parametrial ectopic pregnancy. Fertil. Steril. 2021, 116, 1197–1199. [Google Scholar] [CrossRef]
- Cohen, S.B.; Bouaziz, J.; Bar-On, A.; Schiff, E.; Goldenberg, M.; Mashiach, R. In-office Hysteroscopic Extraction of Intrauterine Devices in Pregnant Patients Who Underwent Prior Ultrasound-guided Extraction Failure. J. Minim. Invasive Gynecol. 2017, 24, 833–836. [Google Scholar] [CrossRef]
- McCarthy, E.A.; Jagasia, N.; Maher, P.; Robinson, M. Ultrasound-guided hysteroscopy to remove a levonorgestrel intrauterine system in early pregnancy. Contraception 2012, 86, 587–590. [Google Scholar] [CrossRef]
- Sanders, A.P.; Fluker, M.R.; Sanders, B.H. Saline Hysteroscopy for Removal of Retained Intrauterine Contraceptive Devices in Early Pregnancy. J. Obstet. Gynaecol. Can. 2016, 38, 1114–1119. [Google Scholar] [CrossRef]
- Vitale, S.G. The Biopsy Snake Grasper Sec. VITALE: A New Tool for Office Hysteroscopy. J. Minim. Invasive Gynecol. 2020, 27, 1414–1416. [Google Scholar] [CrossRef]
- Sorrentino, F.; De Feo, V.; Stabile, G.; Tinelli, R.; D’Alterio, M.; Ricci, G.; Angioni, S.; Nappi, L. Cesarean Scar Pregnancy Treated by Artery Embolization Combined with Diode Laser: A Novel Approach for a Rare Disease. Medicina 2021, 57, 411. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Database Syst. Rev. Implement. Rep. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Stabile, G.; Godina, C.; Cracco, F.; Mangino, F.P.; Canton, M.; Romano, F.; Ricci, G. Hysteroscopic removal of intrauterine device in early pregnancy. BMC Womens Health 2022, 22, 425. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.P.; Sanders, B. Hysteroscopic removal of intrauterine devices in pregnancy. Fertil. Steril. 2018, 110, 1408–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Medina, T.; Sauco, J.S.; Ríos, M.; Pereira, A.; Argila, N.; Cabezas, E.; Cayuela, E. Hysteroscopy in Pregnancy-Related Conditions: Descriptive Analysis in 273 Patients. J. Minim. Invasive Gynecol. 2014, 21, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Couto, M.R.A.; Hernández, R.V.; Rodríguez, M.G.; Portela, A.L.; Valenzuela, A.O. Extracción de DIU mediante histeroscopia en la gestación precoz: Nuestra experiencia en 4 casos. Prog. Obs. Y Ginecol. 2008, 51, 162–166. [Google Scholar] [CrossRef]
- Neis, K.J.; Brandner, P.; Otte, C. Hysteroscopic removal of lost intra-uterine devices in pregnancy. Gynaecol. Endosc. 1994, 3, 233–237. [Google Scholar]
- Lin, J.C.; Chen, Y.O.; Lin, B.L.; Valle, R.F. Outcome of Removal of Intrauterine Devices with Flexible Hysteroscopy in Early Pregnancy. J. Gynecol. Surg. 1993, 9, 195–200. [Google Scholar] [CrossRef]
- Assaf, A.; Gohar, M.; Saad, S.; El-Nashar, A.; Aziz, A.A. Removal of intrauterine devices with missing tails during early pregnancy. Contraception 1992, 45, 541–546. [Google Scholar] [CrossRef]
- Vitale, S.G.; Laganà, A.S.; Caruso, S.; Garzon, S.; Vecchio, G.M.; La Rosa, V.L.; Casarin, J.; Ghezzi, F. Comparison of three biopsy forceps for hysteroscopic endometrial biopsy in postmenopausal patients (HYGREB-1): A multicenter, single-blind randomized clinical trial. Int. J. Gynecol. Obstet. 2021, 155, 425–432. [Google Scholar] [CrossRef]
- Mermet, J.; Bolcato, C.; Rudigoz, R.C.; Dargent, D. Outcome of pregnancies with an intrauterine devices and their management. Rev. Fr. Gynecol. Obstet. 1986, 81, 233–235. [Google Scholar]
- Tatum, H.J.; Schmidt, F.H.; Jain, A.K. Management and outcome of pregnancies associated with the Copper T intrauterine contraceptive device. Am. J. Obstet. Gynecol. 1976, 126, 869–879. [Google Scholar] [CrossRef]
- Alvior, G.T. Pregnancy outcome with removal of intrauterine device. Obstet. Gynecol. 1973, 41, 894–896. [Google Scholar] [PubMed]
- Brahmi, D.; Steenland, M.W.; Renner, R.-M.; Gaffield, M.E.; Curtis, K.M. Pregnancy outcomes with an IUD in situ: A systematic review. Contraception 2012, 85, 131–139. [Google Scholar] [CrossRef]
- Sorrentino, F.; Petito, A.; Angioni, S.; D’Antonio, F.; Severo, M.; Solazzo, M.C.; Tinelli, R.; Nappi, L. Impact of anxiety levels on the perception of pain in patients undergoing office hysteroscopy. Arch. Gynecol. Obstet. 2021, 303, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Schiesser, M.; Lapaire, O.; Tercanli, S.; Holzgreve, W. Lost intrauterine devices during pregnancy: Maternal and fetal outcome after ultrasound-guided extraction. An analysis of 82 cases. Ultrasound Obstet. Gynecol. 2004, 23, 486–489. [Google Scholar] [CrossRef]

| Author (Year) Journal Article Type | Number of Patients (n) | Mean Patients Age (Years) | Mean Gestational Age at the Time of the Procedure (Weeks) | Evolutive Pregnancy | Pregnancy Losses (n) | Preterm Deliveries | Deliveries at Term | Hysteroscope Caliber (mm) |
|---|---|---|---|---|---|---|---|---|
| Stabile G et al. (2022) [12] BMC Women’s Health Case report | 1 | 37 | 6 | 1 | 0 (induced abortion 4 weeks after the procedure) | 0 | 0 | 5 |
| Ari P. Sanders et al. (2018) [13] Fertility and Sterility Case series | 4 | 34 | 10.25 | 4 | 0 | 0 | 4 | 3–5 |
| Shlomo B. Cohen et al. (2017) [5] JMIG The Journal of Minimally Invasive Gynecology Case series | 8 | 30.5 | 7.3 | 7 | 1 (2 weeks after the procedure) | 0 | 7 | 5 |
| Ari P. Sanders et al. (2016) [7] Science Direct Case series | 25 | 30.7 | 11 | 23 | 1 (12 days after the procedure) | 3 | 20 | 5 |
| Perez-Medina et al. (2013) [14] JMIG The Journal of Minimally Invasive Gynecology Case series | 7 | Not known | 8.2 | 6 | 1 (2 weeks after retrieval of the device) | 0 | 7 | Non available. Operating channel was 1.7 mm in diameter (5F) |
| McCarthy et al. (2012) [6] Contraception Case report | 1 | 30 | 8 | 1 | 0 | 0 | 1 | Not available |
| Rut Aguiar Couto et al. (2008) [15] Prog Obstet Ginecol. Case series | 4 | 31 | 7 | 3 | 1 (7 weeks after the procedure) | 0 | 3 | 3,9–5,9 |
| Neis K.J. et al. (1994) [16] Gynaecological Endoscopy Case series | 26 | Not known | 8 | 24 | 2 (first postoperative day and 6 weeks after the removal) | 0 | 24 | Not available |
| Jen-Ching Lin et al. (1993) [17] Journal of Gynecologic Surgery Case series | 28 | Not known | 7 | 24 | 4 | 0 | 24 | 3.7–4.8 |
| Assaf et al. (1992) [18] Contraception Case series | 50 | Not known | 42 under 12 weeks of gestation, 8 patients more than 12 weeks of gestation | 46 | 4 (2 immediate abortions, 2 abortions after a few days) | 15 | 31 | 7 |
| Hysteroscopic Procedural Tricks | Rationale | |
|---|---|---|
| 1 | Use isotonic distension fluids | Minimize gestational sac trauma |
| 2 | Avoid cervical dilation | Avoid potential gestational sac trauma |
| 3 | Prefer small-caliber hysteroscopes (e.g., 3 to 5 mm instruments) | Helps to avoid cervical dilation |
| 4 | Use of low-pressure distension media infusion, during entrance (50 mmHg) and when grasping (40 mmHg) | Minimize gestational sac trauma and reduce IUD fragment mobility |
| 5 | Consider heating the distension media up to 30 °C | Reduce vasoconstriction |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stabile, G.; Cracco, F.; Nappi, L.; Sorrentino, F.; Vitale, S.G.; Angioni, S.; Carlucci, S.; Ricci, G. Hysteroscopic Removal of Intrauterine Device in Pregnancy: A Scoping Review to Guide Personalized Care. Medicina 2022, 58, 1688. https://doi.org/10.3390/medicina58111688
Stabile G, Cracco F, Nappi L, Sorrentino F, Vitale SG, Angioni S, Carlucci S, Ricci G. Hysteroscopic Removal of Intrauterine Device in Pregnancy: A Scoping Review to Guide Personalized Care. Medicina. 2022; 58(11):1688. https://doi.org/10.3390/medicina58111688
Chicago/Turabian StyleStabile, Guglielmo, Francesco Cracco, Luigi Nappi, Felice Sorrentino, Salvatore Giovanni Vitale, Stefano Angioni, Stefania Carlucci, and Giuseppe Ricci. 2022. "Hysteroscopic Removal of Intrauterine Device in Pregnancy: A Scoping Review to Guide Personalized Care" Medicina 58, no. 11: 1688. https://doi.org/10.3390/medicina58111688