
Breast Cancer Incidence Patterns in the Saudi Female Population: A 17-Year Retrospective Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Administrative Regions of Saudi Arabia
2.3. Statistical Parameters
3. Results
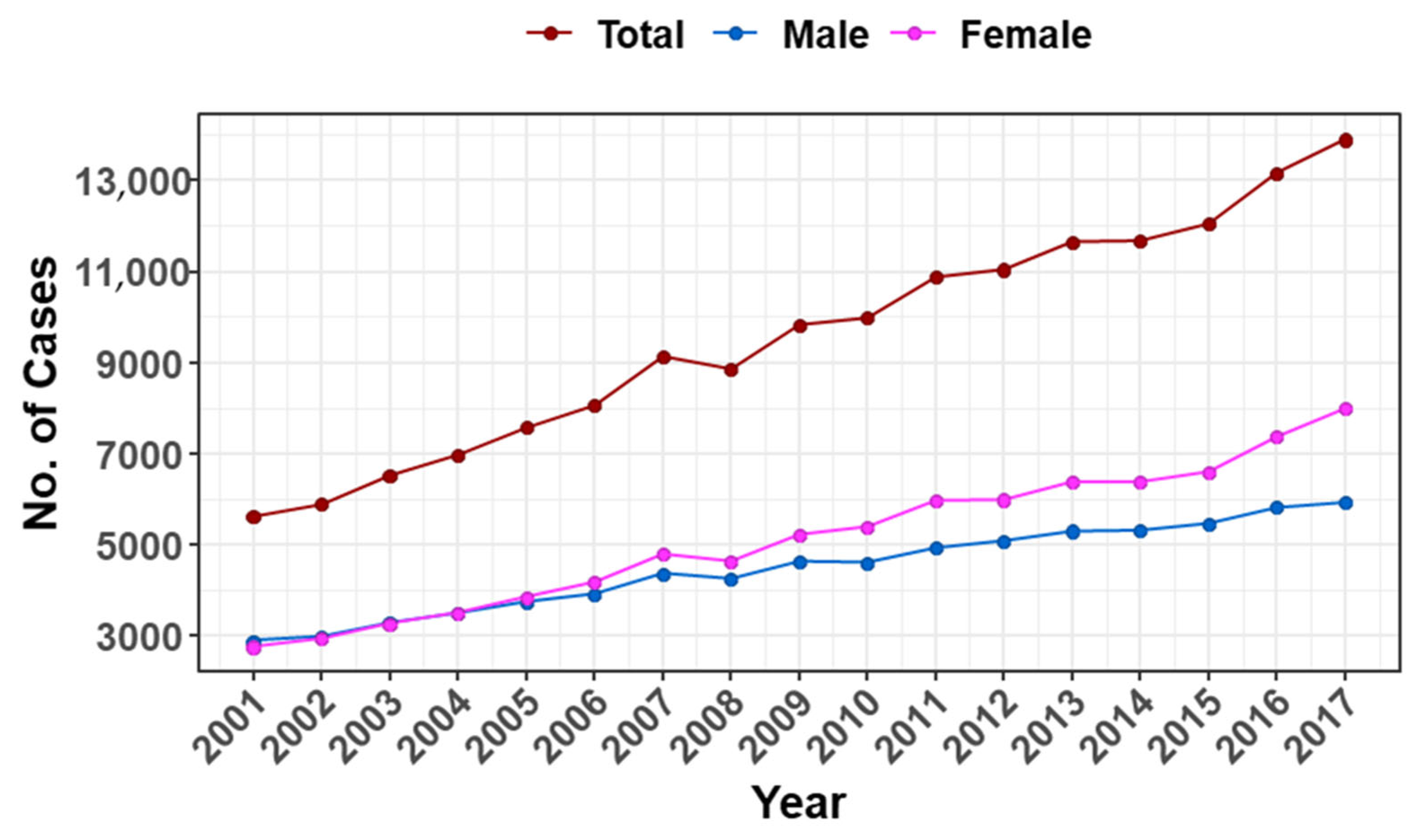
3.1. Number of All Cancer Cases in the Saudi Population
3.2. Breast Cancer Cases and Age at Diagnosis in the Saudi Female Population
3.3. Incidence Rates for Breast Cancer among the Saudi Female Population
3.4. Distribution of Breast Cancer Histological Subtypes
3.5. Trends in Breast Cancer Incidence
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Houghton, S.C.; Hankinson, S.E. Cancer progress and priorities: Breast cancer, cancer epidemiol. Biomark. Prev. 2021, 30, 822–844. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN Estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA: A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Rabbani, S.A.; Mazar, A.P. Evaluating distant metastases in breast cancer: From biology to outcomes. Cancer Metastasis Rev. 2007, 26, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Valastyan, S.; Weinberg, R.A. Tumor metastasis: Molecular insights and evolving paradigms. Cell 2011, 147, 275–292. [Google Scholar] [CrossRef] [Green Version]
- Steeg, P.S. Targeting metastasis. Nat. Rev. Cancer 2016, 16, 201–218. [Google Scholar] [CrossRef]
- Mariotto, A.B.; Etzioni, R.; Hurlbert, M.; Penberthy, L.; Mayer, M. Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol. Prev. Biomark. 2017, 26, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, W.S.; Almufareh, N.A.; Domiaty, D.M.; Albasher, G.; Alduwish, M.A.; Alkhalaf, H.; Almuzzaini, B.; Al-Marshidy, S.S.; Alfraihi, R.; Elasbali, A.M.; et al. Epidemiology of cancer in Saudi Arabia thru 2010–2019: A systematic review with constrained meta-analysis Running title: Epidemiology of cancer in Saudi Arabia thru 2010–2019. AIMS Public Health 2020, 7, 679–696. [Google Scholar] [CrossRef]
- Al-Othman, S.; Haoudi, A.; Alhomoud, S.; Alkhenizan, A.; Khoja, T.; Al-Zahrani, A. Tackling cancer control in the Gulf Cooperation Council Countries. Lancet Oncol. 2015, 16, e246–e257. [Google Scholar] [CrossRef]
- Demographic and Health Indicators for Countries of the Eastern Mediterranean. 1999. Available online: https://apps.who.int/iris/handle/10665/116297 (accessed on 8 September 2022).
- Kim, H.-J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. Stat. Med. 2000, 19, 351. [Google Scholar] [CrossRef]
- Lei, S.; Zheng, R.; Zhang, S.; Wang, S.; Chen, R.; Sun, K.; Zeng, H.; Zhou, J.; Wei, W. Global patterns of breast cancer incidence and mortality: A population-based cancer registry data analysis from 2000 to 2020. Cancer Commun. 2021, 41, 1183–1194. [Google Scholar] [CrossRef]
- Baade, P.D.; Youlden, D.R.; Cramb, S.M.; Dunn, J.; Gardiner, R.A. Epidemiology of prostate cancer in the Asia-Pacific region. Prostate Int. 2013, 1, 47–58. [Google Scholar] [CrossRef] [Green Version]
- Politis, M.; Higuera, G.; Chang, L.R.; Gomez, B.; Bares, J.; Motta, J. Trend analysis of cancer mortality and incidence in Panama, using Joinpoint Regression Analysis. Medicine 2015, 94, e970. [Google Scholar] [CrossRef]
- Albeshan, S.M.; Alashban, Y.I. Incidence trends of breast cancer in Saudi Arabia: A Joinpoint Regression Analysis (2004–2016). J. King Saud Univ. Sci. 2021, 33, 101578. [Google Scholar] [CrossRef]
- Fares, M.Y.; Salhab, H.A.; Khachfe, H.H.; Khachfe, H.M. Breast cancer epidemiology among Lebanese women: An 11-year analysis. Medicina 2019, 55, 463. [Google Scholar] [CrossRef] [Green Version]
- WHO. International Agency for Research on Cancer. The Global Cancer Observatory (GCO). 2022. Available online: https://gco.iarc.fr/overtime/en (accessed on 14 September 2022).
- Bawazir, A.; Al-Zamel, N.; Amen, A.; Akiel, M.; Alhawiti, N.M.; AlShehri, A. The burden of leukemia in the Kingdom of Saudi Arabia: 15 years period (1999–2013). BMC Cancer 2019, 19, 703. [Google Scholar] [CrossRef] [Green Version]
- Albeshan, S.M.; Mackey, M.G.; Hossain, S.Z.; Alfuraih, A.A.; Brennan, P.C. Breast cancer epidemiology in Gulf Cooperation Council countries: A regional and international comparison. Clin. Breast Cancer 2018, 18, e381–e392. [Google Scholar] [CrossRef]
- Chahine, G.; El Rassy, E.; Khazzaka, A.; Saleh, K.; Rassy, N.; Khalife, N.; Atallah, D. Characteristics of incident female breast cancer in Lebanon, 1990–2013: Descriptive study of 612 cases from a hospital tumor registry. Cancer Epidemiol. 2015, 39, 303–306. [Google Scholar] [CrossRef]
- Ramon, J.M.; Escriba, J.M.; Casas, I.; Benet, J.; Gavalda, L.; Torras, G.; Oromi, J. Age at first full-term pregnancy, lactation a n d parity and risk of breast cancer: A case-control study in Spain. Eur. J. Epidemiol. 1996, 12, 449–453. [Google Scholar] [CrossRef]
- Bernstein, L. Epidemiology of endocrine-related risk factors for breast cancer. J. Mammary Gland Biol. Neoplasia 2002, 7, 3–15. [Google Scholar] [CrossRef]
- Babay, Z.A.; Addar, M.H.; Shahid, K.; Meriki, N. Age at menarche and the reproductive performance of Saudi women. Ann. Saudi Med. 2004, 24, 354–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shawky, S.; Abalkhail, B.A. Maternal factors associated with the duration of breast feeding in Jeddah, Saudi Arabia. Paediatr. Perinat. Epidemiology 2003, 17, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, J.L.; Gammon, M.D.; John, E.M. Reproductive factors and breast cancer. Epidemiologic Rev. 1993, 15, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Lambe, M.; Hsieh, C.-C.; Chan, H.-W.; Ekbom, A.; Trichopoulos, D.; Adami, H.-O. Parity, age at first and last birth, and risk of breast cancer: A population-based study in Sweden. Breast Cancer Res. Treat. 1996, 38, 305–311. [Google Scholar] [CrossRef]
- Ng, S.W.; Zaghloul, S.; Ali, H.I.; Harrison, G.; Popkin, B.M. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf States. Obes. Rev. 2010, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mabry, R.M.; Reeves, M.M.; Eakin, E.; Owen, N. Evidence of physical activity participation among men and women in the countries of the Gulf Cooperation Council: A review. Obes. Rev. 2009, 11, 457–464. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Takruri, H.R.; Hassan, A.S.; Abu-Tarboush, H. Food-based dietary guidelines for the Arab Gulf countries. J. Nutr. Metab. 2012, 2012, 303. [Google Scholar] [CrossRef] [Green Version]
- La Vecchia, C.; Giordano, S.H.; Hortobagyi, G.N.; Chabner, B. Overweight, obesity, diabetes, and risk of breast cancer: Interlocking pieces of the puzzle. Oncol. 2011, 16, 726–729. [Google Scholar] [CrossRef] [Green Version]
- Glade, M.J. Food, nutrition, physical activity and the prevention of cancer: A global perspective. World Cancer Research Fund/American Institute for Cancer Research, American Institute for Cancer Research, Washington, D.C (2007). Nutrition 2008, 24, 393–398. [Google Scholar] [CrossRef]
- Cleary, M.P.; Grossmann, M.E. Obesity and breast cancer: The estrogen connection. Endocrinology 2009, 150, 2537–2542. [Google Scholar] [CrossRef]
- Hassounah, S.; Rawaf, D.; Khoja, T.; Rawaf, S.; Hussein, M.; Qidwai, W.; Majeed, A. Tobacco control efforts in the Gulf Cooperation Council countries: Achievements and challenges. East. Mediterr. Health J. 2014, 20, 508–513. [Google Scholar] [CrossRef]
- Bjerkaas, E.; Parajuli, R.; Weiderpass, E.; Engeland, A.; Maskarinec, G.; Selmer, R.; Gram, I.T. Smoking duration before first childbirth: An emerging risk factor for breast cancer? Results from 302,865 Norwegian women. Cancer Causes Control 2013, 24, 1347–1356. [Google Scholar] [CrossRef] [Green Version]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Active cigarette smoking and risk of breast cancer. Int. J. Cancer 2014, 136, 2204–2209. [Google Scholar] [CrossRef]
- Macacu, A.; Autier, P.; Boniol, M.; Boyle, P. Active and passive smoking and risk of breast cancer: A meta-analysis. Breast Cancer Res. Treat. 2015, 154, 213–224. [Google Scholar] [CrossRef] [Green Version]
- White, M.C.; Holman, D.M.; Boehm, J.E.; Peipins, L.A.; Grossman, M.; Henley, S.J. Age and cancer risk: A potentially modifiable relationship. Am. J. Prev. Med. 2014, 46, S7–S15. [Google Scholar] [CrossRef] [Green Version]
- Hajjar, R.; Atli, T.; Al-Mandhari, Z.; Oudrhiri, M.; Balducci, L.; Silbermann, M. Prevalence of aging population in the Middle East and its implications on cancer incidence and care. Ann. Oncol. 2013, 24 (Suppl. 7), vii11–vii24. [Google Scholar] [CrossRef]
- Smith, R.A.; Ba, K.S.A.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Wender, R.C. Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA A Cancer J. Clin. 2019, 69, 184–210. [Google Scholar] [CrossRef]
- VFabiano, V.; Mandó, P.; Rizzo, M.; Ponce, C.; Coló, F.; Loza, M.; Loza, J.; Amat, M.; Mysler, D.; Costanzo, M.V.; et al. Breast Cancer in Young Women Presents With More Aggressive Pathologic Characteristics: Retrospective Analysis From an Argentine National Database. JCO Glob. Oncol. 2020, 6, 639–646. [Google Scholar] [CrossRef]
- Bharat, A.; Aft, R.L.; Gao, F.; Margenthaler, J.A. Patient and tumor characteristics associated with increased mortality in young women (≤40 years) with breast cancer. J. Surg. Oncol. 2009, 100, 248–251. [Google Scholar] [CrossRef]
- Nixon, A.J.; Neuberg, D.; Hayes, D.F.; Gelman, R.; Connolly, J.L.; Schnitt, S.; Abner, A.; Recht, A.; Vicini, F.; Harris, J.R. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J. Clin. Oncol. 1994, 12, 888–894. [Google Scholar] [CrossRef]
- Collins, L.C.; Marotti, J.D.; Gelber, S.; Cole, K.; Ruddy, K.; Kereakoglow, S.; Brachtel, E.F.; Schapira, L.; Come, S.E.; Winer, E.P.; et al. Pathologic features and molecular phenotype by patient age in a large cohort of young women with breast cancer. Breast Cancer Res. Treat. 2011, 131, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wu, J.; Zhang, Z.; Tang, Y.; Li, X.; Liu, S.; Cao, S.; Li, X. Association between BRCA status and triple-negative breast cancer: A meta-analysis. Front. Pharmacol. 2018, 9, 909. [Google Scholar] [CrossRef] [PubMed]
- ZBaretta, Z.; Mocellin, S.; Goldin, E.; Olopade, O.I.; Huo, D. Effect of BRCA germline mutations on breast cancer prognosis. Medicine 2016, 95, e4975. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nationality | Gender | Subtypes | Age |
|---|---|---|---|
| Saudi only | Female only | Invasive Ductal Carcinoma (IDC), Invasive Lobular Carcinoma (ILC), Mixed, or Other | All age groups, as follows: 0–4, 5–9, 10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, and >75 |
| Parameter | 2001 | 2017 | % Increase (2001–2017) |
|---|---|---|---|
| Total number of all cancer cases | 2741.0 | 7975.0 | 191.0 |
| Total number of breast cancer cases | 545.0 | 2463.0 | 351.9 |
| % of breast cancer cases among all cancer cases | 19.9 | 30.9 | 55.3 |
| Breast cancer median age at diagnosis | 48.0 | 51.0 | 6.3 |
| CIR | 6.8 | 24.6 | 261.8 |
| ASR | 11.8 | 29.7 | 151.7 |
| Age Group | APC | 95% CI |
|---|---|---|
| 45–49 | 4.1 * | [2.6–5.7] |
| 50–54 | 6.8 * | [5.7–8] |
| 55–59 | 6.9 * | [5.1–8.7] |
| 60–64 | 5.2 * | [3.6–6.9] |
| 65–69 | 6.0 * | [3.4–8.6] |
| 70–74 | 10.2 * | [7.2–13.4] |
| 75+ | 7.2 * | [6–8.5] |
| Region | APC | 95% CI |
|---|---|---|
| Asir | 6.0 * | [4.6–7.5] |
| Baha | 6.9 * | [1.1–13.1] |
| East | 4.8 * | [3.7–6] |
| Hail | 8.7 * | [6.2–11.3] |
| Jazan | 3.8 | [−0.1–7.8] |
| Jouf | 8.8 * | [3.7–14.2] |
| Madinah | 4.8 * | [2.5–7.3] |
| Makkah | 4.0 * | [2.4–5.6] |
| Najran | 4.7 | [−0.5–10.2] |
| North | 8.6 * | [3–14.6] |
| Qassim | 6.2 * | [3.6–8.9] |
| Riyadh | 4.8 * | [3.8–5.9] |
| Tabuk | 2 | [−0.4–4.4] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basudan, A.M. Breast Cancer Incidence Patterns in the Saudi Female Population: A 17-Year Retrospective Analysis. Medicina 2022, 58, 1617. https://doi.org/10.3390/medicina58111617
Basudan AM. Breast Cancer Incidence Patterns in the Saudi Female Population: A 17-Year Retrospective Analysis. Medicina. 2022; 58(11):1617. https://doi.org/10.3390/medicina58111617
Chicago/Turabian StyleBasudan, Ahmed M. 2022. "Breast Cancer Incidence Patterns in the Saudi Female Population: A 17-Year Retrospective Analysis" Medicina 58, no. 11: 1617. https://doi.org/10.3390/medicina58111617