
Effect of the Helping Babies Breathe Program on Newborn Outcomes: Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion Criteria
- The term newborn was considered as a gestational age of greater than or equal to 37 weeks of gestation and up to 30 days of life. The term preterm newborn was considered as a gestational age of fewer than 37 weeks and up to 30 days of life and/or 40 weeks of corrected age at term.
- Studies, whose objective was to evaluate the effect of the implementation of the HBB program in private or public health institutions (hospitals or clinics), in low and middle-income countries or scenarios.
- Reporting data on mortality and morbidity outcomes.
- Clinical trials, quasi-experimental studies, and observational studies.
2.3. Exclusion Criteria
- Literature reviews such as systematic, integrative, and/or narrative reviews; a summary of conferences and correspondence to the editor.
- Poster presentations, conferences, and/or abstracts only.
2.4. Outcomes
2.5. Screening and Inclusion of Studies
2.6. Data Extraction and Synthesis
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Assessment of Quality and Risk of Bias of the Studies
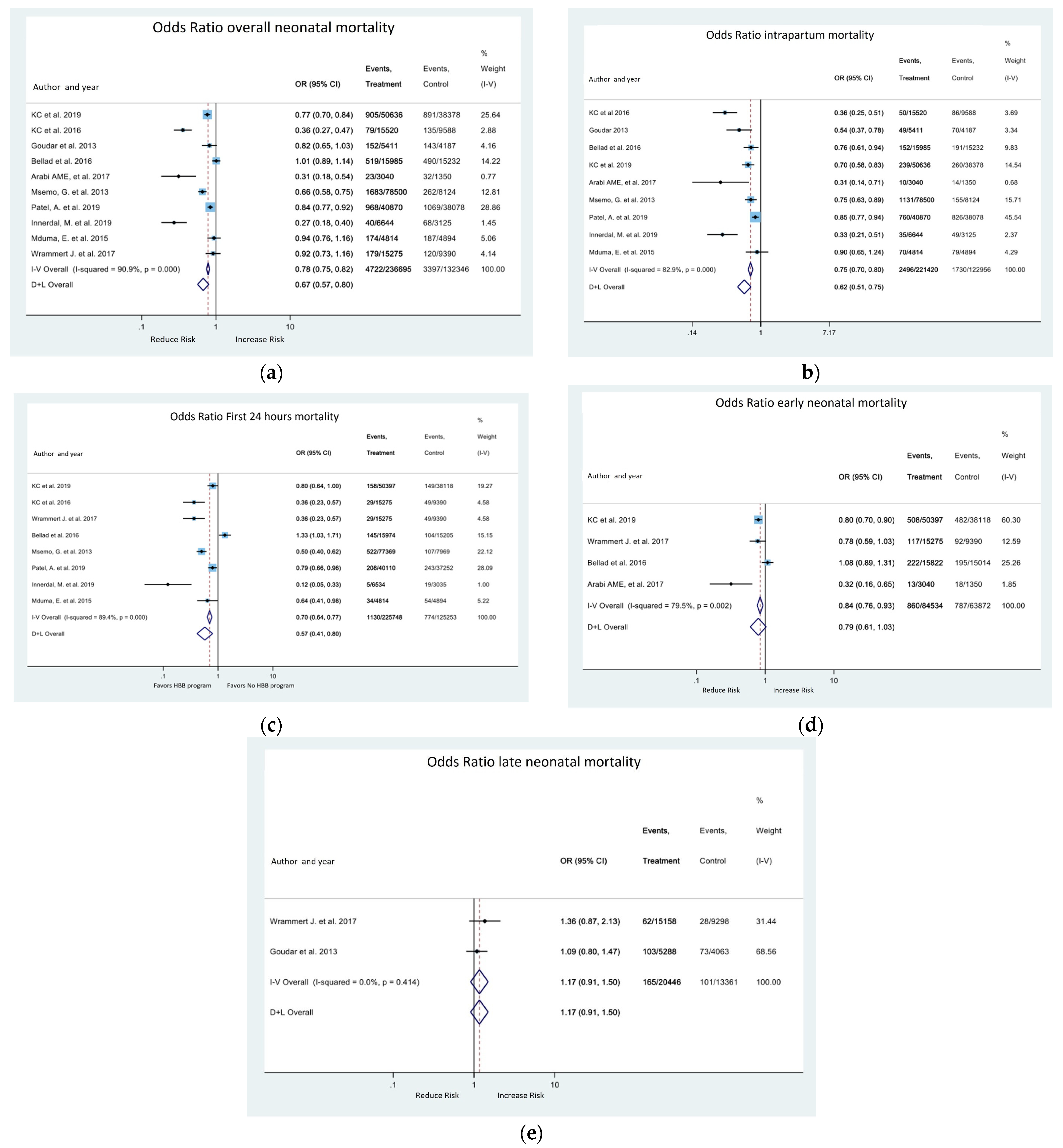
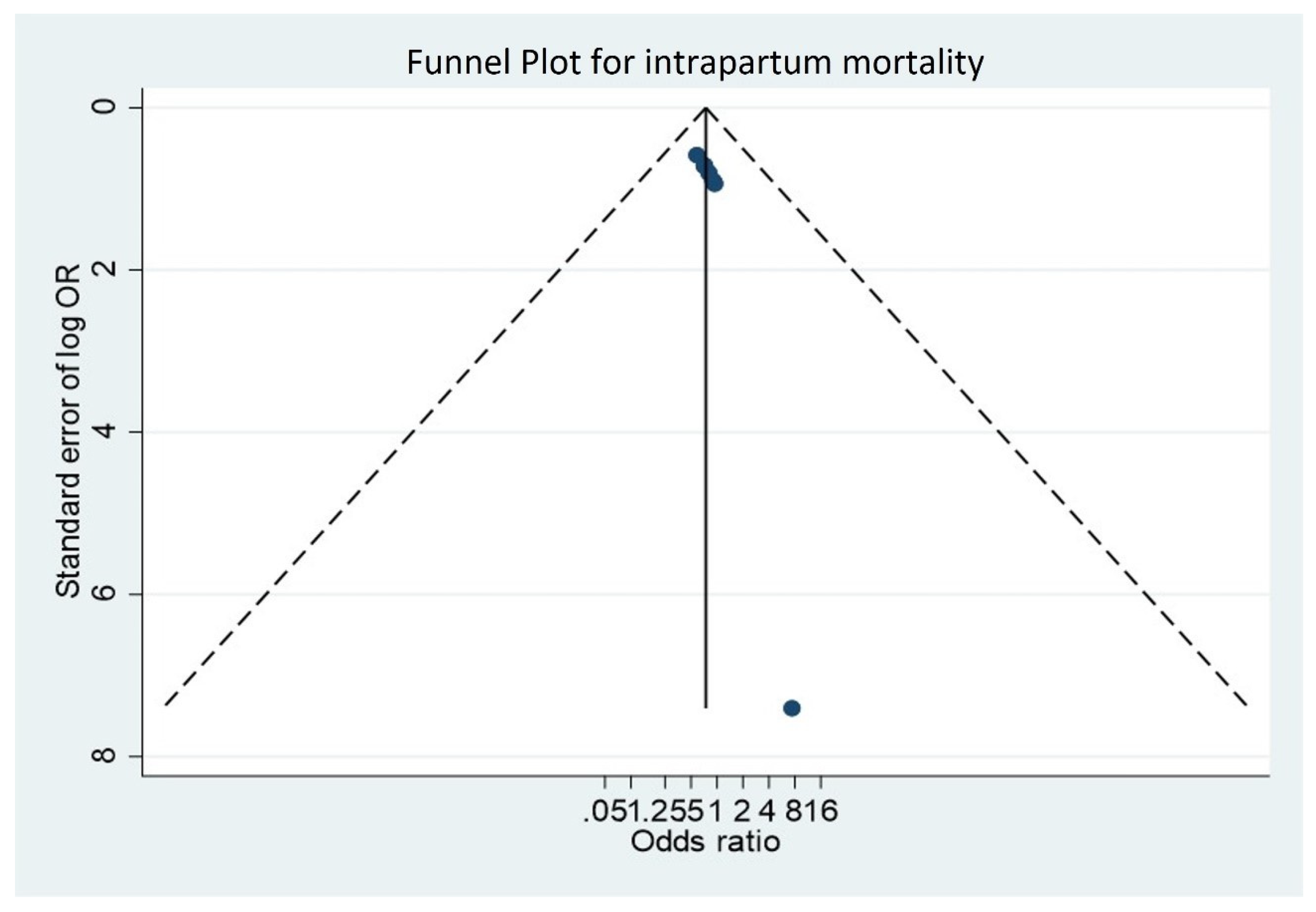
3.3. Meta-Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Objetivos y Metas de Desarrollo Sostenible—Desarrollo Sostenible. n.d. Available online: https://www.un.org/sustainabledevelopment/es/objetivos-de-desarrollo-sostenible/ (accessed on 18 September 2022).
- Darmstadt, G.L.; A Bhutta, Z.; Cousens, S.; Adam, T.; Walker, N.; de Bernis, L. Evidence-based, cost-effective interventions: How many newborn babies can we save? Lancet 2005, 365, 977–988. [Google Scholar] [CrossRef]
- Oestergaard, M.Z.; Inoue, M.; Yoshida, S.; Mahanani, W.R.; Gore, F.M.; Cousens, S.; Lawn, J.E.; Mathers, C.D.; on behalf of the United Nations Inter-agency Group for Child Mortality Estimation and the Child Health Epidemiology Reference Group. Neonatal Mortality Levels for 193 Countries in 2009 with Trends since 1990: A Systematic Analysis of Progress, Projections, and Priorities. PLoS Med. 2011, 8, e1001080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawn, J.E.; Blencowe, H.; Oza, S.; You, D.; Lee, A.C.; Waiswa, P.; Lalli, M.; Bhutta, Z.; Barros, A.J.D.; Christian, P.; et al. Every Newborn: Progress, priorities, and potential beyond survival. Lancet 2014, 384, 189–205. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Baqui, A.H.; Arifeen, S.; Darmstadt, G.L.; Ahmed, S.; Williams, E.; Seraji, H.R.; Mannan, I.; Rahman, S.M.; Shah, R.; Saha, S.K.; et al. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: A cluster-randomised controlled trial. Lancet 2008, 371, 1936–1944. [Google Scholar] [CrossRef]
- Opiyo, N.; English, M. In-service training for health professionals to improve care of the seriously ill newborn or child in low and middle-income countries (Review). Cochrane Database Syst. Rev. 2010, 14, CD007071. [Google Scholar] [CrossRef] [Green Version]
- Ariff, S.; Lee, A.C.; Lawn, J.; Bhutta, Z.A. Global Burden, Epidemiologic Trends, and Prevention of Intrapartum-Related Deaths in Low-Resource Settings. Clin. Perinatol. 2016, 43, 593–608. [Google Scholar] [CrossRef]
- Narayanan, I.; Rose, M.; Cordero, D.; Faillace, S.; Sanghvi, T. The Components of Essential Newborn Care; Basics Support for Institutionalizing Child Survival Project for the United States Agency for International Development: Arlington, VA, USA, 2004. [Google Scholar]
- World Health Organization. Guidelines on Basic Newborn Resuscitation; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- van Heerden, C. An introduction to Helping Babies Breathe: The "Golden Minute" is here for South African newborn babies. Prof. Nurs. Today 2012, 16, 6–7. [Google Scholar]
- Steele, C. Helping Babies Breathe Around the World. J. Obstet. Gynecol. Neonatal Nurs. 2013, 42, 243–246. [Google Scholar] [CrossRef]
- Helping Babies Survive. n.d. Available online: https://www.aap.org/en/aap-global/helping-babies-survive/ (accessed on 18 September 2022).
- Carlo, W.A.; Goudar, S.S.; Pasha, O.; Chomba, E.; Wallander, J.L.; Biasini, F.J.; McClure, E.M.; Thorsten, V.; Chakraborty, H.; Wallace, D.; et al. Randomized Trial of Early Developmental Intervention on Outcomes in Children after Birth Asphyxia in Developing Countries. J. Pediatr. 2013, 162, 705–712.e3. [Google Scholar] [CrossRef] [Green Version]
- Wallander, J.L.; Bann, C.; Chomba, E.; Goudar, S.S.; Pasha, O.; Biasini, F.J.; McClure, E.M.; Thorsten, V.; Wallace, D.; Carlo, W.A. Developmental trajectories of children with birth asphyxia through 36months of age in low/low–middle income countries. Early Hum. Dev. 2014, 90, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Wall, S.N.; Lee, A.C.C.; Niermeyer, S.; English, M.; Keenan, W.J.; Carlo, W.; Bhutta, Z.A.; Bang, A.; Narayanan, I.; Ariawan, I.; et al. Neonatal resuscitation in low-resource settings: What, who, and how to overcome challenges to scale up? Int. J. Gynecol. Obstet. 2009, 107, S47–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhury, S.; Arlington, L.; Brenan, S.; Kairuki, A.K.; Meda, A.R.; Isangula, K.G.; Mponzi, V.; Bishanga, D.; Thomas, E.; Msemo, G.; et al. Cost analysis of large-scale implementation of the ’Helping Babies Breathe’ newborn resuscitation-training program in Tanzania. BMC Health Serv. Res. 2016, 16, 681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jüni, P.; Loke, Y.; Pigott, T.; Ramsay, C.; Regidor, D.; Rothstein, H.; Sandhu, L.; Santaguida, P.L.; Schünemann, H.J.; Shea, B. Risk of bias in non-randomized studies of interventions (ROBINS-I): Detailed guidance. Br. Med. J. 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Kc, A.; Ewald, U.; Basnet, O.; Gurung, A.; Pyakuryal, S.N.; Jha, B.K.; Bergström, A.; Eriksson, L.; Paudel, P.; Karki, S.; et al. Effect of a scaled-up neonatal resuscitation quality improvement package on intrapartum-related mortality in Nepal: A stepped-wedge cluster randomized controlled trial. PLoS Med. 2019, 16, e1002900. [Google Scholar] [CrossRef] [Green Version]
- Rule, A.R.; Maina, E.; Cheruiyot, D.; Mueri, P.; Simmons, J.M.; Kamath-Rayne, B.D. Using quality improvement to decrease birth asphyxia rates after ‘Helping Babies Breathe’ training in Kenya. Acta Paediatr. 2017, 106, 1666–1673. [Google Scholar] [CrossRef]
- Msemo, G.; Massawe, A.; Mmbando, D.; Rusibamayila, N.; Manji, K.; Kidanto, H.L.; Mwizamuholya, D.; Ringia, P.; Ersdal, H.L.; Perlman, J. Newborn Mortality and Fresh Stillbirth Rates in Tanzania After Helping Babies Breathe Training. Pediatrics 2013, 131, e353–e360. [Google Scholar] [CrossRef] [Green Version]
- Mduma, E.; Ersdal, H.; Svensen, E.; Kidanto, H.; Auestad, B.; Perlman, J. Frequent brief on-site simulation training and reduction in 24-h neonatal mortality—An educational intervention study. Resuscitation 2015, 93, 1–7. [Google Scholar] [CrossRef]
- Patel, A.; Bang, A.; Kurhe, K.; Bhargav, S.; Prakash, A.; Arramraj, S.; Hibberd, P.L. Comparison of perinatal outcomes in facilities before and after Global Network’s Helping Babies Breathe Implementation Study in Nagpur, India. BMC Pregnancy Childbirth 2019, 19, 324. [Google Scholar] [CrossRef] [Green Version]
- Innerdal, M.; Simaga, I.; Diall, H.; Eielsen, M.; Niermeyer, S.; Eielsen, O.; Saugstad, O.D. Reduction in Perinatal Mortality after Implementation of HBB Training at a District Hospital in Mali. J. Trop. Pediatr. 2020, 66, 315–321. [Google Scholar] [CrossRef]
- Kc, A.; Wrammert, J.; Clark, R.B.; Ewald, U.; Vitrakoti, R.; Chaudhary, P.; Pun, A.; Raaijmakers, H.; Målqvist, M. Reducing Perinatal Mortality in Nepal Using Helping Babies Breathe. Pediatrics 2016, 137, e20150117. [Google Scholar] [CrossRef] [PubMed]
- Bellad, R.M.; Bang, A.; Carlo, W.A.; McClure, E.; Meleth, S.; Goco, N.; Goudar, S.; Derman, R.; Hibberd, P.L.; Petal, A.; et al. A pre-post study of a multi-country scale up of resuscitation training of facility birth attendants: Does Helping Babies Breathe training save lives? BMC Pregnancy Childbirth 2016, 16, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrammert, J.; Kc, A.; Ewald, U.; Målqvist, M. Improved postnatal care is needed to maintain gains in neonatal survival after the implementation of the Helping Babies Breathe initiative. Acta Paediatr. 2017, 106, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Goudar, S.S.; Somannavar, M.S.; Clark, R.; Lockyer, J.M.; Revankar, A.P.; Fidler, H.M.; Sloan, N.L.; Niermeyer, S.; Keenan, W.J.; Singhal, N. Stillbirth and Newborn Mortality in India After Helping Babies Breathe Training. Pediatrics 2013, 131, e344–e352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabi, A.; Ibrahim, S.; Manar, A.; Abdalla, M.; Ahmed, S.; Dempsey, E.; Ryan, C. Perinatal outcomes following Helping Babies Breathe training and regular peer–peer skills practice among village midwives in Sudan. Arch. Dis. Child. 2018, 103, 24–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.M.; Fratt, E.M.; Rodriguez, J.; Ruman, A.; Wibecan, L.; Nelson, B.D. Implementation of the Helping Babies Breathe Training Program: A Systematic Review. Pediatrics 2020, 146, e20193938. [Google Scholar] [CrossRef]
- Versantvoort, J.M.D.; Kleinhout, M.Y.; Ockhuijsen, H.D.L.; Bloemenkamp, K.; de Vries, W.B.; Hoogen, A.V.D. Helping Babies Breathe and its effects on intrapartum-related stillbirths and neonatal mortality in low-resource settings: A systematic review. Arch. Dis. Child. 2020, 105, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Travers, C.P.; Carlo, W.A. How to Save 1 Million Lives in a Year in Low- and Middle-Income Countries. Neonatology 2017, 111, 431–436. [Google Scholar] [CrossRef]
- Hodgins, S. Helping Babies Breathe—Beyond Training. Glob. Health Sci. Pract. 2018, 6, 402–404. [Google Scholar] [CrossRef] [Green Version]
- Dempsey, E.M.; Pammi, M.; Ryan, A.C.; Barrington, K.J. Standardised formal resuscitation training programmes for reducing mortality and morbidity in newborn infants. Cochrane Database Syst. Rev. 2015, 2015, CD009106. [Google Scholar] [CrossRef]
- Dol, J.; Campbell-Yeo, M.; Murphy, G.T.; Aston, M.; McMillan, D.; Richardson, B. The impact of the Helping Babies Survive program on neonatal outcomes and health provider skills: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 701–737. [Google Scholar] [CrossRef] [PubMed]
- Budhathoki, S.S.; Gurung, R.; Ewald, U.; Thapa, J.; Kc, A. Does the Helping Babies Breathe Programme impact on neonatal resuscitation care practices? Results from systematic review and meta-analysis. Acta Paediatr. 2019, 108, 806–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, K.; Lee, H.C.; Escobedo, M.B.; Hoover, A.V.; Kamath-Rayne, B.D.; Kapadia, V.S.; Magid, D.J.; Niermeyer, S.; Schmölzer, G.M.; Szyld, E.; et al. Part 5: Neonatal Resuscitation: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S524–S550. [Google Scholar] [CrossRef] [PubMed]
- Niermeyer, S. Global gains after Helping Babies Breathe. Acta Paediatr. 2017, 106, 1550–1551. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Design | Duration of Study | Sample and Place | Objective | Intervention-Implementation Strategy | Measured Outcomes |
|---|---|---|---|---|---|---|
| Msemo 2013 Tanzania [21] | Before and after | 2 years | 86.621 (8124 before and 78,500 after) 8 hospitals in Tanzania | To determine whether the implementation of HBB improves the basic skills of those attending deliveries, including the application of mask bag ventilation, and whether it reduces early neonatal mortality by 50% and death rate. | For 6 to 9 months: The principal investigator and trainers conducted a one-day training of healthcare providers at each hospital | Overall mortality, intrapartum mortality, 24 h mortality and asphyxia |
| Mduma 2015 Tanzania [22] | Before and after | 2 years (2010–2012) | 9807 (4894 before and 4812 after) 1 hospital in Tanzania | To assess whether frequent and brief HBB simulation training would affect clinical practice and reduce 24 h neonatal mortality. | Training in FBOS HBB simulation. One-day trainings for everyone who works in the delivery room. Monthly training sessions of 40 min duration. The practical sessions focused on the immediate basic care of stabilization and resuscitation intervention. | Overall mortality, intrapartum mortality, 24 h mortality |
| Rule 2017 Kenya [20] | Before and after | 21 months (1/2014–9/2015) | 4117 (2106 before and 2011 after) 1 hospital in Bomet, Kenya | Describe a study that uses quality improvement. The hospital’s Neonatal Task Force identified high rates of asphyxia at birth (BA) as a quality gap. With the implementation of HBB, they sought to reduce hospital BA rates by 50% over a six-month period. | An HBB coach joined the team for one year to train its members in the HBB methodology. Prior to initial training, reference practices in the delivery room were observed, staff members were interviewed, and task force members were trained as HBB teachers. | Asphyxia |
| Patel 2019 India [23] | Before and after | 2 years (2011–2013) | 78,948 (38,078 before and 40,870 after) 13 hospitals in Nagpur, India | To assess perinatal mortality at day 1 in facility deliveries before and after HBB implementation | HBB training of instructors who then trained birth attendants, introduction of a multifaceted follow-up program, and retraining of delivery attendants after six months. They were instructed to reanimate all non-macerated births, including those considered fresh stillbirths. | Overall mortality, intrapartum mortality, 24 h mortality |
| Innerdal 2019 Mali [24] | Before and after | 3 years (2015–2018) | 9769 (3125 before and 6644 after) 1 hospital in Mali and 13 district health centers. | Reduce neonatal mortality in Mali by introducing HBB. | The implementation of the first edition of HBB was 44 sessions, of 1 or 2 days. The evaluation of the training was carried out with a written test before and after the sessions. Then they trained in the second edition of HBB with a duration of 2 to 3 days and weekly repetition training was introduced. | Overall mortality, intrapartum mortality, 24 h mortality |
| KC et al., 2019 Nepal [19] | Randomized controlled trial | 18 months (4/2017–10/2018) | 89.014 (control 38.378, intervention 50,636) 12 public hospitals in Nepal | Phased implementation of a quality improvement package for neonatal resuscitation (HBB) in hospitals in Nepal | Implementation of a quality improvement package in neonatal resuscitation that includes facilitation strategies, training, weekly meetings, and information dissemination visits. | Intrapartum mortality, 24 h mortality, early mortality |
| KC et al., 2016 Nepal [25] | Prospective cohort study | 14 months (7/2012–9/2013) | 25,108 (control 9588, intervention 15,520) 1 tertiary hospital in Nepal | Improve adherence to the Helping Babies Breathe neonatal resuscitation protocol by using a quality improvement cycle | HBB protocol training, weekly review meetings, daily skills checks, use of self-assessment checklists, and refresher training. | Overall mortality, intrapartum mortality, 24 h mortality |
| Bellad et al., 2016 India y Kenia [26] | Before and after | 24 months (1/2011–10/2013) | 70,704 (before 35,595 and then 35,109) Belgaum: 33 centers Nagpur: 15 centers Kenya: 23 centers | To assess the impact of implementing a package of HBB interventions and monitoring in select health facilities representing a large proportion of births and perinatal mortality rate at sites in India and Kenya | Master trainer training and training of childbirth care teams. It included assessment of HBB knowledge and skills before and after training courses and updates 6 months later. | Overall mortality, intrapartum mortality, 24 h mortality, early mortality. |
| Wrammert J. et al., 2017 Nepal [27] | prospective cohort study | 15 months (7/2012–9/2013) | 24,665 (control 9390 and intervention 15,275) 1 tertiary hospital in Kathmandu | Describe the timing and causes of neonatal deaths in hospital before and after HBB training at a maternity health center in Nepal | Evaluation of the effect of HBB training on neonatal mortality rates | General mortality, 24 h mortality, early mortality, late mortality. |
| Goudar et al., 2013 India [28] | Before and after | 11 months (10/2009–09/2010) | 9598 (before 4187 and then 5411) District hospitals in Karnataka, India, and urban hospitals in Belgaum | To assess the efficacy of HBB training in reducing stillbirths and neonatal mortality rate | Model of training and teaching and skills and practice, coaches were trained, including discussion, practice, and simulation. Training to trainers was continued and learning assessments were applied. | Overall mortality, intrapartum mortality, late mortality. |
| Arabi AME, et al., 2017 Sudan [29] | Before and after | 24 months | 4390 (before 1350 and after 4390) 6 rural medical centers in east Nile | Community-based intervention (village midwives) to assess the impact of HBB on neonatal mortality | Trainers at HBB instructed midwives, included simulator training kit and teaching materials, then weekly post-HBB follow-up | Intrapartum mortality, early mortality |
| Article/Domain | Confusion | Participants Selection | Classification of Interventions | Deviations and Interventions | Lack of Data | Measurement of Results | Result Selection Reported | Global | Risk |
|---|---|---|---|---|---|---|---|---|---|
| Ashish KC 2016 [25] | Moderate | ||||||||
| Bellad et al., 2016 [26] | Serious | ||||||||
| Wrammert et al., 2017 [27] | Critical | ||||||||
| Goudar et al., 2013 [28] | Serious | ||||||||
| Ashish KC 2019 [19] | Moderate | ||||||||
| Arabi AME, et al., 2017 [29] | Moderate | ||||||||
| Msemo G, et al., 2013 [21] | Moderate | ||||||||
| Patel A, et al., 2019 [23] | Moderate | ||||||||
| Rule AL, et al., 2017 [20] | Serious | ||||||||
| Innerdal M, et al., 2019 [24] | Serious | ||||||||
| Mduma E, et al., 2015 [22] | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agudelo-Pérez, S.; Cifuentes-Serrano, A.; Ávila-Celis, P.; Oliveros, H. Effect of the Helping Babies Breathe Program on Newborn Outcomes: Systematic Review and Meta-Analysis. Medicina 2022, 58, 1567. https://doi.org/10.3390/medicina58111567
Agudelo-Pérez S, Cifuentes-Serrano A, Ávila-Celis P, Oliveros H. Effect of the Helping Babies Breathe Program on Newborn Outcomes: Systematic Review and Meta-Analysis. Medicina. 2022; 58(11):1567. https://doi.org/10.3390/medicina58111567
Chicago/Turabian StyleAgudelo-Pérez, Sergio, Annie Cifuentes-Serrano, Paula Ávila-Celis, and Henry Oliveros. 2022. "Effect of the Helping Babies Breathe Program on Newborn Outcomes: Systematic Review and Meta-Analysis" Medicina 58, no. 11: 1567. https://doi.org/10.3390/medicina58111567